1. Today's lesson from my forum is on hyperhydrosis and dysautonimia.
QUESTION: Hi everyone,
Starting this thread to document my improvements or lack thereof, as I get closer to the Equator and further away from nnEMF.
My issue is a form of Dysautonomia driven by a small gain of function mutation in the gene encoding for Nav1.7.
The results is a persistent Na+ leak in the neurons where Nav1.7 is expressed, resulting in hyperexcitability of these neurons.
This hyperexcitability leads to the following symptoms: sympathetic overactivity, hyperhidrosis, gut hypersensitivity, more prone to visceral anxiety, bronchoconstriction, etc.
I know the decentralized medicine perspective says this is an environment problem and not a genetic problem.
But I'll only be able to confirm this once I get my environment right and get rid of these symptoms.
Best,
Alex
How can my neurons help Alex?
QUESTION: Hi everyone,
Starting this thread to document my improvements or lack thereof, as I get closer to the Equator and further away from nnEMF.
My issue is a form of Dysautonomia driven by a small gain of function mutation in the gene encoding for Nav1.7.
The results is a persistent Na+ leak in the neurons where Nav1.7 is expressed, resulting in hyperexcitability of these neurons.
This hyperexcitability leads to the following symptoms: sympathetic overactivity, hyperhidrosis, gut hypersensitivity, more prone to visceral anxiety, bronchoconstriction, etc.
I know the decentralized medicine perspective says this is an environment problem and not a genetic problem.
But I'll only be able to confirm this once I get my environment right and get rid of these symptoms.
Best,
Alex
How can my neurons help Alex?
2. ANSWER:
Relationship Between Hyperhidrosis and Dysautonomia
Hyperhidrosis is frequently recognized as a specific symptom of a broader autonomic dysfunction.
In cases involving the upper neck:
1. Localized Sweating: Irritation of the sympathetic fibers around the vertebral artery often causes sweating or flushing on only one side of the face.
2. Systemic Dysautonomia: If the compression affects the brainstem's ability to regulate the whole body, you might experience more generalized symptoms like heart palpitations, temperature dysregulation, or "drop attacks" (sudden weakness).
3. Other relationships to be explored are found below
A. Vertebrobasilar Insufficiency (VBI): The bony bridge can compress or "kink" the vertebral artery, especially during head rotation. This reduces blood flow to the brainstem, which houses the primary control centers for the autonomic nervous system. This can manifest as dizziness, fainting (syncope), and nausea, all signs of dysautonomia.
B. Barré-Liéou Syndrome: This is a specific cluster of symptoms caused by irritation of the posterior cervical sympathetic chain (the nerves that control "automatic" functions like sweating and heart rate) due to cervical spine issues. Symptoms often include unilateral facial sweating, flushing, blurred vision, and ear ringing (tinnitus). Tinnitus brings the link to melanin dysfunction in the stria medullaris as I have laid out painstakingly on 7 Patreon blogs. It signifies an nnEMF etiology to the Hyperhidrosis and dysautonomia.
C. Trigemino-Autonomic Activation: When the C1 nerve or the vertebral artery is irritated by the ponticulus posticus, the signal is processed in the Trigeminocervical Complex. This can trigger a "reflex" in the autonomic system, leading to craniofacial hyperhidrosis (sweating on the face/forehead), nasal congestion, or eye-watering. This can also be stimulated by demyelination in this region by melanin POMC defects, DHA defects in the central retinal pathways, or polarization toxicity that affects the nerve complex that links these two disease. Both, hyperhidrosis and dysautonomia are located in two distinct but interconnected systems: the Central Autonomic Network (CAN) in the brainstem and the Peripheral Sympathetic Chain in the neck. Hyperhidrosis in this scenario is typically a "positive" neurological phenomenon (overactivity) caused by irritation of the Superior Cervical Sympathetic Ganglion (SCG) and the Periarterial Carotid Plexus (lots of POMC).
Relationship Between Hyperhidrosis and Dysautonomia
Hyperhidrosis is frequently recognized as a specific symptom of a broader autonomic dysfunction.
In cases involving the upper neck:
1. Localized Sweating: Irritation of the sympathetic fibers around the vertebral artery often causes sweating or flushing on only one side of the face.
2. Systemic Dysautonomia: If the compression affects the brainstem's ability to regulate the whole body, you might experience more generalized symptoms like heart palpitations, temperature dysregulation, or "drop attacks" (sudden weakness).
3. Other relationships to be explored are found below
A. Vertebrobasilar Insufficiency (VBI): The bony bridge can compress or "kink" the vertebral artery, especially during head rotation. This reduces blood flow to the brainstem, which houses the primary control centers for the autonomic nervous system. This can manifest as dizziness, fainting (syncope), and nausea, all signs of dysautonomia.
B. Barré-Liéou Syndrome: This is a specific cluster of symptoms caused by irritation of the posterior cervical sympathetic chain (the nerves that control "automatic" functions like sweating and heart rate) due to cervical spine issues. Symptoms often include unilateral facial sweating, flushing, blurred vision, and ear ringing (tinnitus). Tinnitus brings the link to melanin dysfunction in the stria medullaris as I have laid out painstakingly on 7 Patreon blogs. It signifies an nnEMF etiology to the Hyperhidrosis and dysautonomia.
C. Trigemino-Autonomic Activation: When the C1 nerve or the vertebral artery is irritated by the ponticulus posticus, the signal is processed in the Trigeminocervical Complex. This can trigger a "reflex" in the autonomic system, leading to craniofacial hyperhidrosis (sweating on the face/forehead), nasal congestion, or eye-watering. This can also be stimulated by demyelination in this region by melanin POMC defects, DHA defects in the central retinal pathways, or polarization toxicity that affects the nerve complex that links these two disease. Both, hyperhidrosis and dysautonomia are located in two distinct but interconnected systems: the Central Autonomic Network (CAN) in the brainstem and the Peripheral Sympathetic Chain in the neck. Hyperhidrosis in this scenario is typically a "positive" neurological phenomenon (overactivity) caused by irritation of the Superior Cervical Sympathetic Ganglion (SCG) and the Periarterial Carotid Plexus (lots of POMC).
3. ANSWER CONTINUES
The broader "dysautonomia" (dizziness, heart rate changes, nausea) stems from a defect in the Lower Brainstem, specifically the Nucleus Tractus Solitarius (NTS) and the Ventrolateral Medulla. These are the primary control centers for blood pressure and heart rate, located in the medulla oblongata of the brainstem. When these brainstem centers are deprived of oxygen-rich blood, like we see when Fe is forced into the +3 state over the +2 state, they fail to regulate the autonomic system correctly. This is why nnEMF can cause this syndrome. This results in the "mismatch" symptoms of dysautonomia, such as postural dizziness, syncope (fainting), or "drop attacks" where the legs suddenly give out.
Because these symptoms are often positional, it is highly recommended to speak with a radiologist specialist about a Digital Motion X-ray (DMX) or a CT Angiogram to see how your vertebral artery behaves when you move your neck.
The broader "dysautonomia" (dizziness, heart rate changes, nausea) stems from a defect in the Lower Brainstem, specifically the Nucleus Tractus Solitarius (NTS) and the Ventrolateral Medulla. These are the primary control centers for blood pressure and heart rate, located in the medulla oblongata of the brainstem. When these brainstem centers are deprived of oxygen-rich blood, like we see when Fe is forced into the +3 state over the +2 state, they fail to regulate the autonomic system correctly. This is why nnEMF can cause this syndrome. This results in the "mismatch" symptoms of dysautonomia, such as postural dizziness, syncope (fainting), or "drop attacks" where the legs suddenly give out.
Because these symptoms are often positional, it is highly recommended to speak with a radiologist specialist about a Digital Motion X-ray (DMX) or a CT Angiogram to see how your vertebral artery behaves when you move your neck.
4. Alex brings me some new data.
Just received my results from biochemical Mitochondria testing by MitoSwab, a buccal mitochondria enzyme assay.
Not sure what Jack would think of these type of tests but my result clearly indicate my issue is a mitochondrial dysfunction:
- citrate synthase (mitochondrial content): 60% of mean → low-normal
- respiratory chain complex I (RC-I): 131% of mean → normal-high
- respiratory chain complex II (RC-II): 54% of mean → low-normal
- respiratory chain complex II + III (RC-II+III): 174% of mean → slightly elevated
- respiratory chain complex IV (RC-IV): 355% of mean → massively elevated
Overall No mitochondrial deficiency with preserved electron entry (complex I & II) BUT extreme overactivity of complex IV relative to mitochondrial content shows mitochondria are over-driven, with a strong compensatory upregulation of the terminal oxygen-consuming step (complex IV).
Just received my results from biochemical Mitochondria testing by MitoSwab, a buccal mitochondria enzyme assay.
Not sure what Jack would think of these type of tests but my result clearly indicate my issue is a mitochondrial dysfunction:
- citrate synthase (mitochondrial content): 60% of mean → low-normal
- respiratory chain complex I (RC-I): 131% of mean → normal-high
- respiratory chain complex II (RC-II): 54% of mean → low-normal
- respiratory chain complex II + III (RC-II+III): 174% of mean → slightly elevated
- respiratory chain complex IV (RC-IV): 355% of mean → massively elevated
Overall No mitochondrial deficiency with preserved electron entry (complex I & II) BUT extreme overactivity of complex IV relative to mitochondrial content shows mitochondria are over-driven, with a strong compensatory upregulation of the terminal oxygen-consuming step (complex IV).
5. ANSWER
Complex IV: Massively Elevated (355%)
This is the most striking part of your result. In mitochondrial diagnostics, a massively elevated Complex IV often represents a compensatory response.
Implications? Your cells are trying to "overclock" the final step of the energy production line because earlier steps (like Complex II) are failing.
Link to Symptoms: Complex IV (Cytochrome c Oxidase) is the "oxygen sink." If it's hyperactive, you may be experiencing high levels of oxidative stress or "leaking" electrons. This is the nnEMF trigger you missed. This can lead to central sensitization because the brainstem and nerves (like the C1 and Trigeminal convergence) become hypersensitive, turning minor mechanical irritation in your neck motions into your two symptoms in the brainstem likely causing slight de melanation and demyelination as the blogs lay out.
Complex IV: Massively Elevated (355%)
This is the most striking part of your result. In mitochondrial diagnostics, a massively elevated Complex IV often represents a compensatory response.
Implications? Your cells are trying to "overclock" the final step of the energy production line because earlier steps (like Complex II) are failing.
Link to Symptoms: Complex IV (Cytochrome c Oxidase) is the "oxygen sink." If it's hyperactive, you may be experiencing high levels of oxidative stress or "leaking" electrons. This is the nnEMF trigger you missed. This can lead to central sensitization because the brainstem and nerves (like the C1 and Trigeminal convergence) become hypersensitive, turning minor mechanical irritation in your neck motions into your two symptoms in the brainstem likely causing slight de melanation and demyelination as the blogs lay out.
6. Complex II: Low-Normal (54%)
Complex II is unique because it is the only part of the ETC that is also a direct member of the Krebs Cycle (Succinate Dehydrogenase). This links it to the TCA cycle. The blogs have a lot to say about this. TCA cycle is critical in myelin biology too. A deficit here suggests a bottleneck in the TCA cycle. You aren't processing fuel efficiently at the entry point. My bet = deuterium blockade of TCA .
Complex II dysfunction is strongly associated with autonomic nervous system instability. When energy supply to the medulla (brainstem) is inconsistent due to this bottleneck, it can cause the "glitches" you feel, like hyperhidrosis and heart rate variability.
Complex II is unique because it is the only part of the ETC that is also a direct member of the Krebs Cycle (Succinate Dehydrogenase). This links it to the TCA cycle. The blogs have a lot to say about this. TCA cycle is critical in myelin biology too. A deficit here suggests a bottleneck in the TCA cycle. You aren't processing fuel efficiently at the entry point. My bet = deuterium blockade of TCA .
Complex II dysfunction is strongly associated with autonomic nervous system instability. When energy supply to the medulla (brainstem) is inconsistent due to this bottleneck, it can cause the "glitches" you feel, like hyperhidrosis and heart rate variability.
7. Citrate Synthase: Low-Normal (60%)
Citrate Synthase is a marker of mitochondrial density (how many mitochondria you actually have).
What it means: You have a lower-than-average population of mitochondria per cell based on this # = mitochondrial biogenesis failure.
Link to Symptoms: With fewer "engines" (mitochondria) and a bottleneck at Complex II, your body has very little buffer for stress.
Physical triggers, like turning your head and slightly compressing the vertebral artery, nnEMF, lack of melanin, drain your remaining "battery" instantly, leading to dizziness or pain flare-ups.
Citrate Synthase is a marker of mitochondrial density (how many mitochondria you actually have).
What it means: You have a lower-than-average population of mitochondria per cell based on this # = mitochondrial biogenesis failure.
Link to Symptoms: With fewer "engines" (mitochondria) and a bottleneck at Complex II, your body has very little buffer for stress.
Physical triggers, like turning your head and slightly compressing the vertebral artery, nnEMF, lack of melanin, drain your remaining "battery" instantly, leading to dizziness or pain flare-ups.
8. Complex I: Normal-High (131%)
Complex I is where electrons from NADH enter the chain. Your "entry gate" for carbohydrates/proteins remains wide open, but since Complex II is low, the system is unbalanced. This often leads to a "backpressure" of electrons in ETC, which increases Reactive Oxygen Species (ROS). ROS production = aberrent UPE transformation = disease symptoms.
Your symptoms = The "Perfect nnEMF melanin Storm"
Your symptoms are likely a combination of structural and metabolic factors linked to melanin loss and mitochondrial chelation issues that cause alien UPE formation. DHA can shield a lot of this. So can CT, but melanin renovation and a strict circadian light diet are critical.
In the paradigm of Quantum Biology and decentralized medicine, your biochemical data and anatomy suggest a decoupled light-water-magnetism system. Your symptoms represent a classic "Perfect Storm" where nnEMF (non-native electromagnetic fields)and low solar yield meet a compromised mitochondrial engine.
Complex I is where electrons from NADH enter the chain. Your "entry gate" for carbohydrates/proteins remains wide open, but since Complex II is low, the system is unbalanced. This often leads to a "backpressure" of electrons in ETC, which increases Reactive Oxygen Species (ROS). ROS production = aberrent UPE transformation = disease symptoms.
Your symptoms = The "Perfect nnEMF melanin Storm"
Your symptoms are likely a combination of structural and metabolic factors linked to melanin loss and mitochondrial chelation issues that cause alien UPE formation. DHA can shield a lot of this. So can CT, but melanin renovation and a strict circadian light diet are critical.
In the paradigm of Quantum Biology and decentralized medicine, your biochemical data and anatomy suggest a decoupled light-water-magnetism system. Your symptoms represent a classic "Perfect Storm" where nnEMF (non-native electromagnetic fields)and low solar yield meet a compromised mitochondrial engine.
9. ANSWER CONTINUES
A mutation in the SCN9A gene which is the Nav 1.7 mutation you mentioned is the gasoline on your mitochondrial fire.
This creates a state of permanent depolarization of VGCCs, making your nerves functionally "leaky batteries" that can never fully recharge. This means photoerepair becomes mandatory. nnEMF elimination is critical.
Nav1.7 is highly concentrated in nociceptors (pain-sensing neurons) and the trigeminal ganglion.
The Defect: Normally, these channels stay closed until a threshold is met. Your "leak" means the resting membrane potential is sitting right at the edge of firing.
The Link: When a structural defect in your neck around the nerves that link to these syndromes even slighty irritates the vertebral artery (melanopsin damage), your hyper-excitable Nav1.7 channels "fire" immediately. Because of the convergence in the Trigeminocervical Complex, your brain perceives this as a chronic activation syndrome. You have a structural trigger acting on a genetically "explosive" nerve complex. It could be melanopsin damage to your VB circulation too.
The Mitochondrial Death Spiral (The Bioenergetic Cost)
This is why your Complex IV is at 355%.
The Pump: To counteract a persistent Na+ leak, your neurons must run the Na+/K+-ATPase pump at maximum capacity 24/7 to try and push the sodium back out.
A mutation in the SCN9A gene which is the Nav 1.7 mutation you mentioned is the gasoline on your mitochondrial fire.
This creates a state of permanent depolarization of VGCCs, making your nerves functionally "leaky batteries" that can never fully recharge. This means photoerepair becomes mandatory. nnEMF elimination is critical.
Nav1.7 is highly concentrated in nociceptors (pain-sensing neurons) and the trigeminal ganglion.
The Defect: Normally, these channels stay closed until a threshold is met. Your "leak" means the resting membrane potential is sitting right at the edge of firing.
The Link: When a structural defect in your neck around the nerves that link to these syndromes even slighty irritates the vertebral artery (melanopsin damage), your hyper-excitable Nav1.7 channels "fire" immediately. Because of the convergence in the Trigeminocervical Complex, your brain perceives this as a chronic activation syndrome. You have a structural trigger acting on a genetically "explosive" nerve complex. It could be melanopsin damage to your VB circulation too.
The Mitochondrial Death Spiral (The Bioenergetic Cost)
This is why your Complex IV is at 355%.
The Pump: To counteract a persistent Na+ leak, your neurons must run the Na+/K+-ATPase pump at maximum capacity 24/7 to try and push the sodium back out.
10. The Pump: To counteract a persistent Na+ leak, your neurons must run the Na+/K+-ATPase pump at maximum capacity 24/7 to try and push the sodium back out.
The Energy Drain: This pump consumes roughly 2/3 of all ATP in a neuron. Your mitochondria (already low in density per your 60% Citrate Synthase) are being "overclocked" to keep the cell from dying due to sodium overload.
Result: This massive ATP demand drives the Complex IV hyper-activity, leading to the "Alien UPE" (photon leakage) I discussed above. You are burning through your "battery" just to stay at baseline.
Dysautonomia and Hyperhidrosis
Do your centralized experts in France know that Nav1.7 is also expressed in sympathetic ganglion neurons?
Autonomic Misfiring: The Na+ leak makes your sympathetic "fight or flight" nerves hyperexcitable.
The Symptom: This directly causes hyperhidrosis. Even without a stressor, your sympathetic nerves are "leaking" signals to your sweat glands. When you combine this with the Barré-Liéou irritation from anywhere in your neck close to the sympathetic chain, the sweating becomes profuse and difficult to control.
The Energy Drain: This pump consumes roughly 2/3 of all ATP in a neuron. Your mitochondria (already low in density per your 60% Citrate Synthase) are being "overclocked" to keep the cell from dying due to sodium overload.
Result: This massive ATP demand drives the Complex IV hyper-activity, leading to the "Alien UPE" (photon leakage) I discussed above. You are burning through your "battery" just to stay at baseline.
Dysautonomia and Hyperhidrosis
Do your centralized experts in France know that Nav1.7 is also expressed in sympathetic ganglion neurons?
Autonomic Misfiring: The Na+ leak makes your sympathetic "fight or flight" nerves hyperexcitable.
The Symptom: This directly causes hyperhidrosis. Even without a stressor, your sympathetic nerves are "leaking" signals to your sweat glands. When you combine this with the Barré-Liéou irritation from anywhere in your neck close to the sympathetic chain, the sweating becomes profuse and difficult to control.
11. How to "Plug the Leak" (Quantum Strategy of Decentralized Medicine)
Standard pain meds often fail here because they don't address the electric potential defects.
DHA is Non-Negotiable: DHA doesn't just shield EMF; it integrates into the cell membrane to stabilize the voltage gate. It acts as the "insulation" to stop the Na+ leak.
Extreme Cold (CT): Cold increases the viscosity of the cell membrane and slows down the kinetic movement of ions. This can "mechanically" help close the leaky Nav1.7 gates and lower the metabolic demand on your mitochondria.
SUNLIGHT IS THE BEST CALCIUM CHANNEL BLOCKER ON THE PLANET. USE it to renovate melanin and myelin to stop hyper neuronal activation.
Non savage idea will be Magnesium & Topicals uses for this: Magnesium acts as a natural calcium-channel blocker and stabilizes membranes. Topical Magnesium on the suboccipital area (C1) and neck region may help dampen the local hyperexcitability but this is a half truth action.
This is how decentralized medicine operates, Alex
Standard pain meds often fail here because they don't address the electric potential defects.
DHA is Non-Negotiable: DHA doesn't just shield EMF; it integrates into the cell membrane to stabilize the voltage gate. It acts as the "insulation" to stop the Na+ leak.
Extreme Cold (CT): Cold increases the viscosity of the cell membrane and slows down the kinetic movement of ions. This can "mechanically" help close the leaky Nav1.7 gates and lower the metabolic demand on your mitochondria.
SUNLIGHT IS THE BEST CALCIUM CHANNEL BLOCKER ON THE PLANET. USE it to renovate melanin and myelin to stop hyper neuronal activation.
Non savage idea will be Magnesium & Topicals uses for this: Magnesium acts as a natural calcium-channel blocker and stabilizes membranes. Topical Magnesium on the suboccipital area (C1) and neck region may help dampen the local hyperexcitability but this is a half truth action.
This is how decentralized medicine operates, Alex
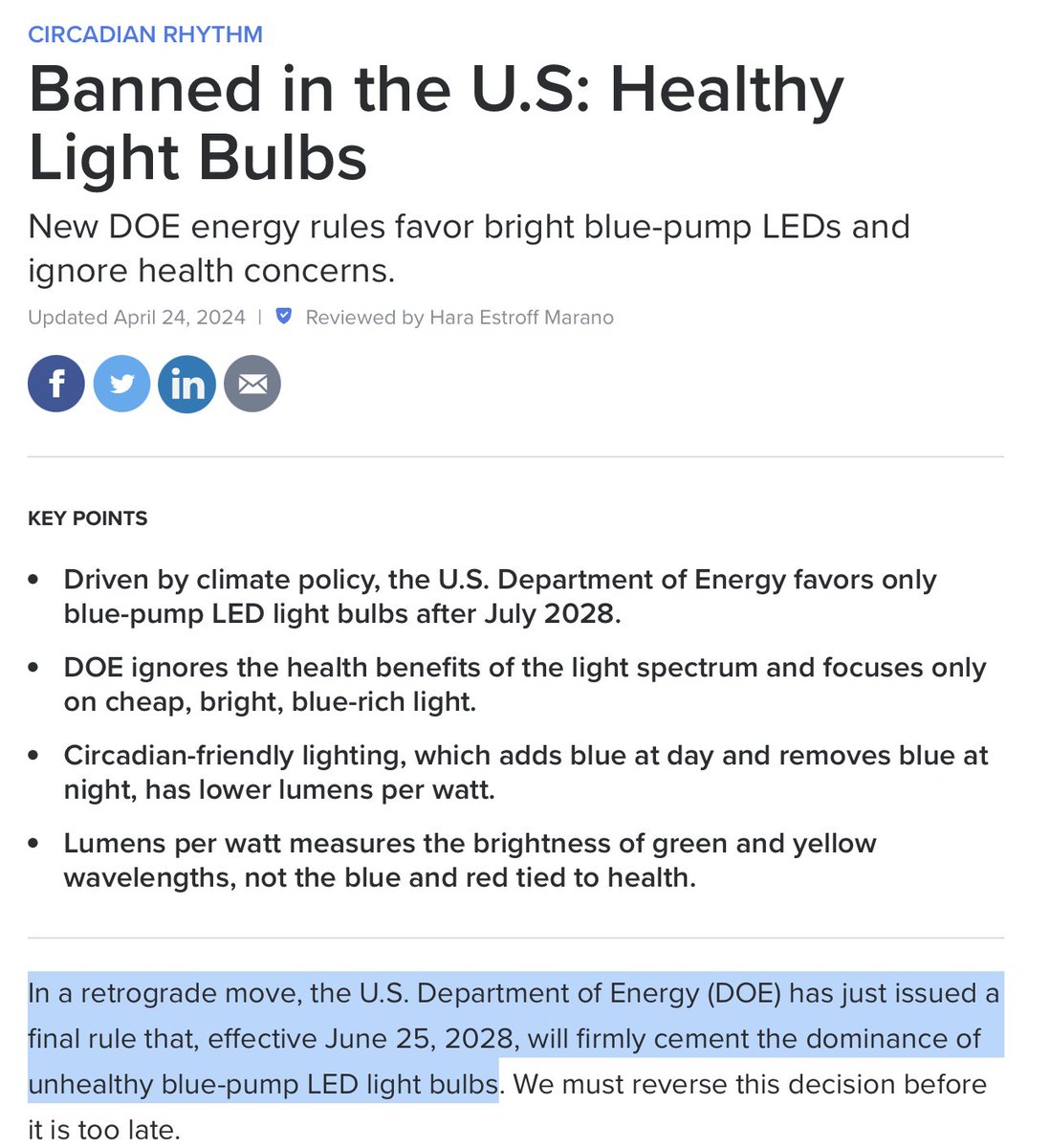
12. Given the Nav1.7 leak and Complex IV surge, you should noticed that your pain and sweating get significantly worse in environments with high nnEMF (like under LED lights or near Wi-Fi routers), which further destabilizes voltage-gated channels. This would be diagnostic confirmation of your mitoSwab results, FYI.

13. WNT10A is a critical ligand for the canonical β-catenin pathway, which regulates the proliferation and specialized differentiation of adult epithelial progenitors in sweat ducts.
The most likely cause is atrophic skin from a lack of sun. Getting this after pregnancy means the baby stole the person DHA, Vitamin D and you lost more surface and endogenous melanin due to your lack of sunlight as baby grew. Another perfect storm that pushed your biology back to the GOE.
Localized Over-secretion: While mutations generally cause sweat duct regression, the localized hyperhidrosis on palms and soles is believed to stem from variable compensatory mechanisms due to melanin loss or myelin loss in the nerve that innervate the sweat ducts.
Barrier Defects = Vitamin A problems = ROR/RXR blindness due to nnEMF abuse: Loss of WNT10A causes a deficiency in specialized keratins (like KRT9), leading to a thinner or abnormal epidermal barrier. This can cause localized "leakiness" or a mismatch in the autonomic sudomotor response, where the body over-activates specific sweat glands to compensate for a failing skin barrier or heat regulation issues elsewhere.
The most likely cause is atrophic skin from a lack of sun. Getting this after pregnancy means the baby stole the person DHA, Vitamin D and you lost more surface and endogenous melanin due to your lack of sunlight as baby grew. Another perfect storm that pushed your biology back to the GOE.
Localized Over-secretion: While mutations generally cause sweat duct regression, the localized hyperhidrosis on palms and soles is believed to stem from variable compensatory mechanisms due to melanin loss or myelin loss in the nerve that innervate the sweat ducts.
Barrier Defects = Vitamin A problems = ROR/RXR blindness due to nnEMF abuse: Loss of WNT10A causes a deficiency in specialized keratins (like KRT9), leading to a thinner or abnormal epidermal barrier. This can cause localized "leakiness" or a mismatch in the autonomic sudomotor response, where the body over-activates specific sweat glands to compensate for a failing skin barrier or heat regulation issues elsewhere.
14. When human embryonic sweat gland germs develop normally, but the ducts fail to extend or maintain themselves postnatally due to decreased basal cell proliferation it is usually due to a lack of light. This problem is also present in psoriasis which is associated with basal skin problems.
This often creates a "dry skin" phenotype over most of the body (hypohidrosis). The hyperhidrosis seen in Odonto-onycho-dermal dysplasia (OODD) is localized specifically to ectodermal derivatives (palms/soles) where the structural "glitch" in Wnt-active stem cells results in an uncontrolled or hyper-reactive secretory response from the remaining glands.
WNT10A is also expressed in the central nervous system (including the medulla and spinal cord) and has been linked to neuropathic pain pathwaysand synaptic function. WNT10A: Mutations cause severe hypodontia (missing teeth) and malformed tooth roots.
Oxalate is a potent inhibitor of Succinate Dehydrogenase (Complex II) because it competes with succinate for the active site.
The Mechanism: Oxalate mimics the structure of dicarboxylic acids. When it binds to Complex II, it completely halts the Krebs cycle and electron entry at that point. This is why people with oxalate issues need AM sun to make the TCA kickstart again.
They need to overdose on sunlight because their mitochondria are effectively chronically depolarized. This is why their skin is atrophic and lacks melanin and nerves lack myelin.
This situation worsens the existing bottlenecks cause by oxalate dumping because it forces Complex IV (CCO) to work even harder to maintain a membrane potential, which accelerates their "Alien UPEs" creation ( Popp's photon leakage) to cause all their symptoms. It can get so bad it can put you in bed like you are a cripple. Most centralized docs have zero clue about how Kreb's bicycle operates in these situations. No AM sunlight = no CCO renovation = no DDW = no TCA use.
This often creates a "dry skin" phenotype over most of the body (hypohidrosis). The hyperhidrosis seen in Odonto-onycho-dermal dysplasia (OODD) is localized specifically to ectodermal derivatives (palms/soles) where the structural "glitch" in Wnt-active stem cells results in an uncontrolled or hyper-reactive secretory response from the remaining glands.
WNT10A is also expressed in the central nervous system (including the medulla and spinal cord) and has been linked to neuropathic pain pathwaysand synaptic function. WNT10A: Mutations cause severe hypodontia (missing teeth) and malformed tooth roots.
Oxalate is a potent inhibitor of Succinate Dehydrogenase (Complex II) because it competes with succinate for the active site.
The Mechanism: Oxalate mimics the structure of dicarboxylic acids. When it binds to Complex II, it completely halts the Krebs cycle and electron entry at that point. This is why people with oxalate issues need AM sun to make the TCA kickstart again.
They need to overdose on sunlight because their mitochondria are effectively chronically depolarized. This is why their skin is atrophic and lacks melanin and nerves lack myelin.
This situation worsens the existing bottlenecks cause by oxalate dumping because it forces Complex IV (CCO) to work even harder to maintain a membrane potential, which accelerates their "Alien UPEs" creation ( Popp's photon leakage) to cause all their symptoms. It can get so bad it can put you in bed like you are a cripple. Most centralized docs have zero clue about how Kreb's bicycle operates in these situations. No AM sunlight = no CCO renovation = no DDW = no TCA use.

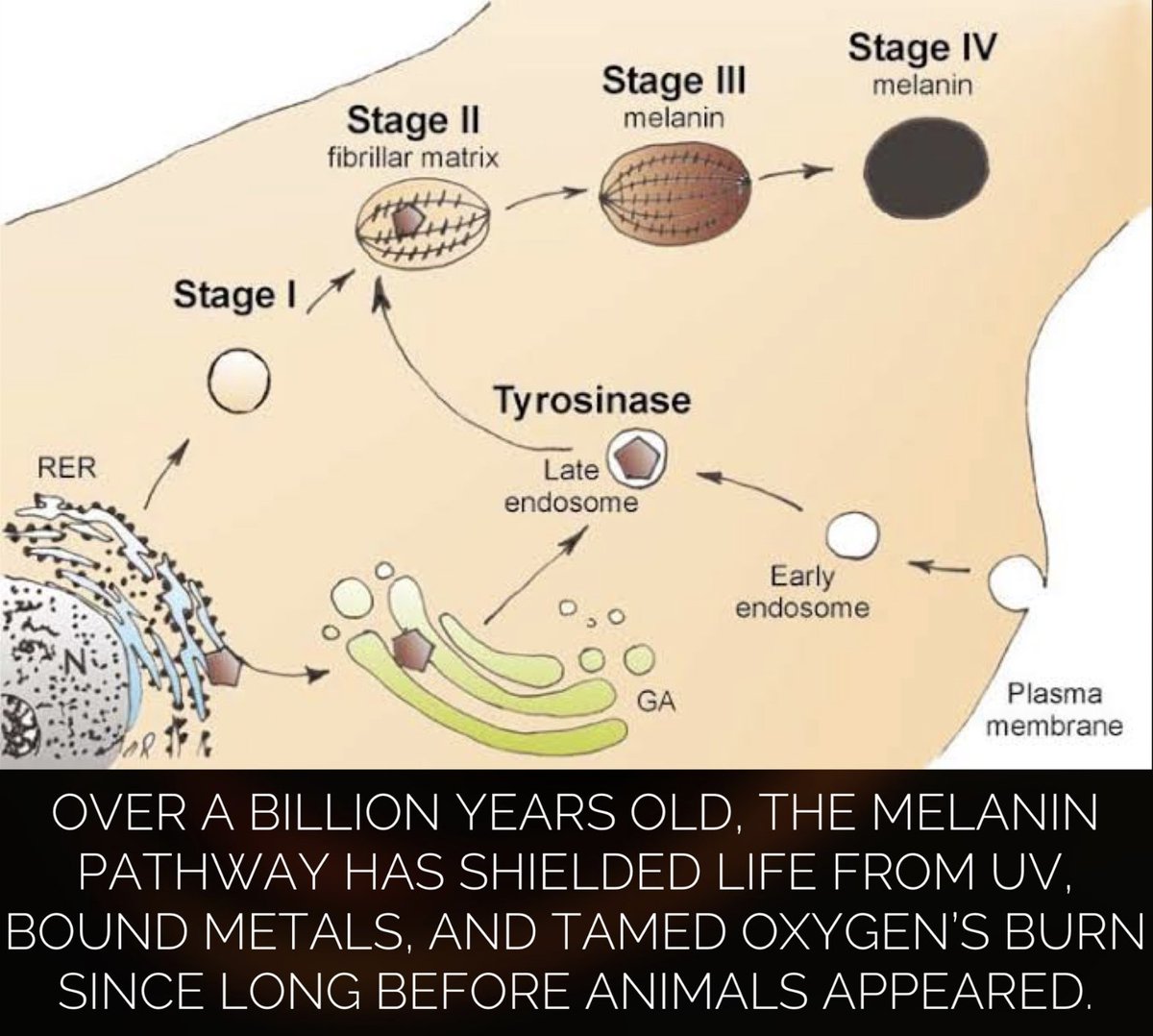
15. Chelation of Matrix Metal Ions (Fe, Mn, Cu) = oxalate problem = why their mitochondria are demolished = no melanin controller. People forget that melanin main evolutionary roles was to control the dirty chemistry that existed in the GOE. Melanin is a metal chelator for these dirty metals that destroy mitochondrial function.
Oxalate has an extreme affinity for positively charged metal ions, forming insoluble crystals or stable complexes that "strip" the matrix of its functional catalysts:
Manganese (Mn) & SOD2: Oxalate chelates Mn2+, the essential cofactor for Manganese Superoxide Dismutase (SOD2). Without Mn, your mitochondria cannot neutralize the superoxide produced by your overactive Complex IV. This leads to massive oxidative stress in the Trigeminocervical Complex = cause massive pain.
Iron (Fe) & Heme Groups: Oxalate can interfere with the availability of iron for Iron-Sulfur (Fe-S) clusters found in Complexes I, II, and III. This physically degrades the "wiring" of your electron transport chain = why they are energy vampires for themselves and others
Copper (Cu) & Complex IV: While your Complex IV is high, it requires Copper to function. High oxalate levels can sequester copper, potentially leading to the production of dysfunctional, "broken" Complex IV enzymes that consume oxygen but produce heat and ROS instead of ATP. You also cannot make DDW at CCO = makes all tissues deserts.
Oxalates disrupt the Melanin-Mitochondria link by depleting the cell of Molybdenum (Mo) and Copper. These are required for tyrosinase (melanin production) and sulfite oxidase. This is why these people are PALE AS FUCK AND SICK AS FUCK.
A "Molybdenum dump" caused by oxalate toxicity prevents the detoxification of sulfites, which are neurotoxic and can trigger the hyperhidrosis and dysautonomia that many experience.
It is decnetralized medicine 101, Alex.
Now I am done with you. That is your answer.
Oxalate has an extreme affinity for positively charged metal ions, forming insoluble crystals or stable complexes that "strip" the matrix of its functional catalysts:
Manganese (Mn) & SOD2: Oxalate chelates Mn2+, the essential cofactor for Manganese Superoxide Dismutase (SOD2). Without Mn, your mitochondria cannot neutralize the superoxide produced by your overactive Complex IV. This leads to massive oxidative stress in the Trigeminocervical Complex = cause massive pain.
Iron (Fe) & Heme Groups: Oxalate can interfere with the availability of iron for Iron-Sulfur (Fe-S) clusters found in Complexes I, II, and III. This physically degrades the "wiring" of your electron transport chain = why they are energy vampires for themselves and others
Copper (Cu) & Complex IV: While your Complex IV is high, it requires Copper to function. High oxalate levels can sequester copper, potentially leading to the production of dysfunctional, "broken" Complex IV enzymes that consume oxygen but produce heat and ROS instead of ATP. You also cannot make DDW at CCO = makes all tissues deserts.
Oxalates disrupt the Melanin-Mitochondria link by depleting the cell of Molybdenum (Mo) and Copper. These are required for tyrosinase (melanin production) and sulfite oxidase. This is why these people are PALE AS FUCK AND SICK AS FUCK.
A "Molybdenum dump" caused by oxalate toxicity prevents the detoxification of sulfites, which are neurotoxic and can trigger the hyperhidrosis and dysautonomia that many experience.
It is decnetralized medicine 101, Alex.
Now I am done with you. That is your answer.



16. LESSON OVER.


• • •
Missing some Tweet in this thread? You can try to
force a refresh