🧵The best clinicians diagnose before the investigations arrive.
Here are 100 timeless history-taking gems from Hutchison’s Clinical Methods (25th Edition) — distilled into pure bedside wisdom.
🩺 This thread reminds us why the story still matters more than the scan 👇
(Bookmark this — it’ll shape your next patient encounter.)
@DrAkhilX @IhabFathiSulima @drkeithsiau @RheumNow @Janetbirdope #MedTwitter #MedEd #FOAMed #Medicine #internalmedicine
Here are 100 timeless history-taking gems from Hutchison’s Clinical Methods (25th Edition) — distilled into pure bedside wisdom.
🩺 This thread reminds us why the story still matters more than the scan 👇
(Bookmark this — it’ll shape your next patient encounter.)
@DrAkhilX @IhabFathiSulima @drkeithsiau @RheumNow @Janetbirdope #MedTwitter #MedEd #FOAMed #Medicine #internalmedicine
The Art of Beginning
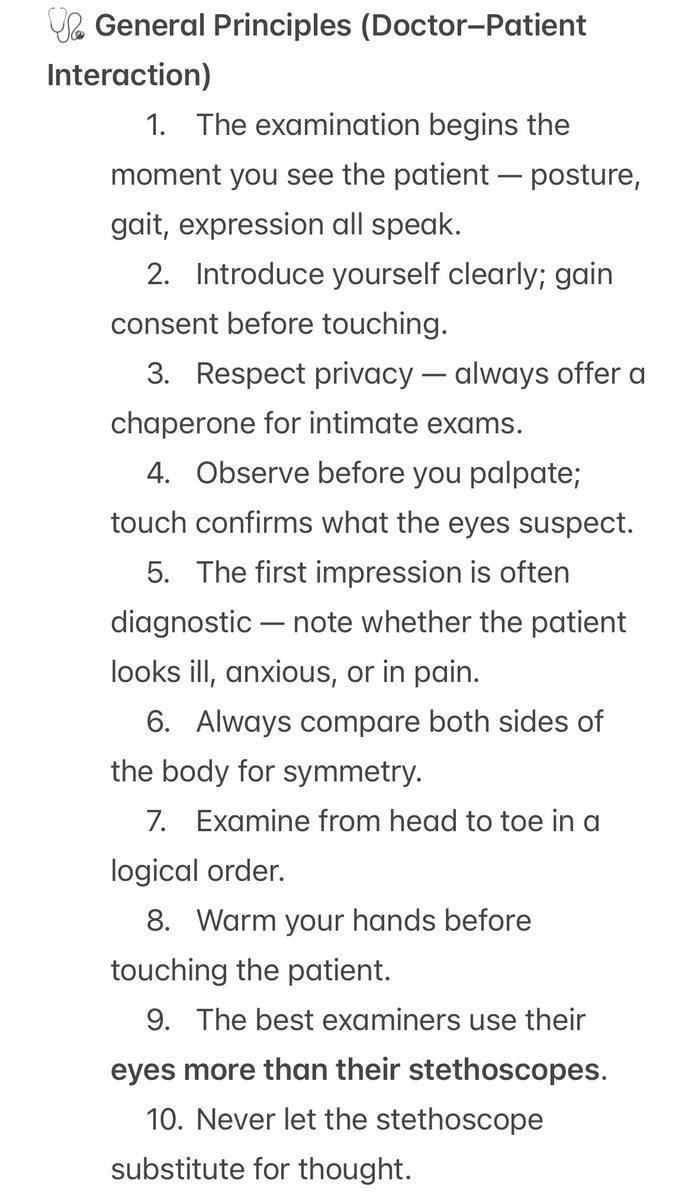
1️⃣ The history starts before you speak.
Observe posture, mood, breathing, gait — the body always speaks first.
Then say softly:
“Tell me about your problem.”
Silence in the first 30 seconds is golden.
1️⃣ The history starts before you speak.
Observe posture, mood, breathing, gait — the body always speaks first.
Then say softly:
“Tell me about your problem.”
Silence in the first 30 seconds is golden.
Chief Complaint
2️⃣ Always in the patient’s own words.
“I feel tired for 2 weeks” > “Fatigue × 2 weeks.”
Ask: “What troubles you most?”
The answer guides the whole consultation.
2️⃣ Always in the patient’s own words.
“I feel tired for 2 weeks” > “Fatigue × 2 weeks.”
Ask: “What troubles you most?”
The answer guides the whole consultation.
Pain
3️⃣ Pain has a story — location, radiation, character, severity, timing.
“Point with one finger.”
Sharp = somatic.
Dull = visceral.
Burning = neuropathic.
The pattern defines the pathology.
3️⃣ Pain has a story — location, radiation, character, severity, timing.
“Point with one finger.”
Sharp = somatic.
Dull = visceral.
Burning = neuropathic.
The pattern defines the pathology.
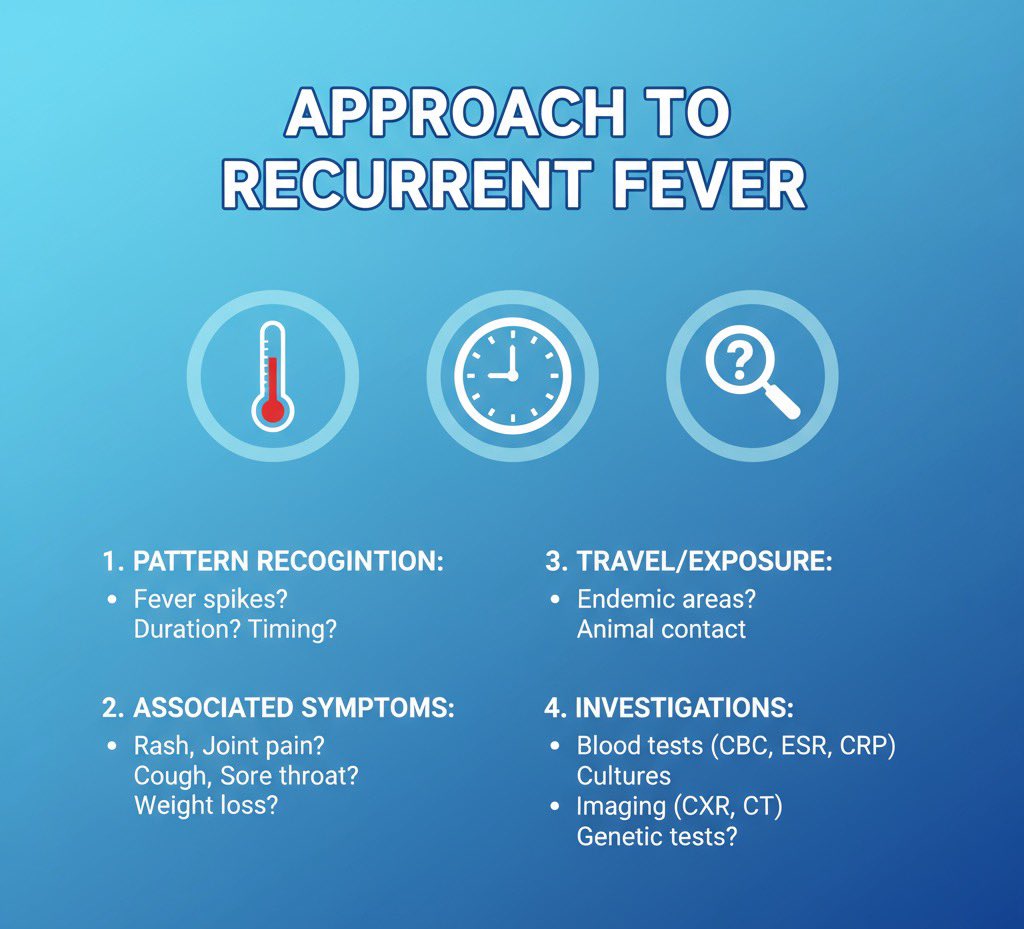
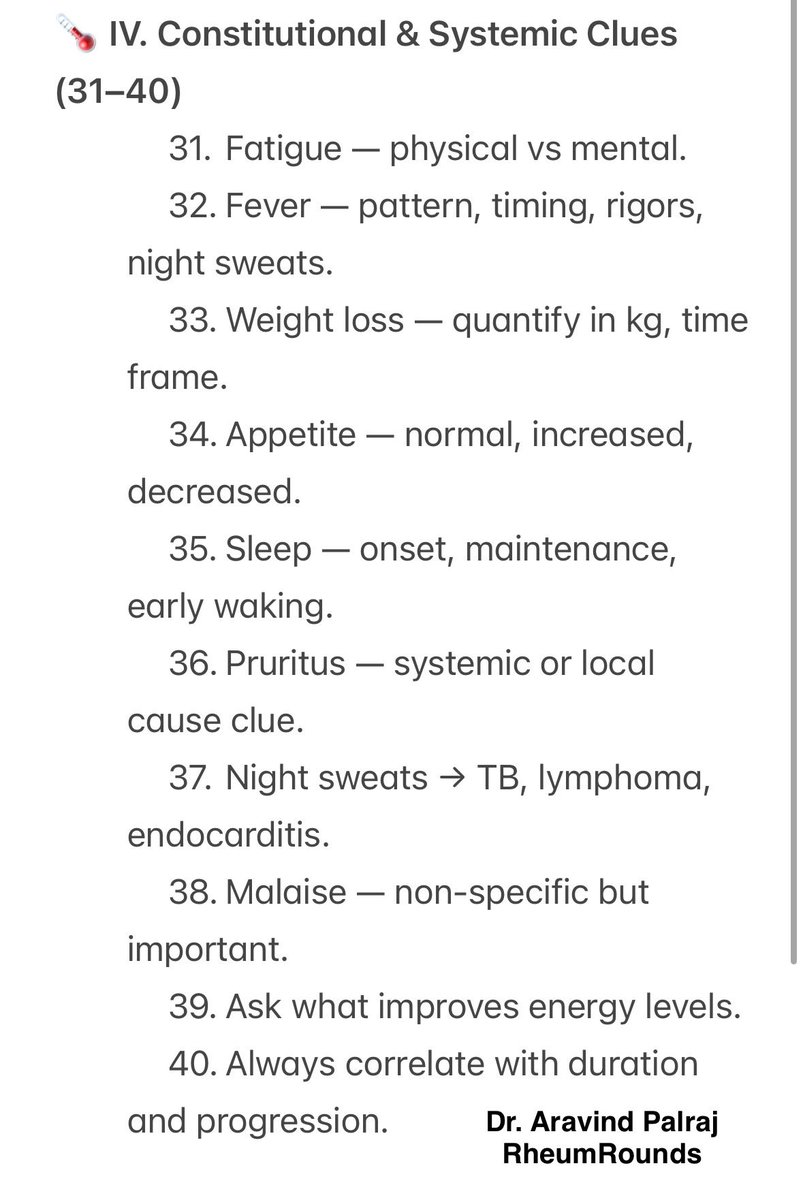
Fever, Fatigue, Weight Loss
4️⃣ Never skip constitutional symptoms.
Fever patterns whisper the diagnosis.
🔹 Evening fever → TB
🔹 Intermittent rigors → malaria
🔹 Night sweats → lymphoma
Weight loss? Always quantify it.
4️⃣ Never skip constitutional symptoms.
Fever patterns whisper the diagnosis.
🔹 Evening fever → TB
🔹 Intermittent rigors → malaria
🔹 Night sweats → lymphoma
Weight loss? Always quantify it.
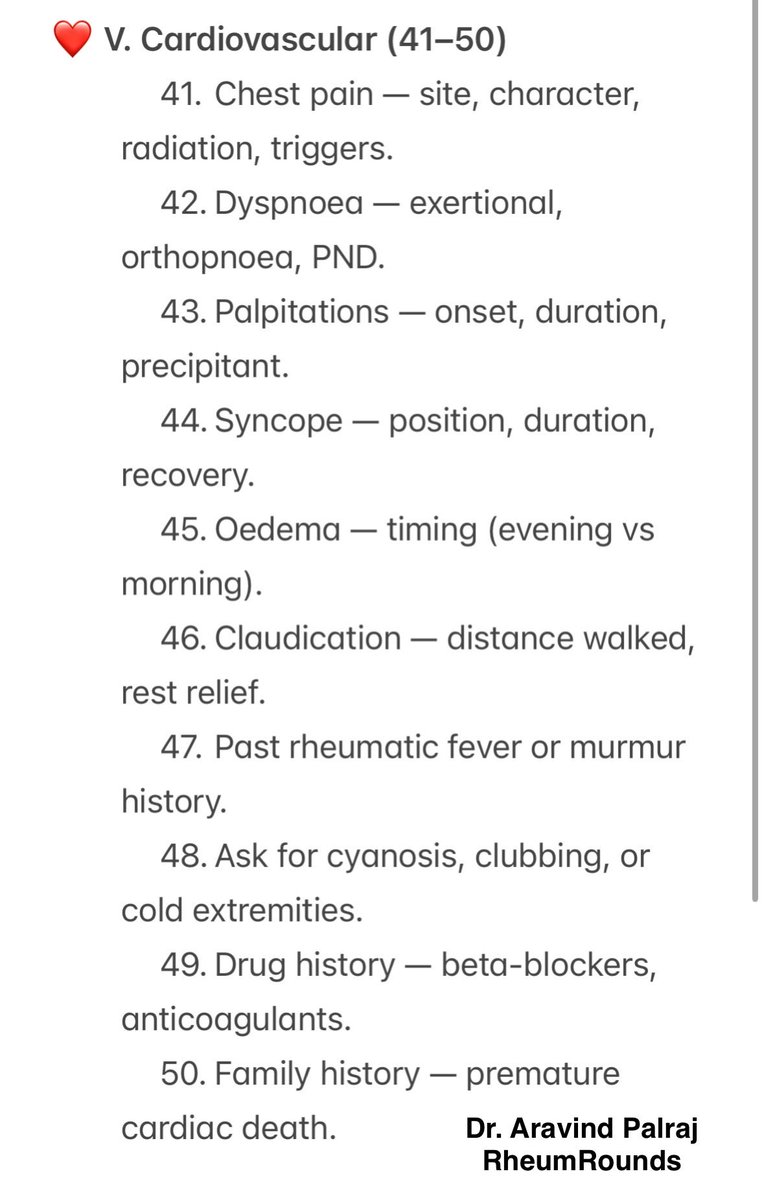
Cardiovascular
5️⃣ Chest pain, dyspnoea, palpitation, syncope, oedema.
The “Big Five” cardiac questions.
Ask:
“How far can you walk before breathlessness?”
That’s better than any NYHA class.
5️⃣ Chest pain, dyspnoea, palpitation, syncope, oedema.
The “Big Five” cardiac questions.
Ask:
“How far can you walk before breathlessness?”
That’s better than any NYHA class.
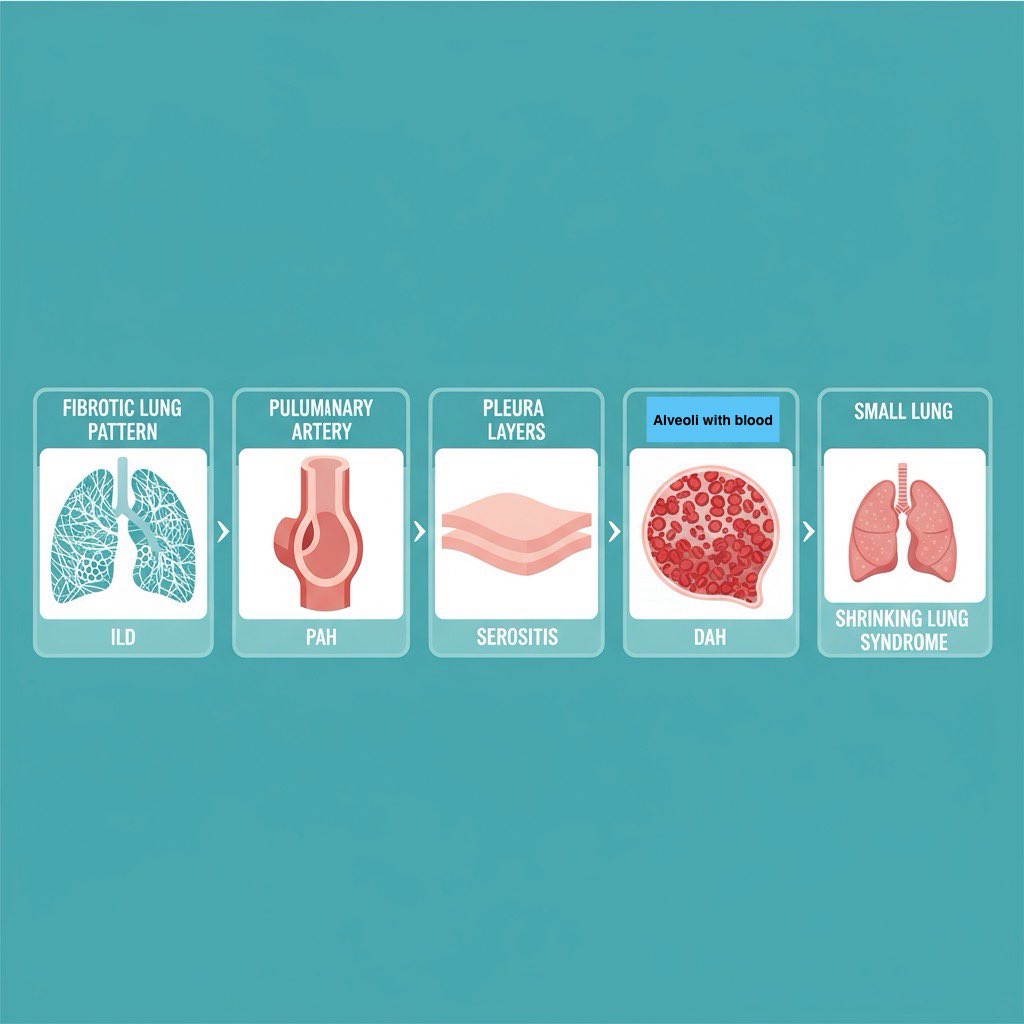
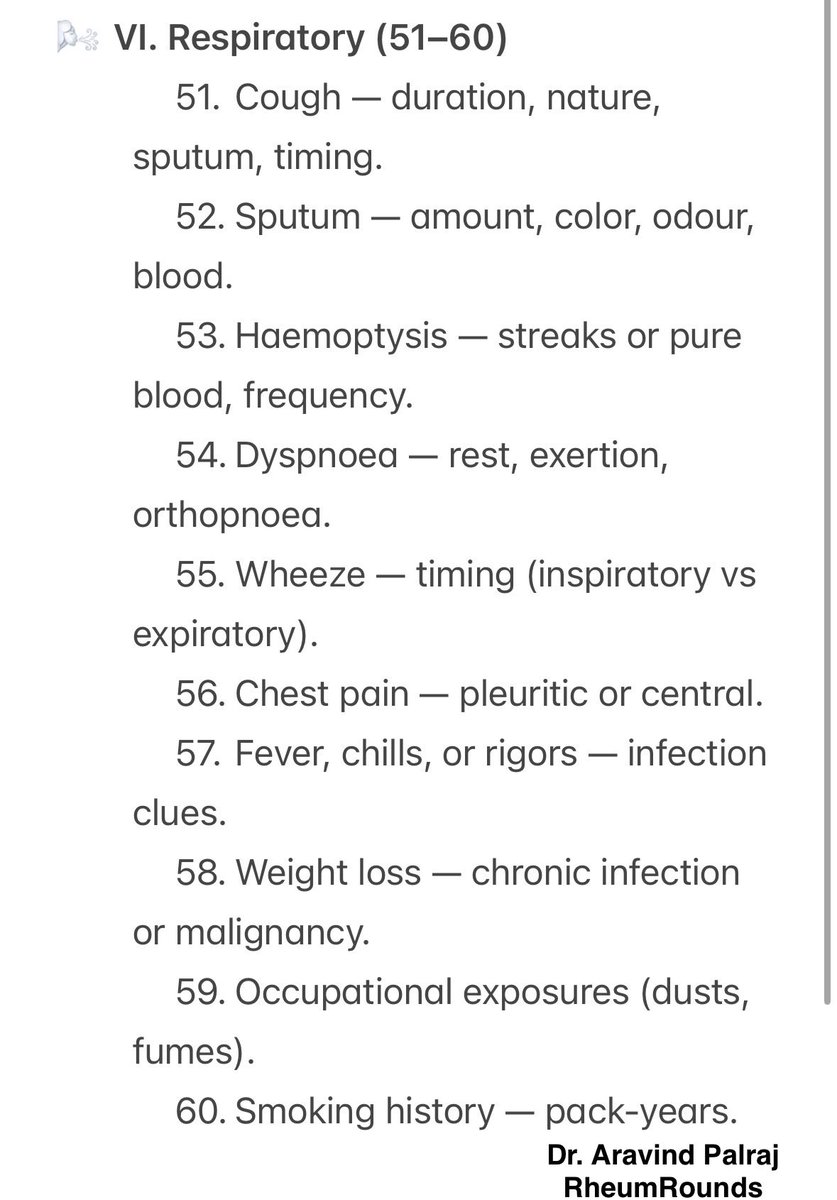
Respiratory
6️⃣ Cough and sputum are storytellers.
Color, quantity, timing.
Morning = bronchitis, nocturnal = asthma.
Haemoptysis?
“How much? Fresh or streaked?”
The words decide urgency.
6️⃣ Cough and sputum are storytellers.
Color, quantity, timing.
Morning = bronchitis, nocturnal = asthma.
Haemoptysis?
“How much? Fresh or streaked?”
The words decide urgency.
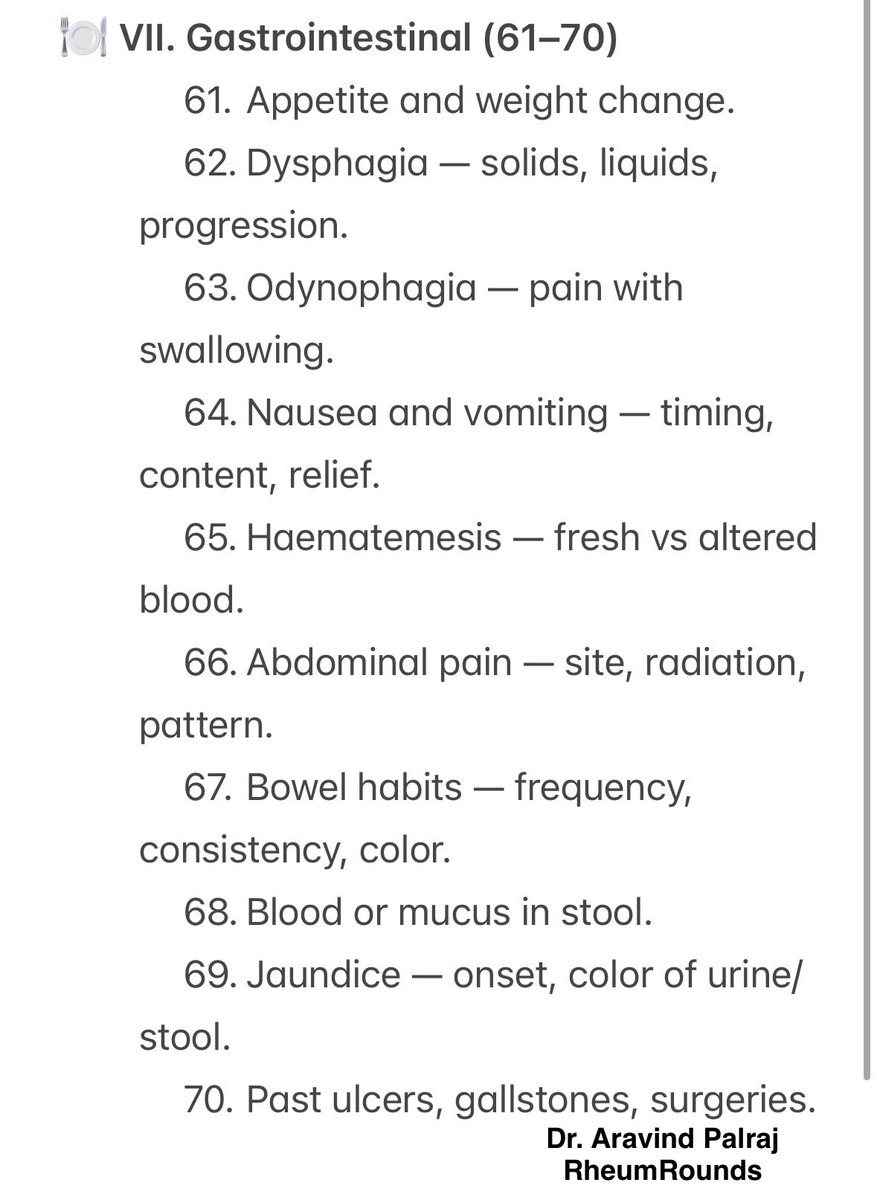
Gastrointestinal
7️⃣ Appetite, nausea, vomiting, bowel, bleed.
Ask: “Any change in food taste or smell?”
(An early hepatic or uremic clue.)
Blood in stool → ask color first.
Black ≠ red ≠ same disease.
7️⃣ Appetite, nausea, vomiting, bowel, bleed.
Ask: “Any change in food taste or smell?”
(An early hepatic or uremic clue.)
Blood in stool → ask color first.
Black ≠ red ≠ same disease.
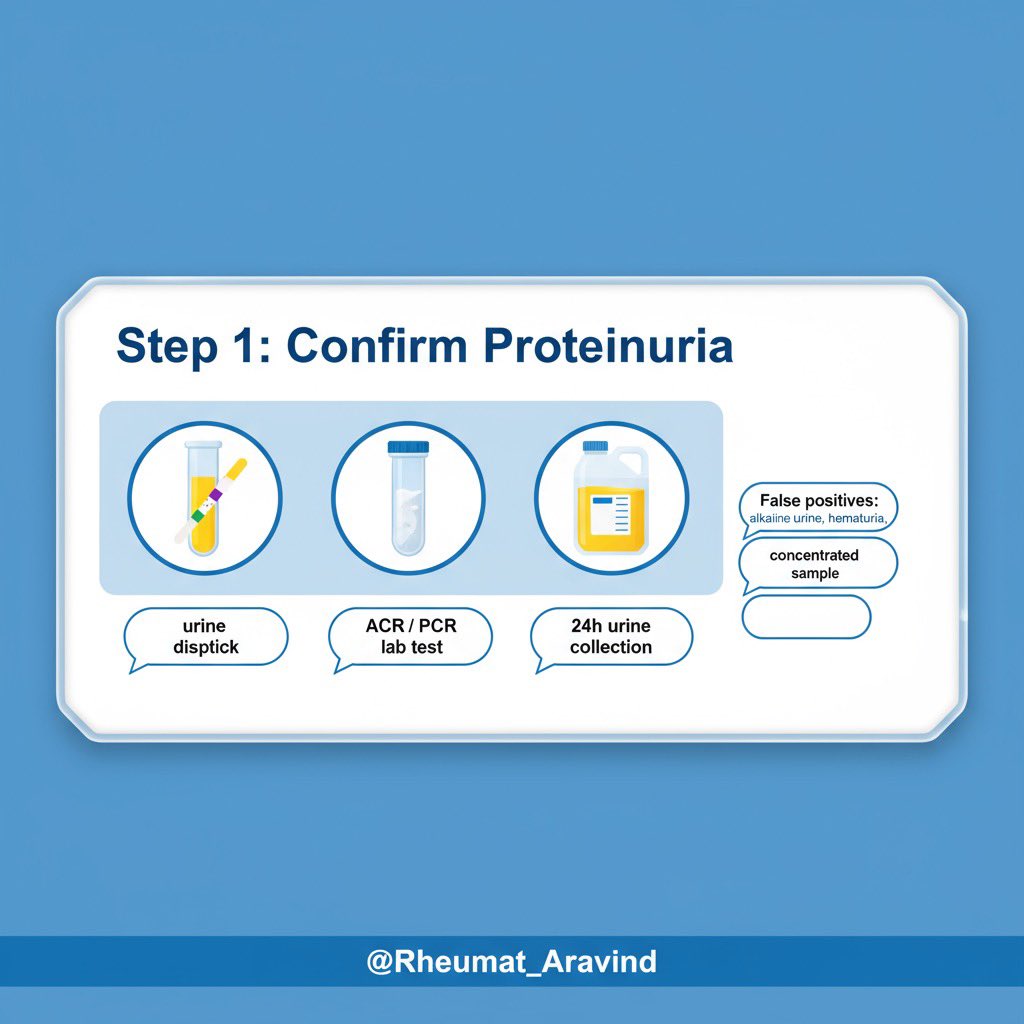
Genitourinary
8️⃣ Frequency, urgency, dysuria, hematuria.
“When in the stream do you see blood?”
▪️ Beginning → urethra
▪️ End → bladder neck
▪️ Throughout → renal
These 10 seconds save 3 tests.
8️⃣ Frequency, urgency, dysuria, hematuria.
“When in the stream do you see blood?”
▪️ Beginning → urethra
▪️ End → bladder neck
▪️ Throughout → renal
These 10 seconds save 3 tests.
Neurological
9️⃣ The nervous system whispers.
Ask for headache, vision, speech, weakness, sensation, balance.
“Any double vision?” → localizes before you touch a reflex hammer.
9️⃣ The nervous system whispers.
Ask for headache, vision, speech, weakness, sensation, balance.
“Any double vision?” → localizes before you touch a reflex hammer.
Musculoskeletal
🔟 Joint pain — site, symmetry, swelling, stiffness.
Morning stiffness > 30 mins → inflammatory.
Evening pain → mechanical.
Ask what the patient can’t do anymore.
That’s functional disability — Hutchison’s gold standard.
🔟 Joint pain — site, symmetry, swelling, stiffness.
Morning stiffness > 30 mins → inflammatory.
Evening pain → mechanical.
Ask what the patient can’t do anymore.
That’s functional disability — Hutchison’s gold standard.
Integration & Insight
💯 Every symptom has a context.
Sequence. Duration. Progression. Impact.
“When did you last feel completely well?” — the most diagnostic question of all.
#MedTwitter #Hutchison #ClinicalMethods #BedsideMedicine #RheumRounds
💯 Every symptom has a context.
Sequence. Duration. Progression. Impact.
“When did you last feel completely well?” — the most diagnostic question of all.
#MedTwitter #Hutchison #ClinicalMethods #BedsideMedicine #RheumRounds
• • •
Missing some Tweet in this thread? You can try to
force a refresh