Past Dean, Cumming School of Medicine; Gastroenterologist, Avid photographer in no particular order. Opinions are mine.
Jun 19 • 13 tweets • 3 min read
Yesterday was a sad day for evidence based medicine in AB. GoA is going ahead with Bill 11.
Despite the fact we‘ve already tried this and it has failed in its stated goals. Lets just put this out there clearly./1
Yesterday our gov said that allowing MD’s to provide both pub and priv access will remove people from the pub wt list and therefore it will shorten.
Sounds wonderful.
The problem is that we’ve done this before and that is not what happens. Ever. /2
Jun 4 • 6 tweets • 1 min read
OK. I went back and looked.
AB was the first province in Canada to introduce pt-pay access for radiology (CT/MRI). It was done in 1993 and the rationale at the time was that wt lists were too long.
/1
By allowing some pts to pay and "leave the queue", pay for access would improve access for everyone.
So we've had 30 years of this expt in AB. Has it worked?
Proponents have argued that this is the answer to our access problem. /2
Apr 17 • 13 tweets • 3 min read
Excellent, but chilling, article here. A short thread.
1. “This could end Canadian medicare as we know it.”
Is it hyperbole? No, I don't think so. /1
‘Pandora’s box’: Danielle Smith and insurance giants unleash attack on healthcare breachmedia.ca/pandoras-box-d…
What Bill 11 allows are 2 major things. a) MD's can both bill the provinces universal insurance plan and b) bill the patient directly for "medically insured services".
b) Intense discussions are ongoing with insurance companies to implement private insurance. /2
Nov 28, 2025 • 7 tweets • 2 min read
Let me try to explain the difference one more time. I will use some made up numbers that although made up *do* describe the situation.
Imagine we have 6 orthopdedic surgeons, 2 general surgeons, 2 heart surgeons and 2 cancer surgeons. We also have 6 anesthetists. /1
In this simplified model this means that we can do 6 operations per day. We are limited by the number of anesthetists.
The way we manage this right now is that the system gives everyone a little time and we leave some aside for emergencies that are triaged based on need. /2
Nov 25, 2025 • 12 tweets • 3 min read
I want to present another take on the issue of private healthcare.
In the end I'm going to suggest that gov is bringing the free market to bear on the wrong problem, but stay with me as I try to get us there.
The first question is what is the problem we are trying to fix? /1
My understanding is that it is the issue of people who have to wait exorbitant times for low acuity surgery (hips/knees, cataracts, etc).
We all agree many wait too long.
So government is proposing to allow people who are waiting to purchase an "upgrade". /2
Nov 20, 2025 • 15 tweets • 4 min read
Everyone here seems to be arguing various ideological positions on using private facilities to ease AB's health woes.
Lets look at some data and try to have an evidence based view of some of this. In fact lets look at AB data. /1
Around 2018 AB noted that wait times for what it called priority surgical procedures were longer than the Cdn average. Not a good look for a province that felt it had a good system.
So why were these times increasing? Lots of reasons but a major one is shown in the graph. /2
Nov 18, 2025 • 10 tweets • 2 min read
Let me just put out there another major problem with this.
The creation of a public and private stream of medicine and the ability of physicians to work in both - at their discretion - is an incredible boon to physicians.
So lets imagine a physician who believes that what they do, should be compensated better. I know a lot for whom this is actually true.
Now we have a solution. You can charge the patient directly and if they are able/willing to pay you get what you think you deserve. /2
Nov 16, 2025 • 8 tweets • 3 min read
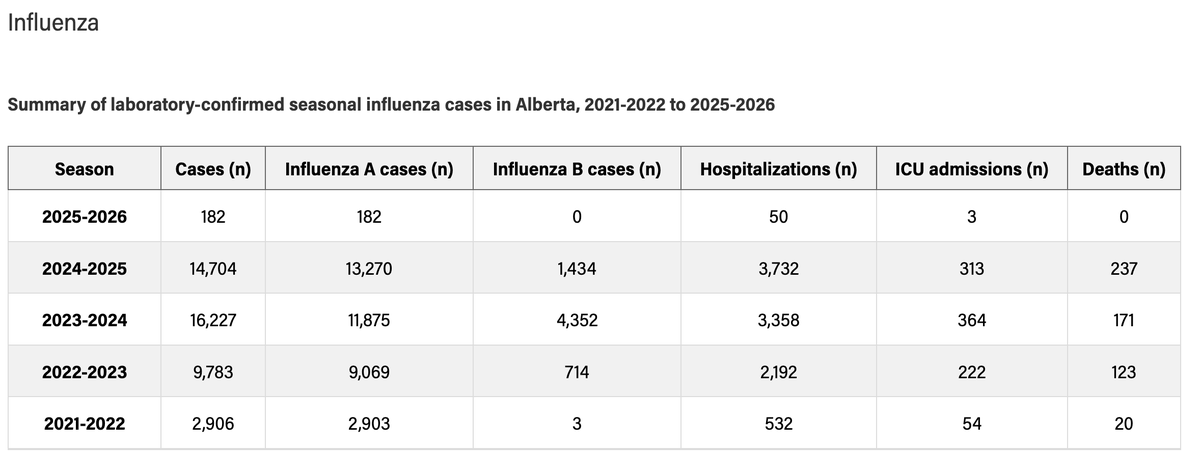
OK. Lets look at how the GoA's strategy to suppress/oops, administer C-19 vaccination is going this year. Data from the Respiratory dashboard.
We are about 8 weeks into the "campaign" at this point. /1
Remember, GoA has restricted where you can get the shot, asked most to pay for it, under ordered supply and put up other barriers.
We would predict poor uptake this year. So lets see. /2
Nov 5, 2025 • 7 tweets • 2 min read
I've had a great conversation with someone who knows how vaccines are ordered and distributed.
Let's see where the blame lies for the vaccine shortfall in AB this year.
A bit of necessary background. Vaccines are not like regular drugs. For something like penicillin - /1
It is the same 'formula'. Vaccines, however, are tailored to this years virus. They have no shelf life and are useless if not used in the year they are designed for.
So companies do not 'over produce' them. For things like flu an order for the fall must be in by Feb. /2
Nov 1, 2025 • 12 tweets • 3 min read
This is simply so wrong..... Although several of us have explained it before let me try again. A short thread. /1
Opinion: Private-pay option will improve access to MRIs and CT scans via @edmontonjournaledmontonjournal.com/opinion/column…
The main premise of this is that the healthcare system is like a market place. If you allow the free market in it will solve the issues we have.
Specifically, if you allow some of us to pay for our MRI then this will increase overall capacity and all will benefit. /2
Oct 26, 2025 • 15 tweets • 3 min read
I want to paint a picture of how AB's "Pay for your own Screening" is likely going to go. A thread.
I'm going to use a fictional example from my own specialty that I've now just retired from. I'm positive that these discussions have already started. /1
Who am I to guess at this? Years ago I was one of the creators of the Calgary Colon Cancer Screening Center - something I'm very proud of.
It does amazing work but there was a difficult balance in keeping it part of the public system. Today I don't think it would be. /2
Oct 24, 2025 • 11 tweets • 3 min read
Just got my flu shot. Some interesting (to me at least) thoughts about this - and so a short thread.
I'm in rural AB right now and so on a trip into town for groceries stopped at an independent pharmacist. Always fun to chat to these people. /1
I asked about getting vaccinated. Was told that sure he could give me my flu shot and if I wanted, C-19. Of course the latter he would have to be a special order and would be $150.
I asked why he didn't have any of the C-19 on hand. /2
Oct 22, 2025 • 7 tweets • 2 min read
There is a huge problem with this that many of us recognize. A short thread.
We call it the incidentaloma issue.
Let me use an example that has actually happened. Imagine you believe young adults should be screened for abdominal cancer to 'protect' their loved ones. /1
Much like the stomach cancer mentioned in this ad.
So you advertise cheap CT scans for young healthy adults to 'prevent the scourge of cancer'. Pay a small amount for piece of mind. What could go wrong?
And people come forward. They get low dose CT abdominal CT's. /2
Oct 22, 2025 • 10 tweets • 2 min read
Let me see if I can explain this a bit. A short thread.
First, we've recognized a paradox for decades.
Cancer cells are different from us - 'self'. Our immune system is there to reject 'non-self'. So why does it not get rid of cancer cells? /1
In fact, we probably generate small cancers all the time that our immune system does dispose of.
But every once in a while along comes a sneaky cancer that can hide from the immune system. This is a dangerous one.
Sometimes we can see this in action. /2
Oct 17, 2025 • 16 tweets • 4 min read
OK - a short set of thoughts on the crisis of Canadian healthcare. It expresses itself in many ways across every province these days.
How do we know it is in crisis? /1
Witness waiting times, #'s who can't find a family MD, ER closures and most recently the resignation of an entire department of O&G in Kamloops.
We are in a mess and need to understand what the problem is. If we don't we risk spending time and $ on the wrong things. /2
Aug 21, 2025 • 14 tweets • 4 min read
OK - a thread. There are a lot of suggestions as to how we improve our h/c system.
But there are naysayers - some who will say everything the UCP/CPC do is just fine but also some with thoughtful objections.
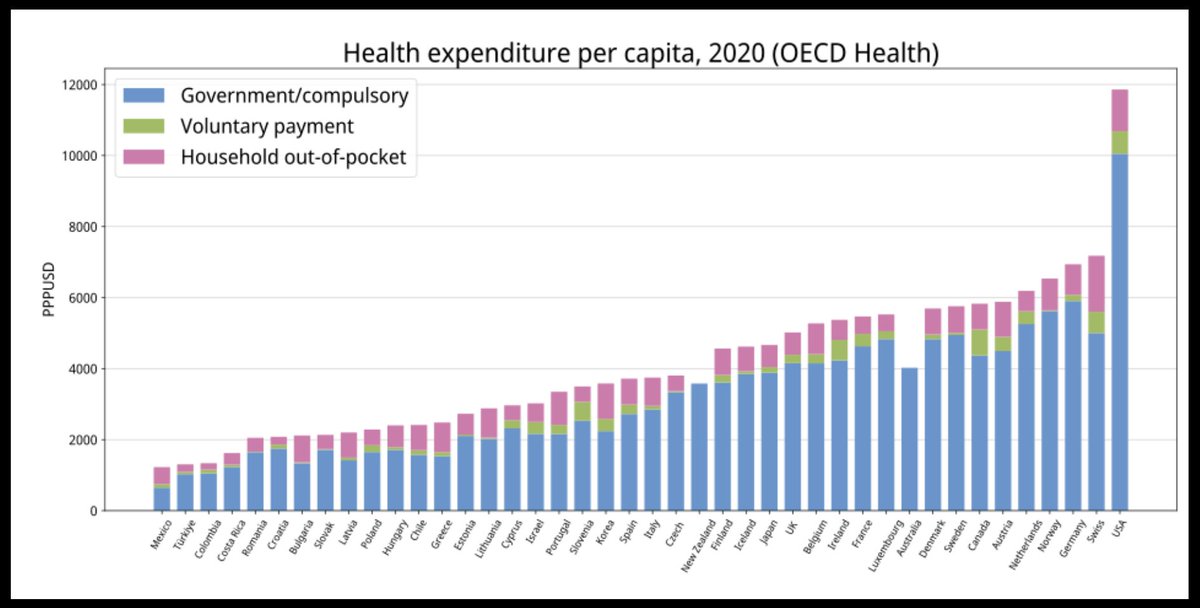
The commonest of these is the "we have no more $" one. /1
So I thought I'd take a dive into comparative h/c spending and the results different countries get from spending.
First, lets look at all the OECD countries and what they spend per capita.
You can see that Canada sits at the high end. /2
Aug 16, 2025 • 5 tweets • 2 min read
I'd like to take a stab at this as I think it is a major piece we are missing. Will take me longer than one reply and so I've reposted this as a thread. These are my thoughts.
The highest level of accountability is between citizen and government. /1
We pay taxes. We expect a well functioning and well managed h/c system. Right now we have neither and government shrug's their shoulders. *That* should not happen.
Second level is accountability between providers and the system. /2
Jun 17, 2025 • 5 tweets • 1 min read
Well, surprise, surprise. A brand new, flashy health care reorganization to fix all our problems.
We now have a *Hospital Based Leadership Structure*.
Amazing. I'm sure it will be wonderful. And instead of a few zones we now have 7 corridors. What a difference! /1
On top we have Alberta Health. Supposed to set provincial priorites. Next in line we have Acute Care AB which will translate the AH strategy into tactics for the hospitals.
Lots of hospitals so how to do that? /2
May 22, 2025 • 4 tweets • 1 min read
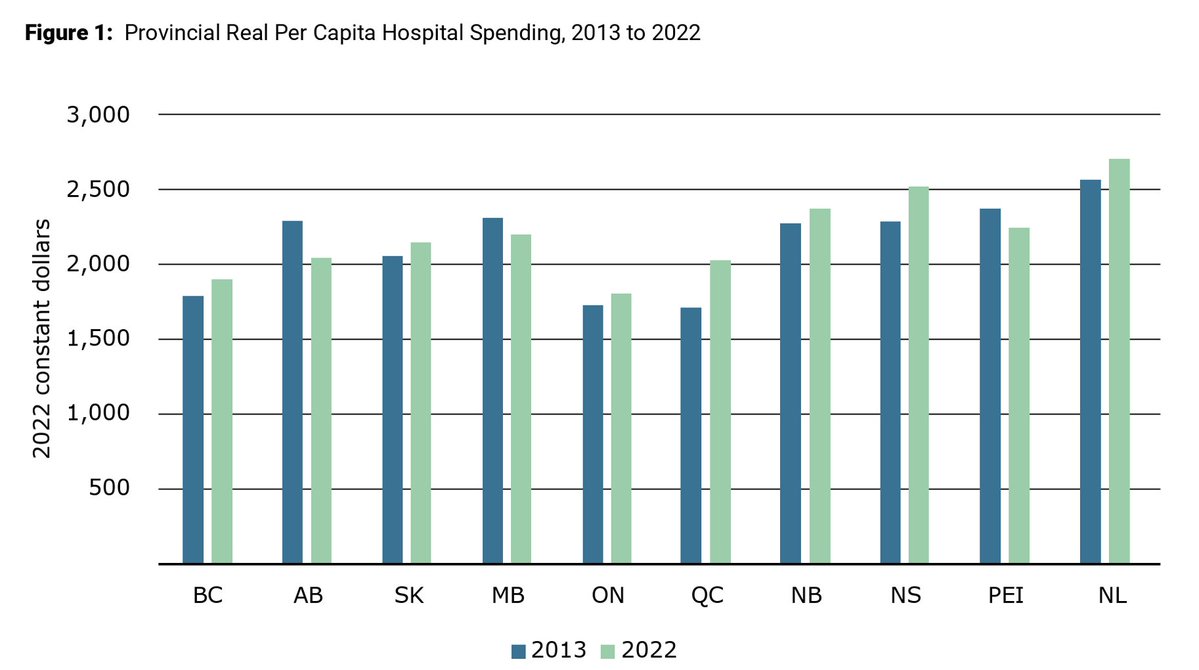
This is a great report (as usual) from Andrew Longhurst. I'm just going to point to a few key findings in a short thread.
First, it is a direct rebuke to our Premiers comments /1
Attack on Alberta Health Services reveals failings of privatization healthcoalition.ca/attack-on-albe…
In Feb she claimed no matter how much $ she gave to AHS surgical rates were not increasing.
This *not* correct.
First, there has been no increase in funding. Only decreases.
One exception. In 22-23 a 14% increase in $ and a similar increase in surgery. /2
May 7, 2025 • 9 tweets • 2 min read
I'd like to comment on todays G&M editorial. It is a whopper and makes several points that I agree with.
Points that will predictably raise the blood pressure of the more heavily influenced members of our species.
A thread. /1
theglobeandmail.com/opinion/editor…
The first, and overriding, point is that the return of a once eradicated disease, measles, is a remarkable failure of government.
Make no mistake. This is a killer disease that we once had under control.
There is no reason that 3 children in AB should be in the ICU. /2
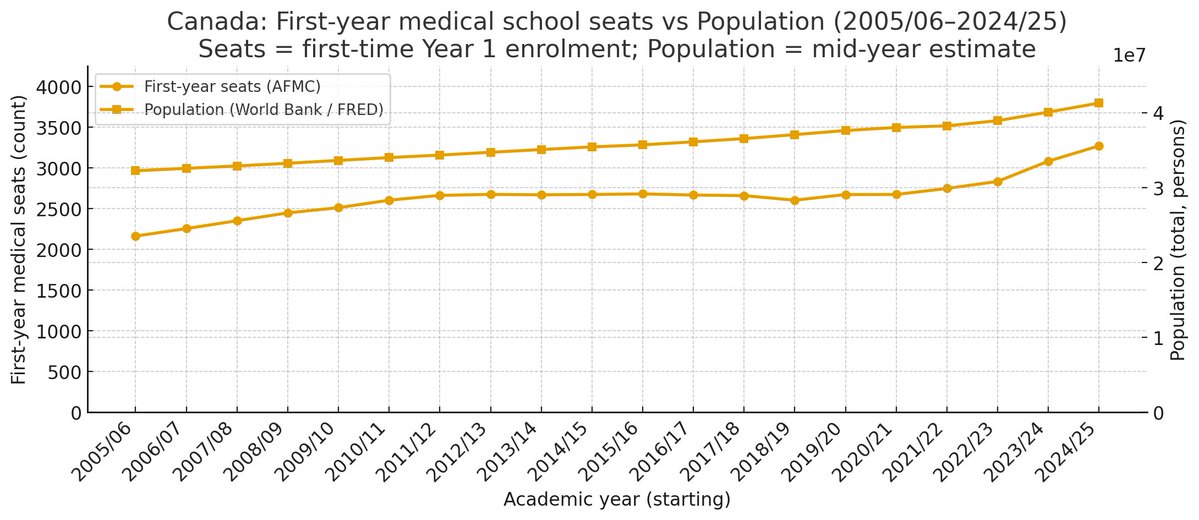
May 2, 2025 • 6 tweets • 2 min read
I wish government understood this. A short thread.
We are desperately short of MD's. Comparable countries have roughly twice as many as we do.