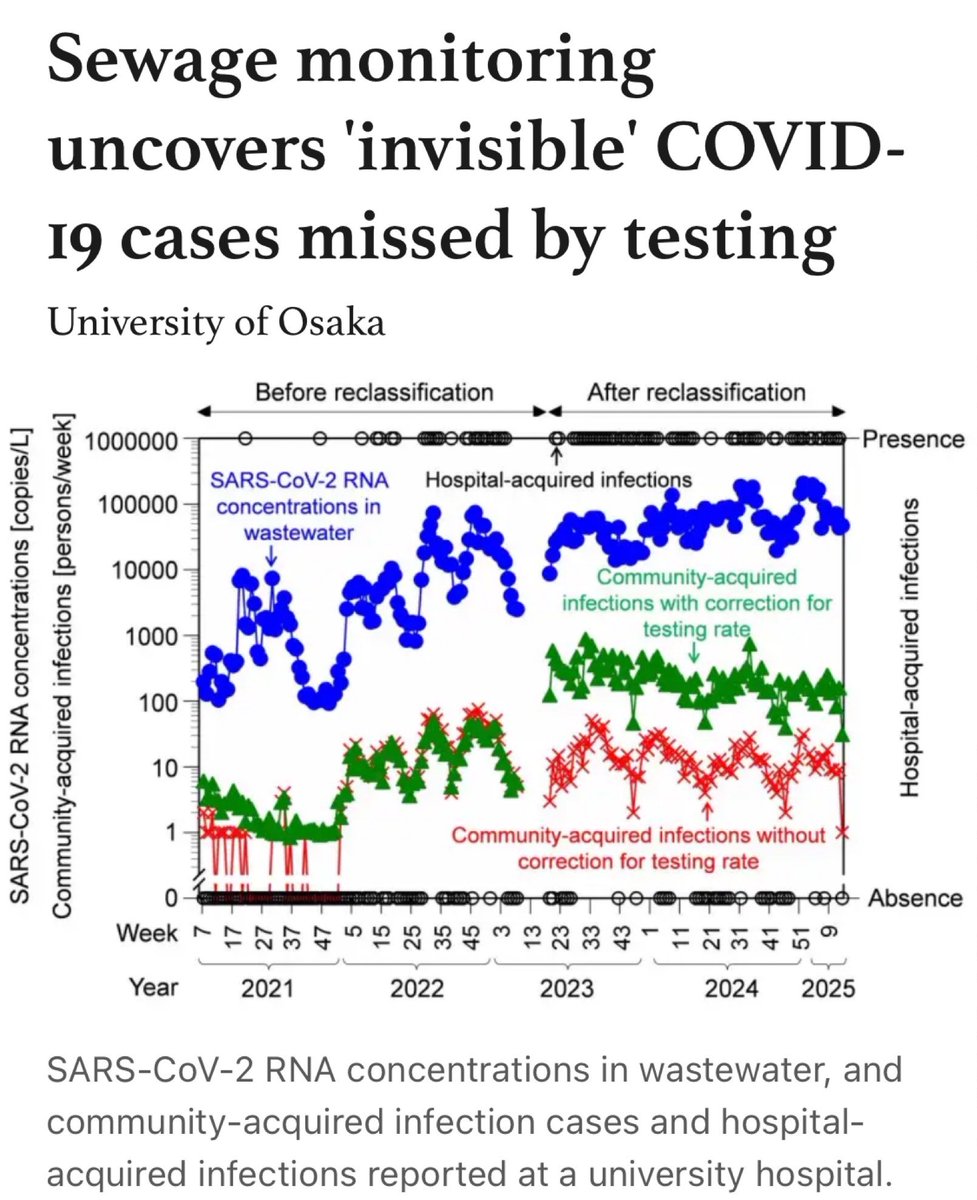
New study from Japan found after reclassifying COVID to a lower alert level, reported infections dropped sharply due to reduced testing, but wastewater continued detecting high viral loads, revealing invisible community spread including asymptomatic cases missed by testing alone. 
This is the kind of thing that occasionally crosses your mind while hospitalized for 5 days, but there’s not much you can do but trust your own N95.
medicalxpress.com/news/2026-01-s…
medicalxpress.com/news/2026-01-s…
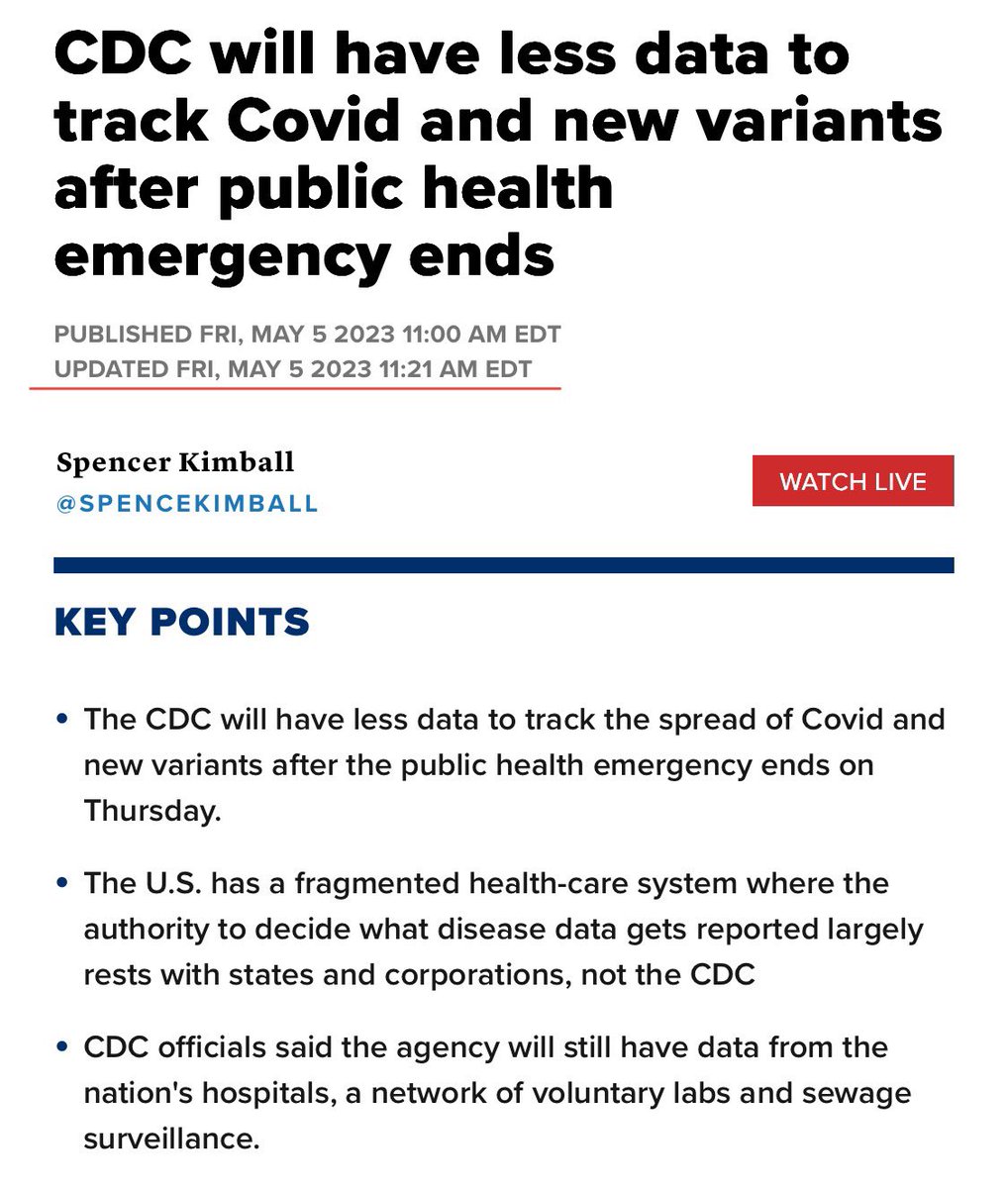
I woke up to being Quoted by Blue Maga blaming President Trump. This study analyzed changes in 2023. In the United States, we stopped mandatory reporting then downgraded it in 2024. Who was President when these policies went into effect?
You people are a societal plague.
You people are a societal plague.
If you’re Red Maga, the vaccine time travels. It’s responsible for things that occurred in 2020-21.
If you’re Blue Maga, the virus time travels. It was bad in 2020, went away 2021-2024, and now it’s back again.
Staggering levels of incompetence.
cnbc.com/amp/2023/05/05…
If you’re Blue Maga, the virus time travels. It was bad in 2020, went away 2021-2024, and now it’s back again.
Staggering levels of incompetence.
cnbc.com/amp/2023/05/05…
• • •
Missing some Tweet in this thread? You can try to
force a refresh