1/ Under a 1980 law known as Bayh-Dole, government scientists have a unique arrangement. They can collect royalties from pharmaceutical companies for discoveries they make while working for us.
fullmeasure.news/news/shows/con… x.com/humanspective/…
fullmeasure.news/news/shows/con… x.com/humanspective/…
2/They even have their own Coalition! bayhdolecoalition.org
3/ They even have a booklet explaining how all this works for biomedical research and drugs. 🥴 techpipeline.com
4/ Their royalty rates are extremely profitable. Here’s an example. researchgate.net/figure/Frequen…

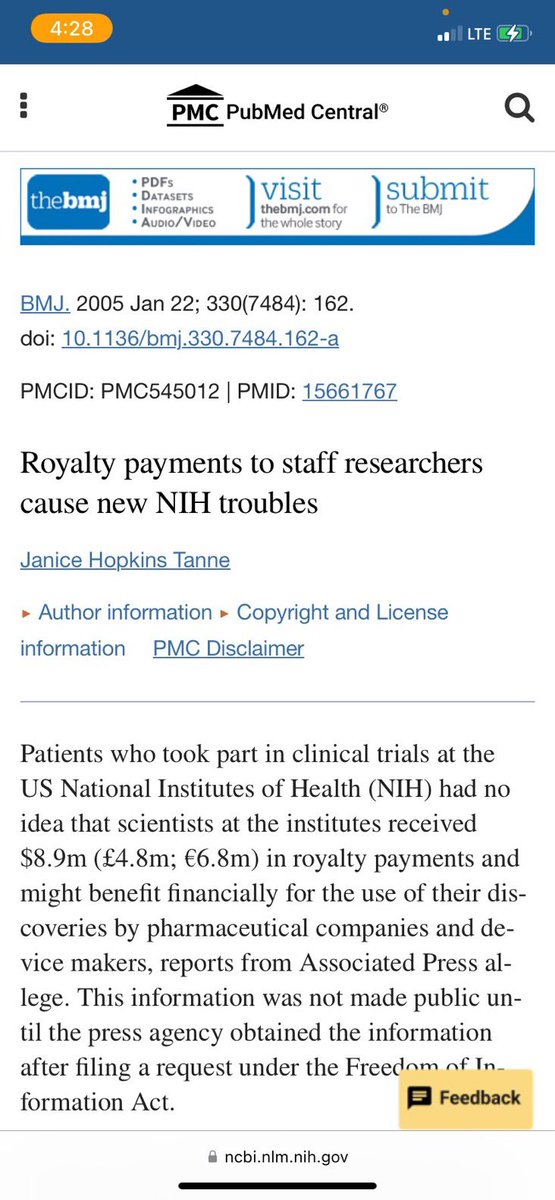
5/ Here is a Pubmed publication admitting the issue while trying to down play how serious the issue is. pmc.ncbi.nlm.nih.gov/articles/PMC54…
6/ Yes, they are very aware of the conflict of interest problem. However, they really do value their investors. Most of which are pharma companies. They make investing a cinch and let them know about royalties. cdc.gov/technology-and…

7/ Once you see this issue, you cannot unsee it. Pair the Bayh-Dole Act issue with the capture of medical Journals via the Pubpeer Mob funded by the Arnold Foundation. It then becomes clear why they shove drugs that solve nothing at patients after running their half-baked drug trials.
8/ To learn about the Arnold Foundation and how ties in to all of it, please search the hashtags @Jikkyleaks mentions here. 👇
https://twitter.com/jikkyleaks/status/2009860618871021870
• • •
Missing some Tweet in this thread? You can try to
force a refresh





