Everyone here seems to be arguing various ideological positions on using private facilities to ease AB's health woes.
Lets look at some data and try to have an evidence based view of some of this. In fact lets look at AB data. /1
Lets look at some data and try to have an evidence based view of some of this. In fact lets look at AB data. /1
Around 2018 AB noted that wait times for what it called priority surgical procedures were longer than the Cdn average. Not a good look for a province that felt it had a good system.
So why were these times increasing? Lots of reasons but a major one is shown in the graph. /2
So why were these times increasing? Lots of reasons but a major one is shown in the graph. /2
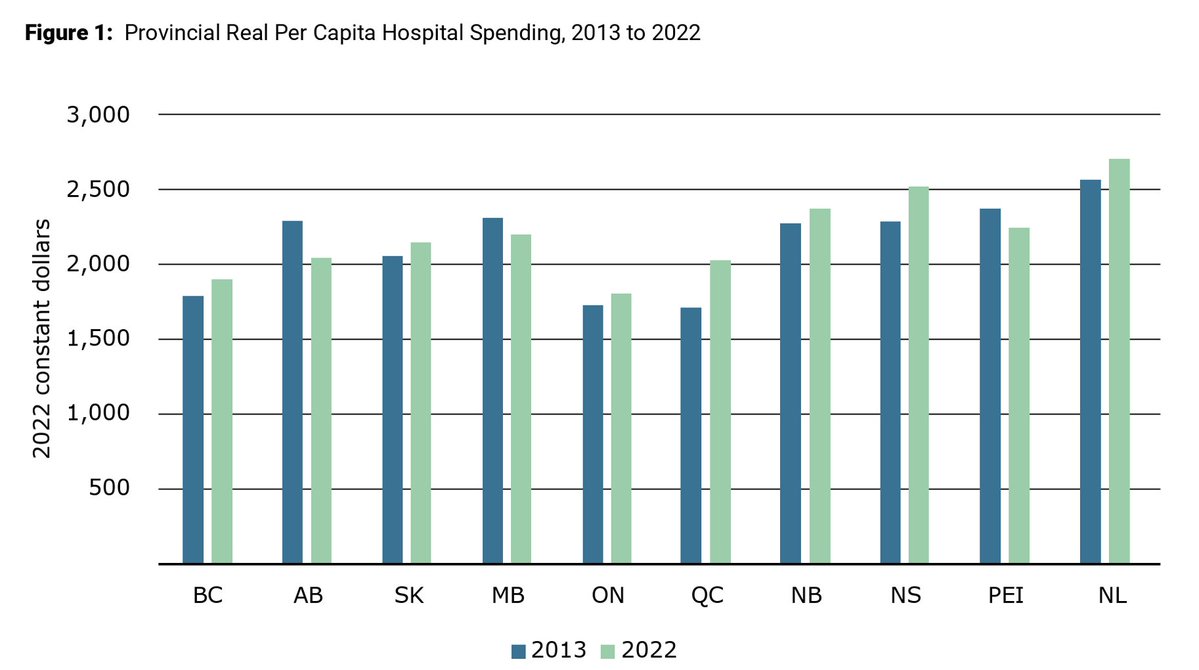
Although this goes to 2022 there has been a reduction in real $/capita paid by the AB government to the hospital system since about 2010. This translates into fewer beds and OR capacity.
In terms of OR time this was a large reduction. /3
In terms of OR time this was a large reduction. /3
Ernst and Young reviewed this in 2019 and observed that AB was only utilizing 70% of its OR capacity. We had room for an easy 18K more procedures in existing space.
That would require an investment in people to manage this space of course. /4
That would require an investment in people to manage this space of course. /4
Lets look at the beds side of this equation. Not only do you need OR's you need beds for the patients. Staffed beds. From CIHI here are the data for AB.
We certainly weren't increasing them were we? /5
We certainly weren't increasing them were we? /5

So in 2019 the AB gov announced a major push to perform priority surgeries. Known as the Alberta Surgical Initiative (ASI) it utilized Chartered Surgical Facilities (CSF's or private hospitals). /6
Despite AB already having OR's these built new ones and used surgeons and other workers from the public system to do the work.
The # of cases in the CSF's ramped up from 2019 to now. The GoA is now saying we need to double down and add more CSF capacity. /7
The # of cases in the CSF's ramped up from 2019 to now. The GoA is now saying we need to double down and add more CSF capacity. /7
We already have data on the effectiveness of this approach over the last several years. Lets look at it.
In blue and red you can see the hip and knee wt time data (shown as an inverse).
Around 2019 we clearly had to do something. But the CSF's did not fix this. /8
In blue and red you can see the hip and knee wt time data (shown as an inverse).
Around 2019 we clearly had to do something. But the CSF's did not fix this. /8
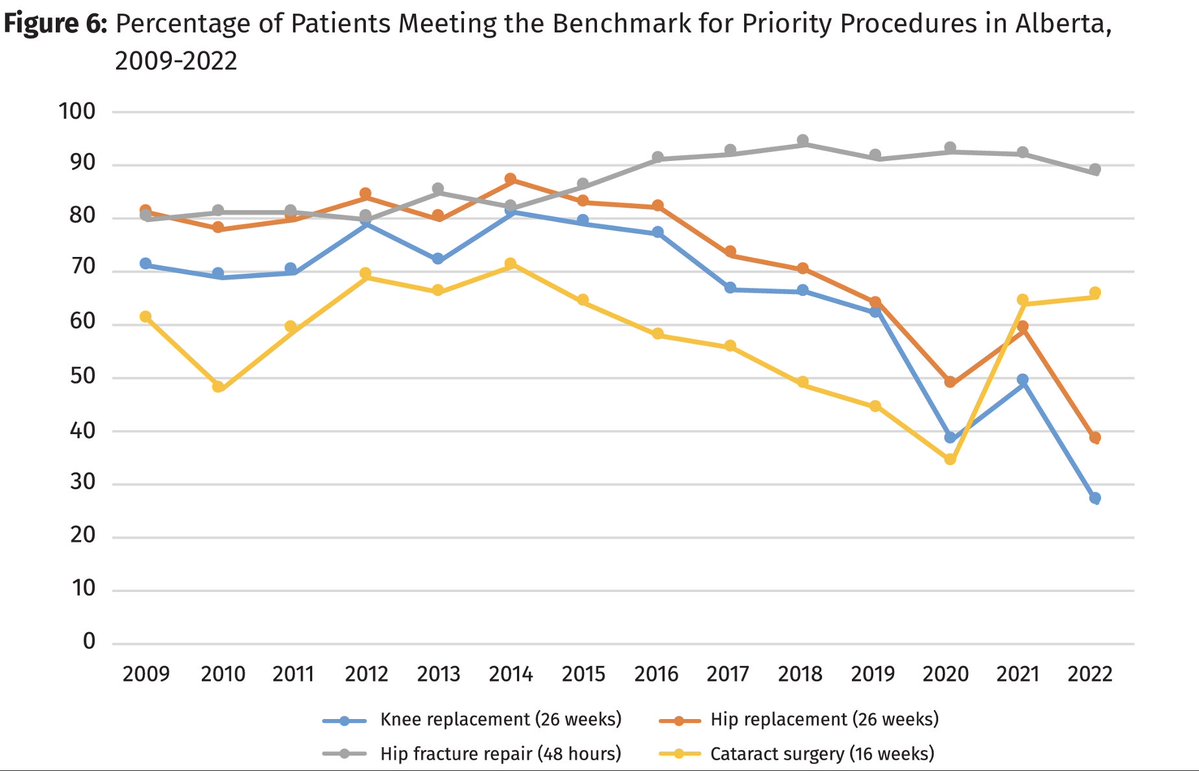
In fact the problem got worse. Not what we would want to see. While the ASI increased easy cases in the CSF's the total number of cases in the province actually fell.
And they appeared to be more expensive than in AHS. That is the accusation in #CorruptCare /9
And they appeared to be more expensive than in AHS. That is the accusation in #CorruptCare /9
Around this time we also started seeing anecdotal reports of ER closures and surgical diversions from one hospital to another. Because the hospital did not have surgeons/anesthetists/etc on call to do the work.
We also started hearing about cancer surgeries being delayed. /10
We also started hearing about cancer surgeries being delayed. /10
Was this linked to siphoning off specialists to the easy CSF procedures? Well there is data on that as well.
From 2019-2023 only cataract wt times really improved. More worrisome is the massive increase in waits for very time sensitive cases. /11
From 2019-2023 only cataract wt times really improved. More worrisome is the massive increase in waits for very time sensitive cases. /11
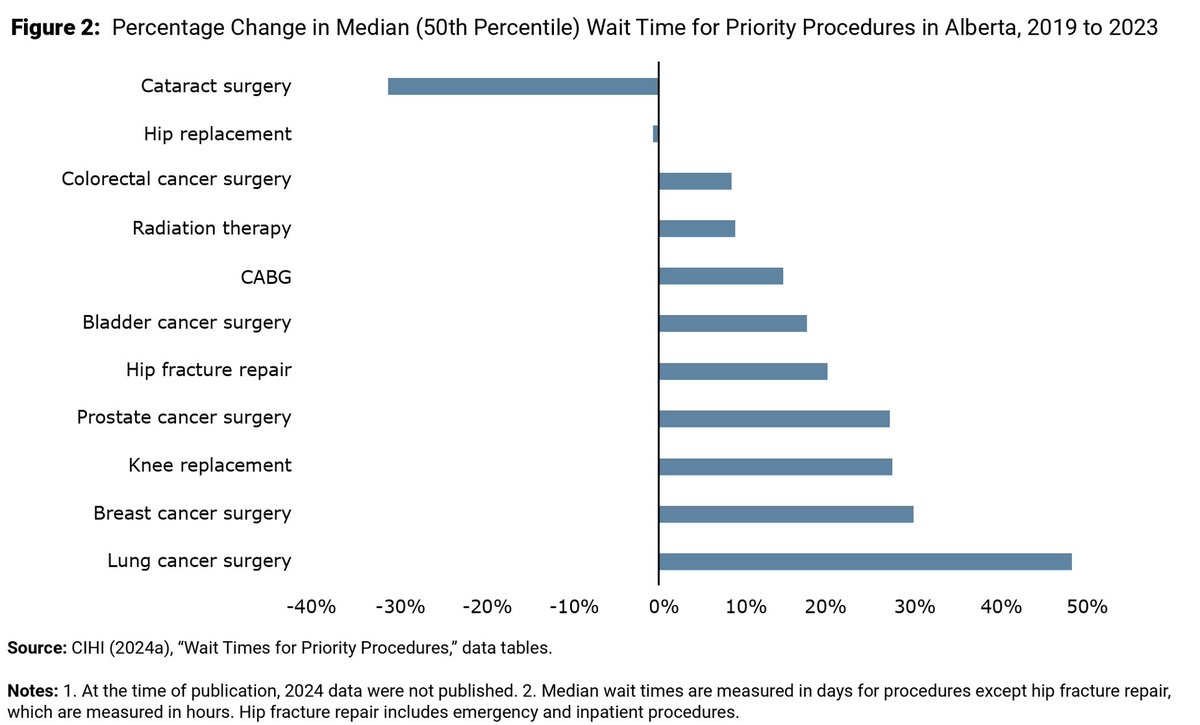
Cancer therapy seems to be suffering from this process and all we have to show for it are a few more cataracts it seems.
Folks, we've done the experiment on private surgical access and it has made things worse. Measurably.
Other than ideology why continue? /12
Folks, we've done the experiment on private surgical access and it has made things worse. Measurably.
Other than ideology why continue? /12
So what else can we do instead? This is whistling in the wind but here is a list:
1. Use the OR's we've already built and get some cheaper cases done. CSF's have only done 16K cases - opening our existing OR's have space for 18K.
/13
1. Use the OR's we've already built and get some cheaper cases done. CSF's have only done 16K cases - opening our existing OR's have space for 18K.
/13
2. Demand docs use centralized triage systems (shown to be better).
3. Use the CSF money to create LTC beds rather than new OR's we don't yet need. This would allow moving ALC pts to a better place and increase our hospital beds. Open ER's and OR's. /14
3. Use the CSF money to create LTC beds rather than new OR's we don't yet need. This would allow moving ALC pts to a better place and increase our hospital beds. Open ER's and OR's. /14
Folks, Einstein once said that repeating the same thing over and over, hoping for a different result is insanity.
Our government has tried the private experiment. It has failed. Why repeat it again and again? /end
Our government has tried the private experiment. It has failed. Why repeat it again and again? /end
• • •
Missing some Tweet in this thread? You can try to
force a refresh