PUPIL ATTENDANCE & ILLNESS
The government & media seem to believe that the significant rise in pupil absence compared to pre-pandemic is primarily driven by truancy.
They don’t seem to believe there is a GENUINE increase in illness.
So let’s take a closer look at the data… 🔎
The government & media seem to believe that the significant rise in pupil absence compared to pre-pandemic is primarily driven by truancy.
They don’t seem to believe there is a GENUINE increase in illness.
So let’s take a closer look at the data… 🔎

This chart shows emergency admissions for children with lower respiratory tract infections, broken down by school-age year group.
I’ve compared the 5 years before the pandemic started (2014/15 - 2018/19) to 2023/24 (most recent data published).
Do you notice anything?
I’ve compared the 5 years before the pandemic started (2014/15 - 2018/19) to 2023/24 (most recent data published).
Do you notice anything?

The data is taken from the NHS Outcomes Framework.
It specifically charts Indicator 3.2: “Emergency admissions for children with lower respiratory tract infections (LRTIs)”.
You can find the raw data here:
digital.nhs.uk/data-and-infor…
It specifically charts Indicator 3.2: “Emergency admissions for children with lower respiratory tract infections (LRTIs)”.
You can find the raw data here:
digital.nhs.uk/data-and-infor…

Indicator 3.2 is basically a measure of how many children are admitted to hospital as an emergency due to respiratory infections.
It doesn’t separate out which infection caused the admission.
It’s an umbrella measure and the underlying cause could include Covid, flu, RSV etc.
It doesn’t separate out which infection caused the admission.
It’s an umbrella measure and the underlying cause could include Covid, flu, RSV etc.
This is important, because it means that this measure is not affected by higher or lower levels of testing for illnesses like Covid or flu in hospital.
This measure is purely about admissions, not positive tests.
This measure is purely about admissions, not positive tests.
A child will only be counted under indicator 3.2 if:
1️⃣ They are sick enough to need emergency hospital care.
2️⃣ Their hospital records show a lower respiratory tract infection.
So the trend is driven by illness severity and hospitalisation rates, NOT by testing behaviour.
1️⃣ They are sick enough to need emergency hospital care.
2️⃣ Their hospital records show a lower respiratory tract infection.
So the trend is driven by illness severity and hospitalisation rates, NOT by testing behaviour.
The raw data breaks it out by every year group from babies up to 18 year olds.
For the purposes of the discussion about pupil attendance in schools, I’ve zoomed in on school-age children from age 4-16 years.
For the purposes of the discussion about pupil attendance in schools, I’ve zoomed in on school-age children from age 4-16 years.
Data during the early pandemic years was heavily affected by lockdowns & pandemic mitigations which worked well to control the spread of *all* airborne respiratory viruses.
But as mitigations have been steadily abandoned, year-by-year, there’s been a dramatic step-change.
But as mitigations have been steadily abandoned, year-by-year, there’s been a dramatic step-change.

In order to illustrate the dramatic step-change between the pre-pandemic period & 2023/24 (most recent published year), I’ve removed the first 3 pandemic years in this version of the chart.
It tells a concerning story…
It tells a concerning story…

For primary age kids, the step-change is particularly dramatic.
For example, here’s the raw data for 6 yr olds ⬇️
Pre-pandemic, rates of emergency hospitalisations for LRTIs for 6 yr olds fluctuated between ~60-80.
In 2023/24, that rate had soared to 140, ie. roughly DOUBLE.
For example, here’s the raw data for 6 yr olds ⬇️
Pre-pandemic, rates of emergency hospitalisations for LRTIs for 6 yr olds fluctuated between ~60-80.
In 2023/24, that rate had soared to 140, ie. roughly DOUBLE.

Of course, this data is only showing the MOST serious cases: the school children who were so poorly they had to be admitted to hospital as an emergency admission.
For each hospitalisation, there will be many more children who are very ill but not ill enough to require hospital.
For each hospitalisation, there will be many more children who are very ill but not ill enough to require hospital.
If hospital admissions of school age children with lower respiratory tract infections has risen so dramatically, it’s extremely likely that respiratory illnesses which *didn’t* require hospital will have risen by a similar percentage.

LRTI data for 2024/25 hasn’t been published yet, but last winter was dominated by a ‘tidal wave’ of four respiratory viruses (flu, Covid, RSV & norovirus) each surging more heavily and earlier than expected.
It placed unprecedented pressure on healthcare & education systems.
It placed unprecedented pressure on healthcare & education systems.

Last year, test positivity rates for flu in school-age children (5-14 year olds) were HIGHER in almost every week than any other age group.
The flu surge also started rising earlier in school-age children last year, as soon as the temperatures started to drop in late October.
The flu surge also started rising earlier in school-age children last year, as soon as the temperatures started to drop in late October.

Of course, when temperatures drop, windows in classrooms are kept firmly shut…
…and, as a direct consequence, ventilation rates plummet, making classrooms the perfect super-spreader environment for highly infectious airborne illnesses.
…and, as a direct consequence, ventilation rates plummet, making classrooms the perfect super-spreader environment for highly infectious airborne illnesses.

A recent study (conducted by SAMHE) revealed that ventilation rates in the majority of classrooms fall to appallingly low levels during periods of colder weather.
It’s little wonder that airborne illnesses spread like wildfire through schools in winter.
samhe.org.uk/recommendations
It’s little wonder that airborne illnesses spread like wildfire through schools in winter.
samhe.org.uk/recommendations

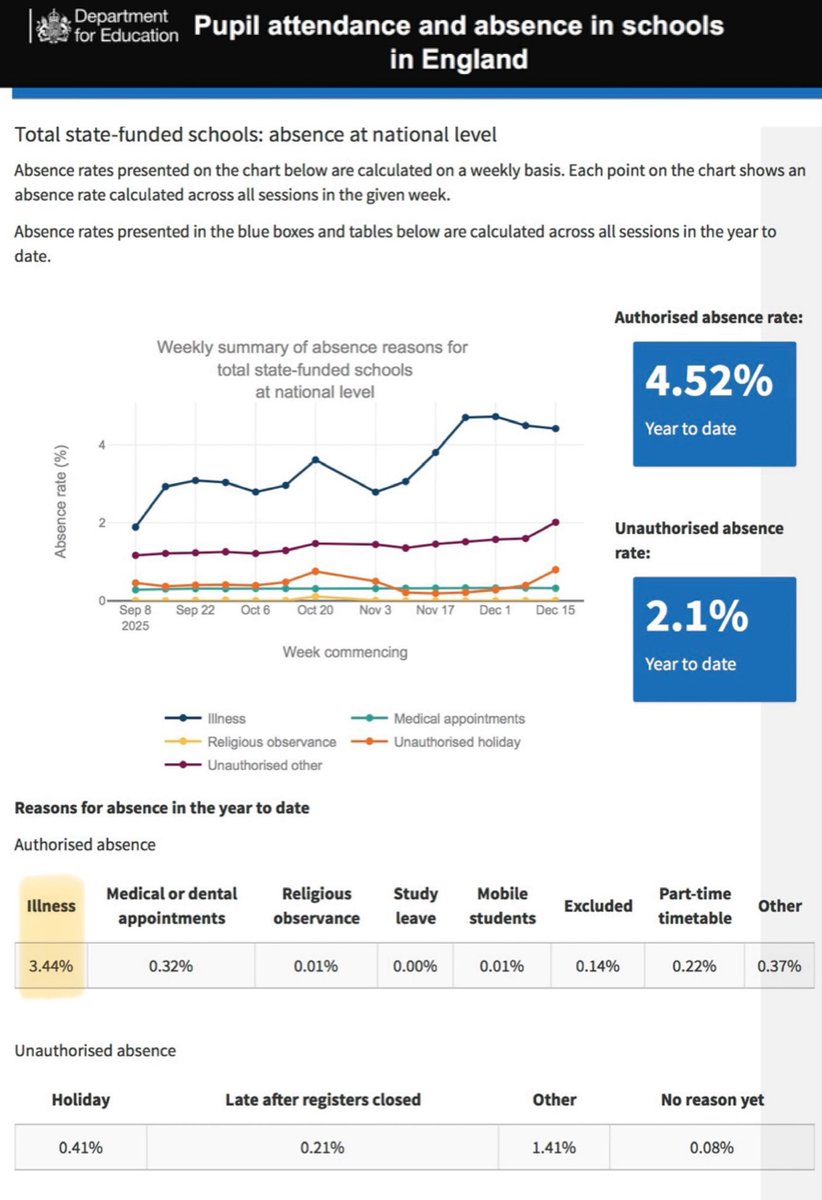
So far THIS academic year, we’ve already had a big wave of Covid.
Of course, Covid is a new illness which didn’t even exist before 2020 - it’s been added to the mix, on top of all the usual illnesses, so it’s not surprising that illness absences are higher now than pre-pandemic.
Of course, Covid is a new illness which didn’t even exist before 2020 - it’s been added to the mix, on top of all the usual illnesses, so it’s not surprising that illness absences are higher now than pre-pandemic.

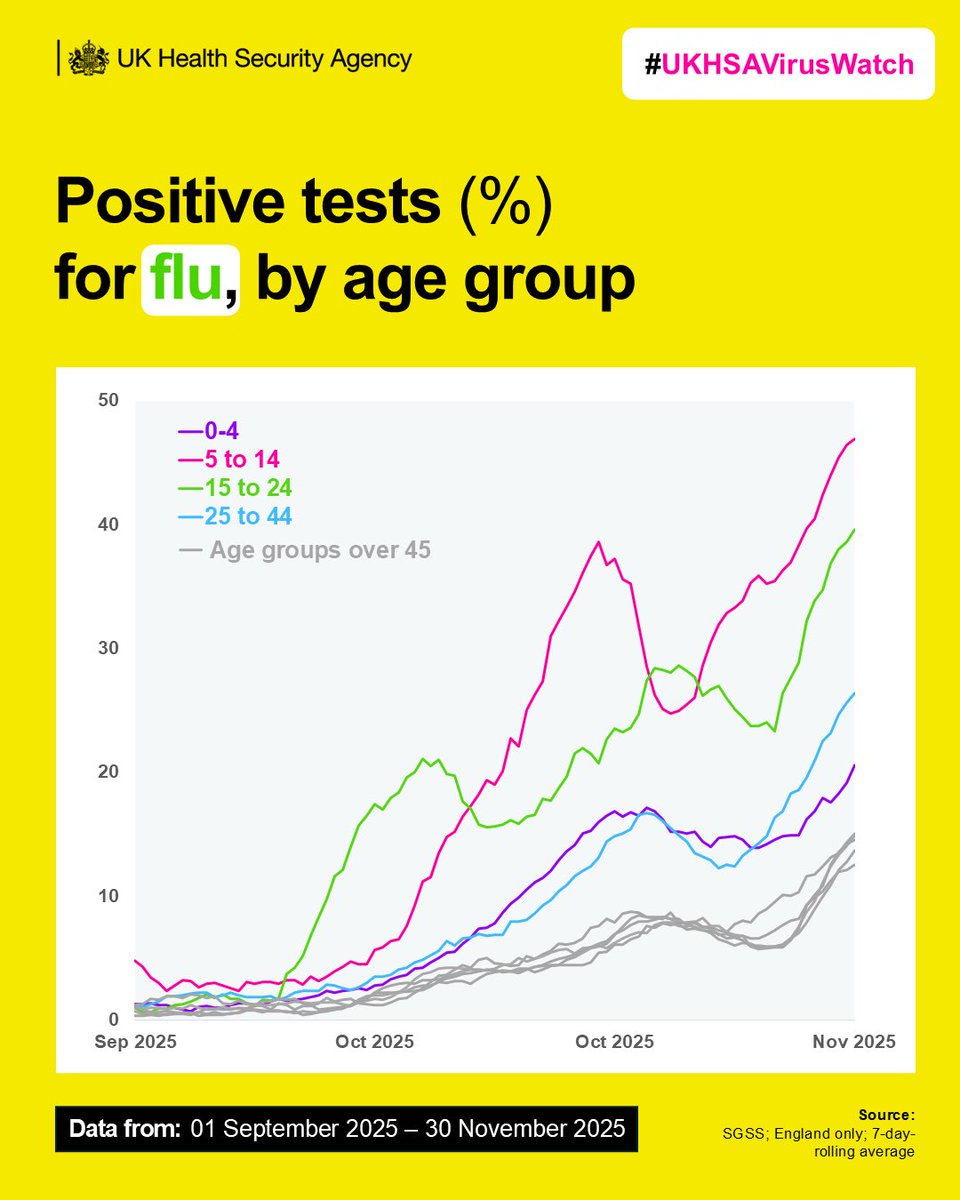
And, just in the last few days, the media has been awash with warnings from experts that this flu season may be the UK’s ‘worst in decades’.
Flu season also kicked off even earlier this year compared to last year, with cases starting to rise from early October.
Flu season also kicked off even earlier this year compared to last year, with cases starting to rise from early October.

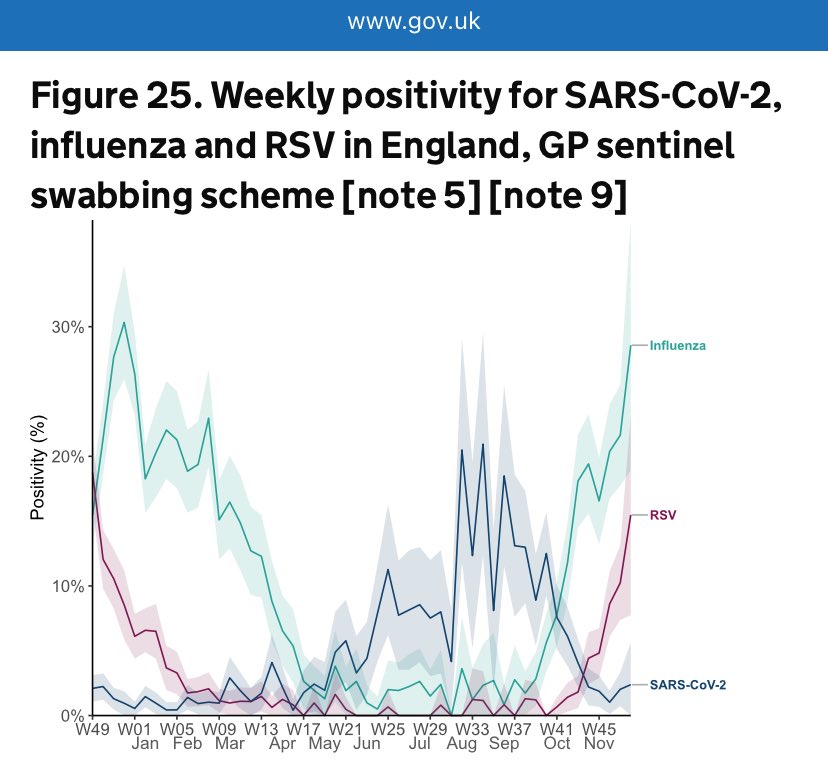
The chart below shows flu test positivity rates (%) across different age groups.
Rates have sky-rocketed in school-age children aged 5-14 years old.
Data only goes up to mid-Oct & already it’s nearly as high as last year’s peak (which wasn’t until early Dec) for this age group.
Rates have sky-rocketed in school-age children aged 5-14 years old.
Data only goes up to mid-Oct & already it’s nearly as high as last year’s peak (which wasn’t until early Dec) for this age group.

But it’s not just Covid & flu driving the recent issues with pupil illness absence...
There have also been huge outbreaks of other highly infectious airborne illnesses like PERTUSSUS (whooping cough) and MEASLES in recent years.
(Charts from UKHSA)
There have also been huge outbreaks of other highly infectious airborne illnesses like PERTUSSUS (whooping cough) and MEASLES in recent years.
(Charts from UKHSA)

And here’s the UKHSA charts for NOROVIRUS (winter vomiting
bug)…
During the 2024/25 norovirus season, lab-confirmed norovirus cases in England were 124% higher than the 5-season average* for the same period.
(* Note: 2019/2020-2021/2022 are excluded from the 5-season average)
bug)…
During the 2024/25 norovirus season, lab-confirmed norovirus cases in England were 124% higher than the 5-season average* for the same period.
(* Note: 2019/2020-2021/2022 are excluded from the 5-season average)

And ROTAVIRUS…
Rotavirus is the most common cause of diarrhoeal disease in young
children.
During the 2024/25 season, lab-confirmed rotavirus cases were 46% higher than the 5-season
average* for the same period.
(* Note: 2019/2020-2021/2022 are excluded from 5-season average)
Rotavirus is the most common cause of diarrhoeal disease in young
children.
During the 2024/25 season, lab-confirmed rotavirus cases were 46% higher than the 5-season
average* for the same period.
(* Note: 2019/2020-2021/2022 are excluded from 5-season average)

These unusually high levels of both norovirus & rotovirus translate into more gastrointestinal illness among children, which inevitably leads to increased school absences and operational disruptions (e.g., classroom closures, clean-ups).
Official DfE guidelines state that children with diarrhoea & vomiting should stay off school for 48 hours after their symptoms have stopped to avoid infecting others.
But, worryingly, it seems some schools may be moving away from the official guidance.
mumsnet.com/talk/am_i_bein…
But, worryingly, it seems some schools may be moving away from the official guidance.
mumsnet.com/talk/am_i_bein…

The list of acute illnesses which have seen notable rises since the start of the pandemic goes on & on…
…but I’ll leave it there for now.
If you want to find out more, @1goodtern had done many excellent threads on this, such as the one below ⬇️
…but I’ll leave it there for now.
If you want to find out more, @1goodtern had done many excellent threads on this, such as the one below ⬇️
https://twitter.com/1goodtern/status/1979554542199898356
@1goodtern The data I’ve presented above hopefully demonstrates that there has indeed been a GENUINE increase in acute illness compared to pre-pandemic norms.
But why?
A growing number of scientists believe that Covid infections may be damaging immune systems…
bmj.com/content/390/bm…
But why?
A growing number of scientists believe that Covid infections may be damaging immune systems…
bmj.com/content/390/bm…

@1goodtern This is not a particularly new idea; it’s been discussed in scientific circles for years already.
Back in early 2023, the World Health Network (@TheWHN) published this article which summarised the latest research on Covid’s impact on the immune system.
whn.global/scientific/cov…
Back in early 2023, the World Health Network (@TheWHN) published this article which summarised the latest research on Covid’s impact on the immune system.
whn.global/scientific/cov…

The German Health Minister was also warning about the risks of developing immune deficiency or dysfunction from Covid infections back in early 2023…
n-tv.de/politik/Lauter…
n-tv.de/politik/Lauter…

A year later, in early 2024, the Yale School of Public Health published a series of infographics highlighting how Covid can create lasting detrimental impacts on the immune systems, making people more susceptible to other opportunistic infections.
https://twitter.com/_catinthehat/status/1782209760630096168

Another paper published in Science in 2024 explored the impact of immune damage in Long Covid, explaining how acute Covid infections can be associated with systemic immune cell activation & inflammation, widespread multi-organ dysfunction & thrombosis.
science.org/doi/10.1126/sc…
science.org/doi/10.1126/sc…

Please don’t stop reading here… there’s still more to the story.
Click “Show replies” to see rest of the thread.
⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️
Click “Show replies” to see rest of the thread.
⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️
The truth is, it’s becoming harder and harder to ignore this worrying rise in infectious diseases since the start of the Covid pandemic.
Even UKHSA is sounding the alarm 🚨
Lockdowns ended over 4 years ago now - we can’t keep blaming them forever.
pulsetoday.co.uk/news/clinical-…
Even UKHSA is sounding the alarm 🚨
Lockdowns ended over 4 years ago now - we can’t keep blaming them forever.
pulsetoday.co.uk/news/clinical-…

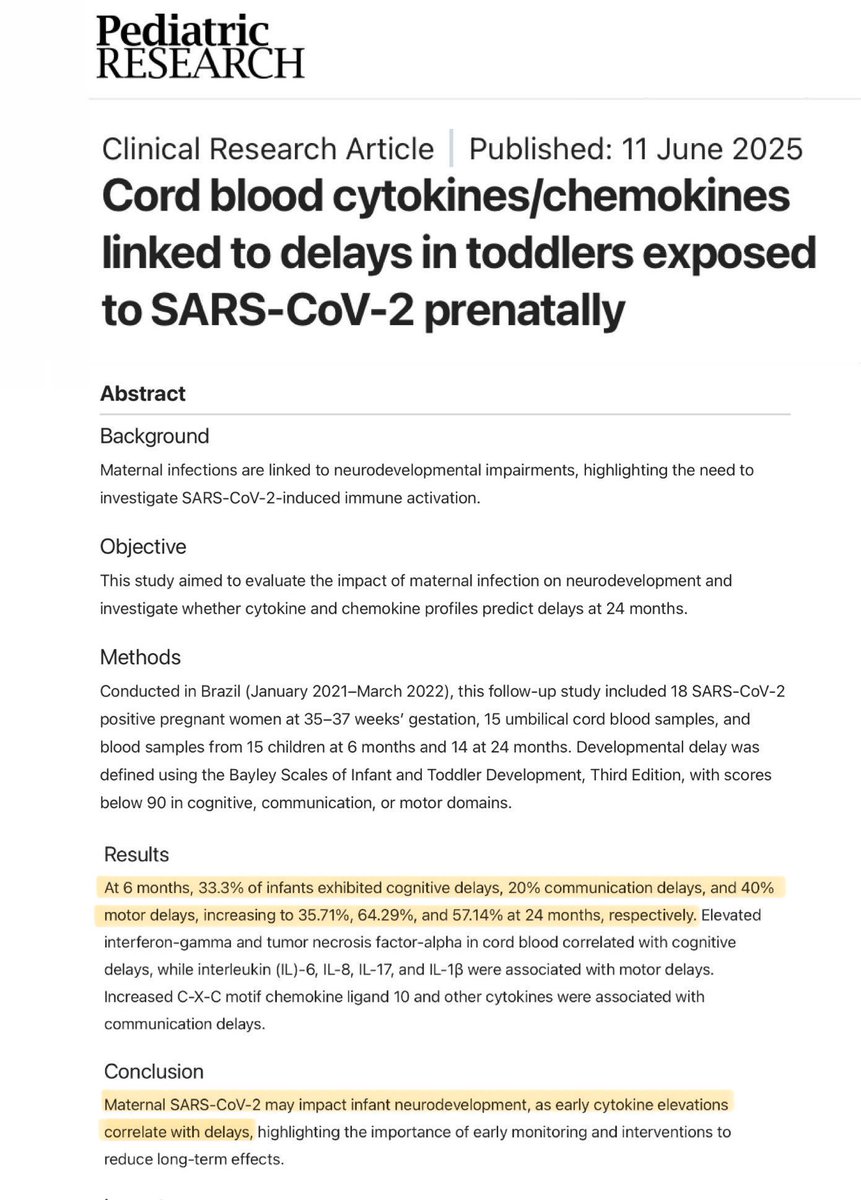
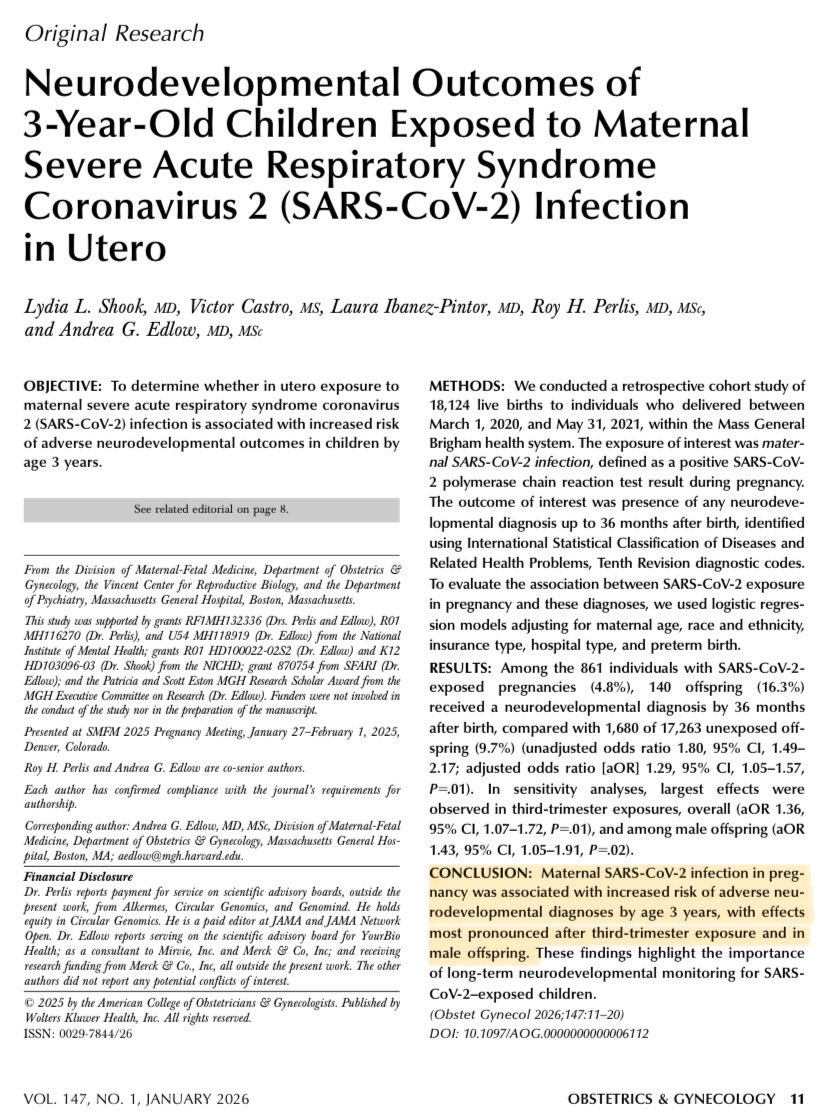
So far, I’ve only talked about acute illness in this thread (the initial phase of illness)… but when it comes to Covid, that’s really just the tip of the iceberg.
For children, the biggest risk is the long-term chronic illness which can result from repeated Covid infections.
For children, the biggest risk is the long-term chronic illness which can result from repeated Covid infections.

Many people have been led to believe that Covid is no more serious than a common cold.
But even mild initial infections can cause long-term complications affecting virtually every organ in the body, including the lungs, heart, kidneys & immune system.
publications.aap.org/pediatrics/art…
But even mild initial infections can cause long-term complications affecting virtually every organ in the body, including the lungs, heart, kidneys & immune system.
publications.aap.org/pediatrics/art…

ONS is no longer tracking prevalence of Long Covid…
…but, at the last count, the # of children with Long Covid had nearly DOUBLED in a year (between Mar 2023 & Mar 2024), rising to over 111K in England & Scotland.
That’s over 1K NEW cases in children PER WEEK across the year.
…but, at the last count, the # of children with Long Covid had nearly DOUBLED in a year (between Mar 2023 & Mar 2024), rising to over 111K in England & Scotland.
That’s over 1K NEW cases in children PER WEEK across the year.

And data from the UK Long COVID in Children & Young People (CloCk) study found that:
▪️A QUARTER of children (aged 11-17) were suffering from Long Covid 3 months after infection.
▪️Nearly a THIRD of these children had still not recovered after 2 years.
nature.com/articles/s4385…
▪️A QUARTER of children (aged 11-17) were suffering from Long Covid 3 months after infection.
▪️Nearly a THIRD of these children had still not recovered after 2 years.
nature.com/articles/s4385…

Meanwhile, in the US, a large study conducted as part of NIH’s RECOVER Initiative, shows that children are TWICE as likely to develop Long Covid after their 2nd Covid infection compared to their 1st infection.
“Reinfection really increases the risk.”
thelancet.com/journals/lanin…
“Reinfection really increases the risk.”
thelancet.com/journals/lanin…

Another study, also from the RECOVER Initiative, found that 10-20% of children who tested positive for Covid went on to develop Long Covid.
In fact, Long Covid may now have surpassed asthma as the most common chronic health condition for US children.
jamanetwork.com/journals/jamap…
In fact, Long Covid may now have surpassed asthma as the most common chronic health condition for US children.
jamanetwork.com/journals/jamap…

Prof Russell Viner is the Chief Scientific Adviser to the DfE.
At the Covid Inquiry, he was recently asked whether he has EVER provided advice to the DfE on Long Covid in children.
His answer is really quite extraordinary.
I’ve dubbed it ‘The Long Prevarication’.
At the Covid Inquiry, he was recently asked whether he has EVER provided advice to the DfE on Long Covid in children.
His answer is really quite extraordinary.
I’ve dubbed it ‘The Long Prevarication’.
During the Covid Inquiry, we also heard how the representative from Public Health England, Dr Shamez Ladhani, said at a Stakeholder Meeting in June 2021 (attended by the DfE, local govt officials & Education Union reps) that “children should not be labelled as having Long Covid”.
The fact that Long Covid in children has been brushed under the carpet is a BIG problem when it comes to understanding the key drivers of the school attendance crisis.
Long-term chronic illness is an undeniably an important driver which is barely even being considered…
Long-term chronic illness is an undeniably an important driver which is barely even being considered…
The Long COVID Kids charity conducted a survey of young people with Long COVID (aged 5-19):
▪️75% reported their attendance had been “greatly impacted”.
▪️Each child with Long Covid lost an average of 20.6 learning hours PER WEEK due to their condition.
longcovidkids.org/post/how-does-…
▪️75% reported their attendance had been “greatly impacted”.
▪️Each child with Long Covid lost an average of 20.6 learning hours PER WEEK due to their condition.
longcovidkids.org/post/how-does-…

Adult studies also illustrate the devastating impact Long Covid is having on those affected.
The UK LOCOMOTION study found that:
▪️28% of Long Covid sufferers have had to stop working altogether.
▪️A further 24% had reduced their paid working hours.
evidence.nihr.ac.uk/alert/how-much…
The UK LOCOMOTION study found that:
▪️28% of Long Covid sufferers have had to stop working altogether.
▪️A further 24% had reduced their paid working hours.
evidence.nihr.ac.uk/alert/how-much…

Unless you’ve experienced it yourself, it’s hard to comprehend the devastating impact Long Covid can have on young people.
Please spare a few minutes to watch this ITV News report which illustrates what it’s like for Long Covid kids & their families.
Please spare a few minutes to watch this ITV News report which illustrates what it’s like for Long Covid kids & their families.
Whenever declining pupil attendance is discussed, mental health is often cited as a key driver.
And this is indeed an important factor.
But what is often *not* mentioned is that these mental health issues are often hugely exacerbated by chronic illness.
lboro.ac.uk/news-events/ne…
And this is indeed an important factor.
But what is often *not* mentioned is that these mental health issues are often hugely exacerbated by chronic illness.
lboro.ac.uk/news-events/ne…

Many children living with Long Covid were previously healthy & high-achieving…
…but suddenly found themselves increasingly isolated from peers, often unable to attend school full-time & no longer able to participate in sports, hobbies or a social life.
longcovidkids.org/post/how-does-…
…but suddenly found themselves increasingly isolated from peers, often unable to attend school full-time & no longer able to participate in sports, hobbies or a social life.
longcovidkids.org/post/how-does-…

A recent US study (2025) concluded that “Long Covid Is Fueling a Mental Health Crisis in Children”.
The study found that:
▪️Nearly 40% of children with Long COVID are experiencing significant symptoms of anxiety or depression, many for the first time.
neurosciencenews.com/long-COVID-chi…
The study found that:
▪️Nearly 40% of children with Long COVID are experiencing significant symptoms of anxiety or depression, many for the first time.
neurosciencenews.com/long-COVID-chi…

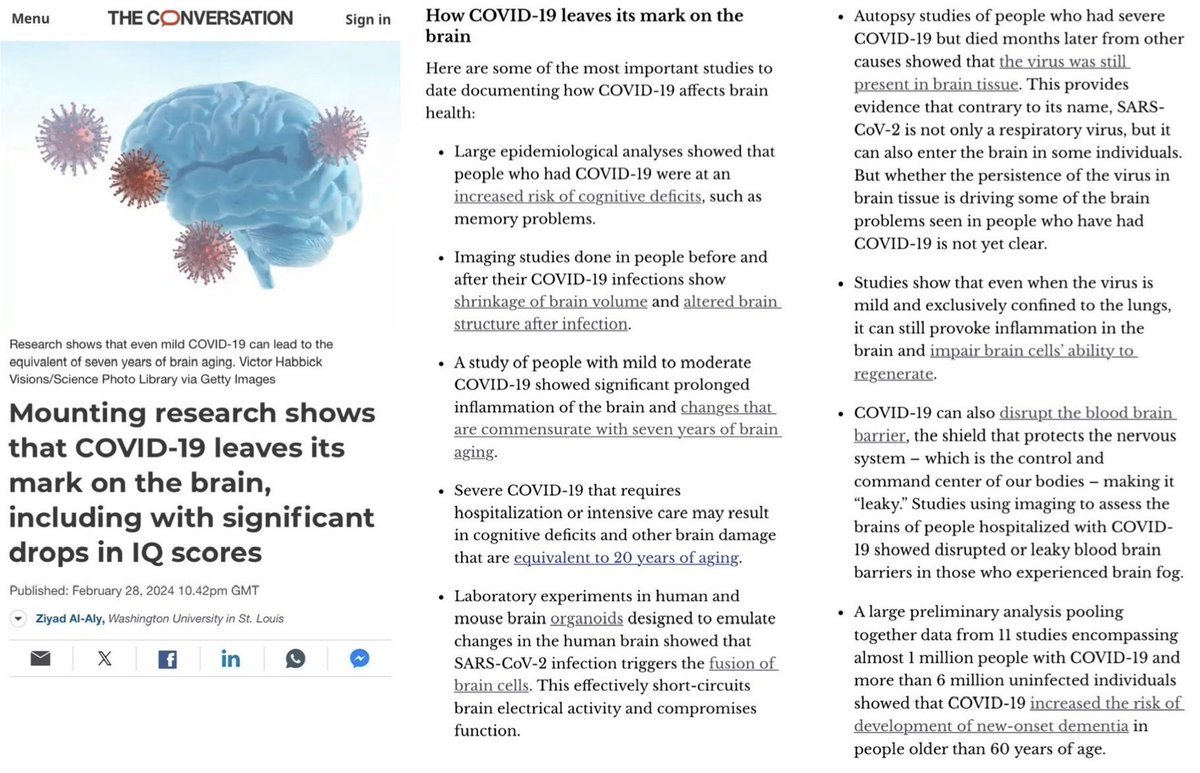
But there’s another crucial aspect which is also commonly overlooked…
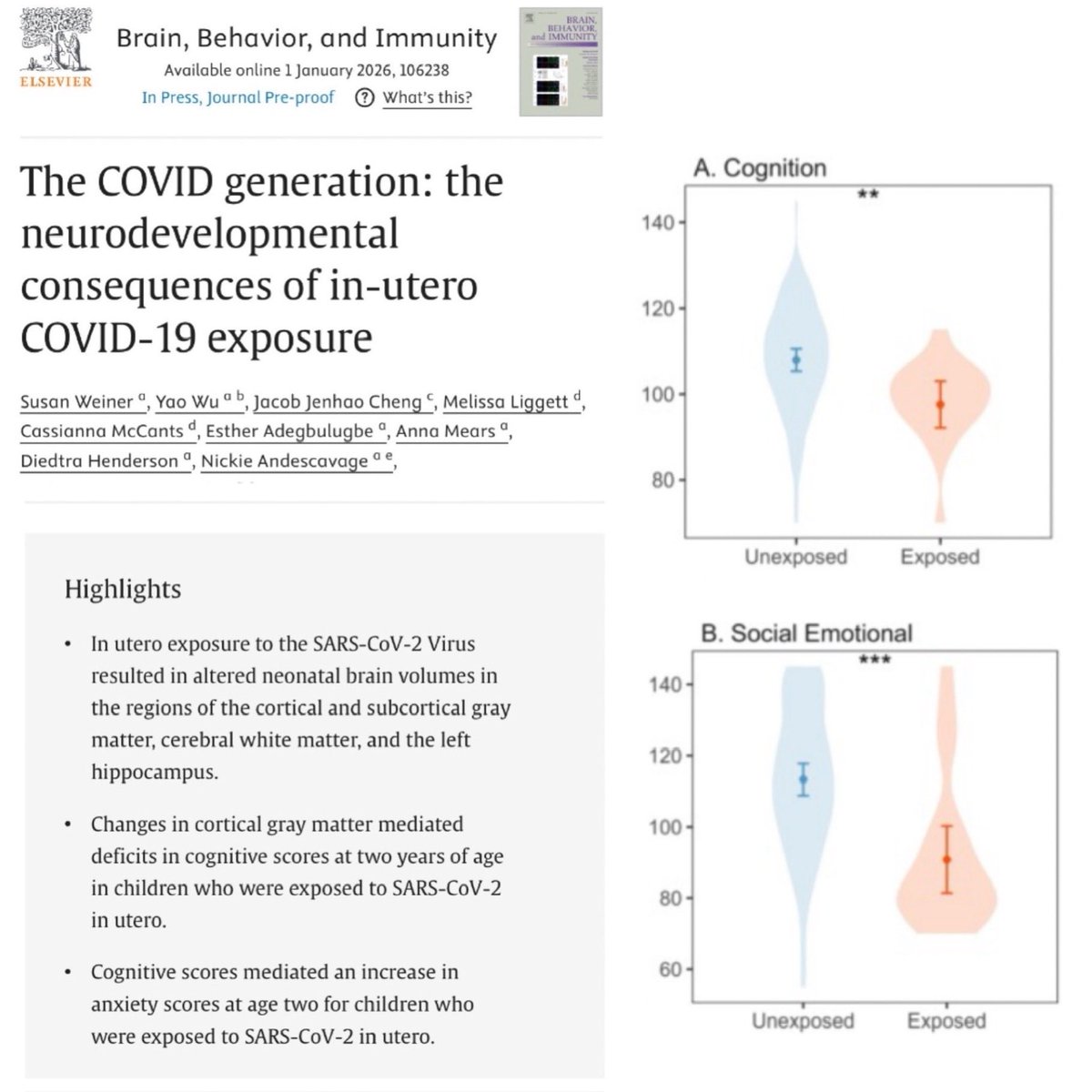
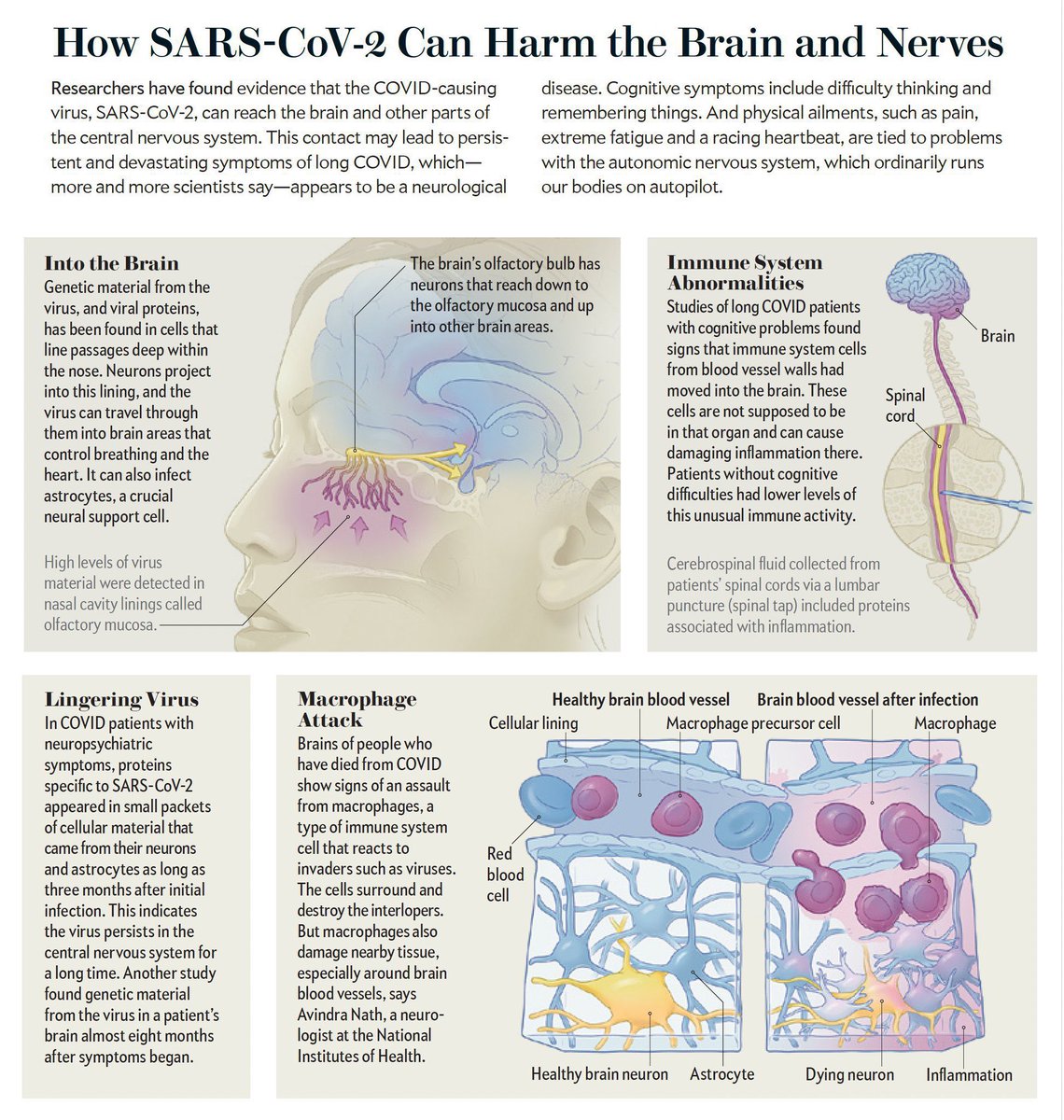
A growing body of evidence shows that Covid infections can have direct physiological effects on the brain which may trigger or exacerbate mental health symptoms.
A growing body of evidence shows that Covid infections can have direct physiological effects on the brain which may trigger or exacerbate mental health symptoms.
This excellent article from Dr Al-Aly (@zalaly) provides a comprehensive summary of the mounting evidence about how Covid leaves its mark on the brain, including with significant drops in IQ scores.
theconversation.com/mounting-resea…
theconversation.com/mounting-resea…
In this SciAm article (Feb 2023), @SutherlandPhD discusses the various long-term neurological aspects of Covid.
She spent a year compiling evidence from an ever-increasing mountain of sources to write this detailed feature.
It’s well worth a read.
scientificamerican.com/article/long-c…
She spent a year compiling evidence from an ever-increasing mountain of sources to write this detailed feature.
It’s well worth a read.
scientificamerican.com/article/long-c…
A systematic review (published Feb 2024) found that:
▪️44% of children experiencing neurological symptoms after Covid infection had abnormal neuroimaging findings, eg. ADEM-like lesions, encephalitic pattern, myelitis & other anomalies.
nature.com/articles/s4159…
▪️44% of children experiencing neurological symptoms after Covid infection had abnormal neuroimaging findings, eg. ADEM-like lesions, encephalitic pattern, myelitis & other anomalies.
nature.com/articles/s4159…

A state-of-the-art narrative review published by the American Academy of Paediatrics in Feb 2024 reported that:
▪️Covid infections have been linked to a significant rise in mental health conditions in children, including anxiety, depression & ADHD.
publications.aap.org/pediatrics/art…
▪️Covid infections have been linked to a significant rise in mental health conditions in children, including anxiety, depression & ADHD.
publications.aap.org/pediatrics/art…

An important study, conducted at Oxford Uni studied 785 ppl who received brain scans before & during the pandemic as part of the Biobank study.
Those who tested positive for Covid between the 2 scans exhibited significant structural changes in the brain.
nature.com/articles/s4158…
Those who tested positive for Covid between the 2 scans exhibited significant structural changes in the brain.
nature.com/articles/s4158…

A similar Italian study (Oct 2024) used cognitive assessments & MRI data to investigate the impact of Covid infection on young people’s brains.
Results revealed persistent functional & structural changes in certain brain areas after Covid infection.
nature.com/articles/s4139…
Results revealed persistent functional & structural changes in certain brain areas after Covid infection.
nature.com/articles/s4139…

Another study (Oct 2022) used high-res microscopy to investigate Covid’s effect on the brain in rhesus monkeys.
7 days post-infection, SARS-CoV-2 was detected in the olfactory cortex & connected areas, accompanied by neuroinflammation & neuronal damage.
sciencedirect.com/science/articl…
7 days post-infection, SARS-CoV-2 was detected in the olfactory cortex & connected areas, accompanied by neuroinflammation & neuronal damage.
sciencedirect.com/science/articl…

In this New Zealand study (Mar 2025), scientists studied the impact of COVID infections on the cognitive performance of university undergraduate students.
37% of undergrads exhibited impaired cognition for up to 17 months following COVID infection.
sciencedirect.com/science/articl…
37% of undergrads exhibited impaired cognition for up to 17 months following COVID infection.
sciencedirect.com/science/articl…

There are many more studies demonstrating the impact of repeated Covid infections on the brain, and how this can trigger and exacerbate mental health issues as well as cognitive issues.
If you want to read more, you can find further studies in this lengthy thread… ⬇️
If you want to read more, you can find further studies in this lengthy thread… ⬇️
https://twitter.com/_catinthehat/status/1763878368242524370
So, the next time you hear someone questioning if there’s genuinely more illness in school-age children now compared to pre-pandemic, hopefully this thread has provided some much needed clarity…
..all backed up by tangible data and evidence.
..all backed up by tangible data and evidence.
And when you think about the increased rates of illness in children, remember, it’s not driven by just one thing.
There are 4 key factors to consider:
1) the introduction of a brand new, highly infectious virus (Covid) on top of all the other pre-existing childhood illnesses;
There are 4 key factors to consider:
1) the introduction of a brand new, highly infectious virus (Covid) on top of all the other pre-existing childhood illnesses;
2) the long-term health impacts of Covid, which include chronic illness and the worsening of existing conditions;
3) worsening mental health linked to both the social impact & physiological effects of Long Covid;
3) worsening mental health linked to both the social impact & physiological effects of Long Covid;
Ooof, this is a really bad point for a thread break.
We’ve only got through 3 out of the 4 summary points and there’s still more to the story.
Please click “Show replies” once more to see the final part of the thread.
⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️
We’ve only got through 3 out of the 4 summary points and there’s still more to the story.
Please click “Show replies” once more to see the final part of the thread.
⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️
And the 4th factor to consider which is driving increased illness in children is:
4) immune system dysfunction triggered by Covid infections, which can make children more susceptible to other infections and also reactivate viruses which may have been lying dormant in the body.
4) immune system dysfunction triggered by Covid infections, which can make children more susceptible to other infections and also reactivate viruses which may have been lying dormant in the body.
When you look at all of the evidence in this thread, hopefully it will be clear why pupil illness absences are 40% higher than pre-pandemic.
And also why it will be very hard to move the dial on improving pupil attendance without addressing the spread of illness in classrooms.
And also why it will be very hard to move the dial on improving pupil attendance without addressing the spread of illness in classrooms.

And I should mention that it’s not only the children who are experiencing significantly higher rates of illness.
Unsurprisingly, as highly-infectious airborne illnesses spread like wildfire through schools, teachers are affected too.
This has resulted in soaring supply costs.
Unsurprisingly, as highly-infectious airborne illnesses spread like wildfire through schools, teachers are affected too.
This has resulted in soaring supply costs.

So, what can be done about this?
How do we fix the problem?
Thankfully, there are some simple solutions…
… but I must get some sleep now. I’ll add more to the thread in the morning.
How do we fix the problem?
Thankfully, there are some simple solutions…
… but I must get some sleep now. I’ll add more to the thread in the morning.
• • •
Missing some Tweet in this thread? You can try to
force a refresh