Another article came out that is suggesting that ventilation doesn’t work in classrooms.
Does it actually showthat?
No.
Does it find out anything new?
Also, no.
Straw Man Science? Most definitely.
Let’s get into this 🧵
Does it actually showthat?
No.
Does it find out anything new?
Also, no.
Straw Man Science? Most definitely.
Let’s get into this 🧵
Context: Air filtration has been argued as an effective means to limit airborne disease transmission. Like any physical intervention of transmission, the effectiveness will depend on how it is used
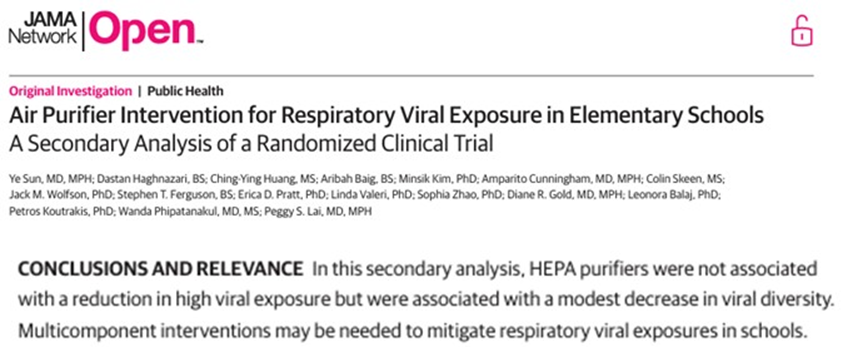
In this study, they put air filters in classrooms and measured transmission rates
In this study, they put air filters in classrooms and measured transmission rates

Each classroom was fitted with 4 HEPA filters that deliver at 3000 L/min.

While 12,000 L/min sounds like a lot, is it?
ASHRAE advises a minimum ventilation rate of 20 L/s/person.
So, let’s do some math:
30 people -> 20 L/s/person *30 person = 600 L/s
600 L/s * 60 s/min = 36,000 L/min
ASHRAE advises a minimum ventilation rate of 20 L/s/person.
So, let’s do some math:
30 people -> 20 L/s/person *30 person = 600 L/s
600 L/s * 60 s/min = 36,000 L/min

Meaning, that the ventilation rate used in the study was about 1/3 of what it would need to be for one to expect a significant drop in transmission (according to the ASHRAE 241 guidelines).
Based on how the study is designed, one WOULD NOT EXPECT to see much.
Based on how the study is designed, one WOULD NOT EXPECT to see much.
And indeed, they found no effect.
This is entirely expected and unsurprising.
However, it is presented as though filtration itself is not effective.
This is entirely expected and unsurprising.
However, it is presented as though filtration itself is not effective.
It is telling that the ASHRAE guidance was not mentioned in the article. Given that many of the authors were American, this is surprising.

The aim of the article is to determine if air filtration is effective at lowering transmission rates. The authors ought to have checked to see if the values they’ve selected would be expected to lower the rate. At the very least, they should provide the reader with context.
It should be noted that it has already been shown that once the ventilation is high enough, a reduction in transmission will be observed.
frontiersin.org/journals/publi…
frontiersin.org/journals/publi…

The conclusion of the current study ought to have been:
“When filtration/ventilation rates are lower than the ASHRAE 241 suggests, the effects on transmission are not significant.”
This of course, is not surprising, nor does it get headlines.
“When filtration/ventilation rates are lower than the ASHRAE 241 suggests, the effects on transmission are not significant.”
This of course, is not surprising, nor does it get headlines.

THIS IS A PROBLEM
This article tells us something we already know, and is presented like it’s something new
It’s not
In order to reduce transmission rates, we have a very good idea of what is required. Less than that is not enough.
This article tells us something we already know, and is presented like it’s something new
It’s not
In order to reduce transmission rates, we have a very good idea of what is required. Less than that is not enough.
I can’t stress this enough. The conclusion that this study supports the ASHRAE requirements would have been useful to promote and discuss.
It shows that:
- The people who made the guidelines know what they are talking about
- We have a good understanding of what is needed
It shows that:
- The people who made the guidelines know what they are talking about
- We have a good understanding of what is needed
This article is another fine example of “Straw Man Science”. I’ve described this kind of study in a previous thread.
https://x.com/ukhadds/status/1955675711936581742
In short, it’s incredibly easy to design studies to “prove” that physical mitigation strategies don’t work.
The conclusion of this study is akin to saying that hard hats don’t protect the user because a person wearing one still got injured when a car was dropped on them.

Air filtration is always a good thing.
While in this study it was not high enough to limit transmission spread, it will be enough to lower student’s exposure to other pollutants that may have other effects. This helps. Over the long term, it helps a lot.
While in this study it was not high enough to limit transmission spread, it will be enough to lower student’s exposure to other pollutants that may have other effects. This helps. Over the long term, it helps a lot.
It would be a tragedy if people were to use this study to argue against better indoor air quality in schools.
Anyway, hoped you found that useful.
• • •
Missing some Tweet in this thread? You can try to
force a refresh