🧵What are the differences between Ketamine and Memantine - 🚨1/7
Both are NMDA antagonists - But with different clinical effects.
Here’s why 👇
Both are NMDA antagonists - But with different clinical effects.
Here’s why 👇
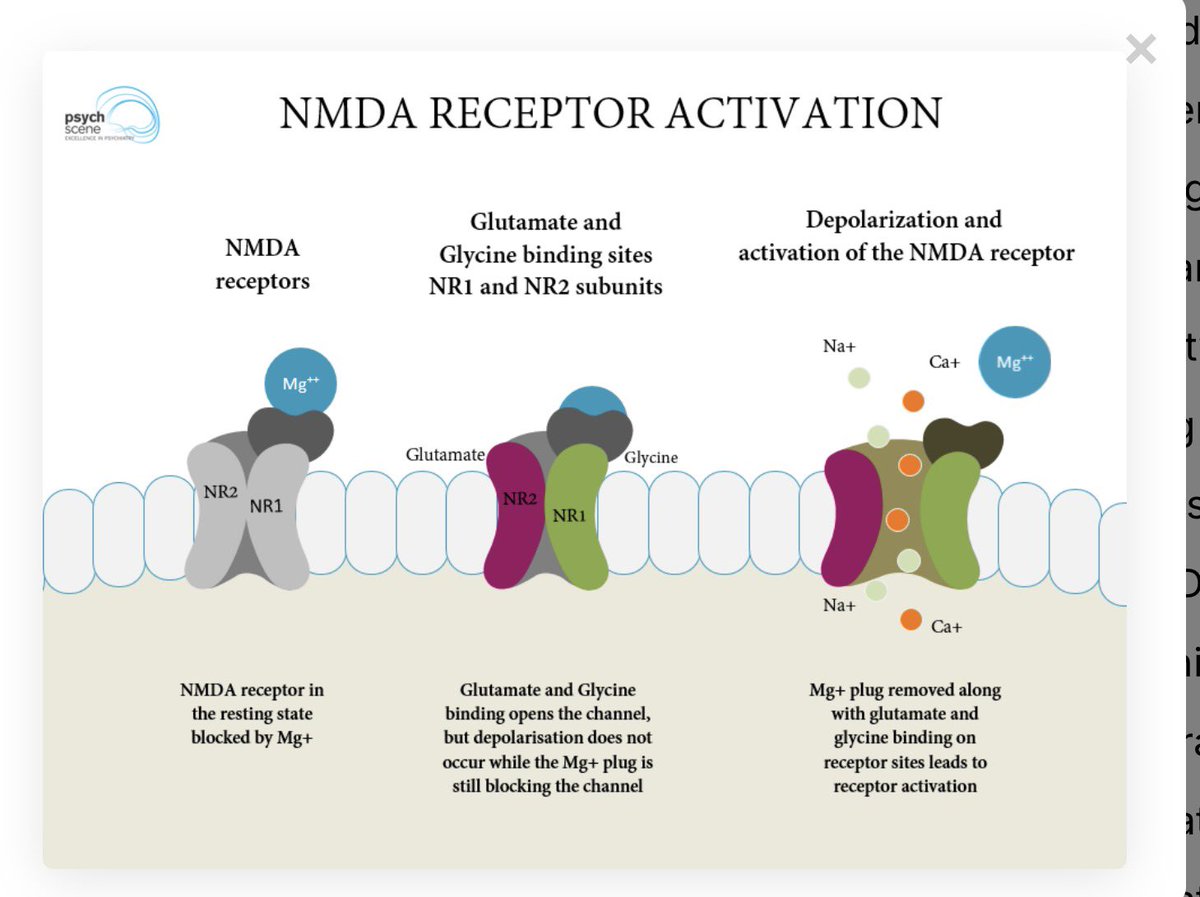
1/ Receptor selectivity
-Memantine → preferentially blocks extrasynaptic NMDARs (excitotoxic signalling)
-Ketamine → blocks synaptic + extrasynaptic NMDARs
- Ketamine is non-selective (muscarinic, monoaminergic, opioid effects → psychotomimetic profile)
-Memantine → preferentially blocks extrasynaptic NMDARs (excitotoxic signalling)
-Ketamine → blocks synaptic + extrasynaptic NMDARs
- Ketamine is non-selective (muscarinic, monoaminergic, opioid effects → psychotomimetic profile)
2/ Affinity & channel behaviour
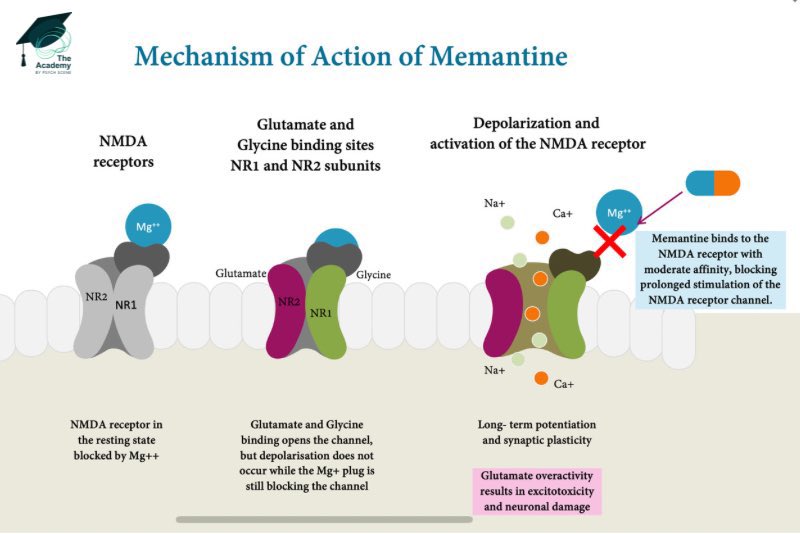
- Memantine: moderate affinity, fast unblocking, activity-dependent
- Ketamine: higher affinity, longer channel occupancy
Clinical relevance :
Memantine disengages during normal synaptic activity → good tolerability.
Ketamine’s longer occupancy contributes to dissociation and perceptual effects.
- Memantine: moderate affinity, fast unblocking, activity-dependent
- Ketamine: higher affinity, longer channel occupancy
Clinical relevance :
Memantine disengages during normal synaptic activity → good tolerability.
Ketamine’s longer occupancy contributes to dissociation and perceptual effects.
3/ NR2 subunit preference
- Memantine → GluN1/NR2A (LTP, prolonged glutamate exposure)
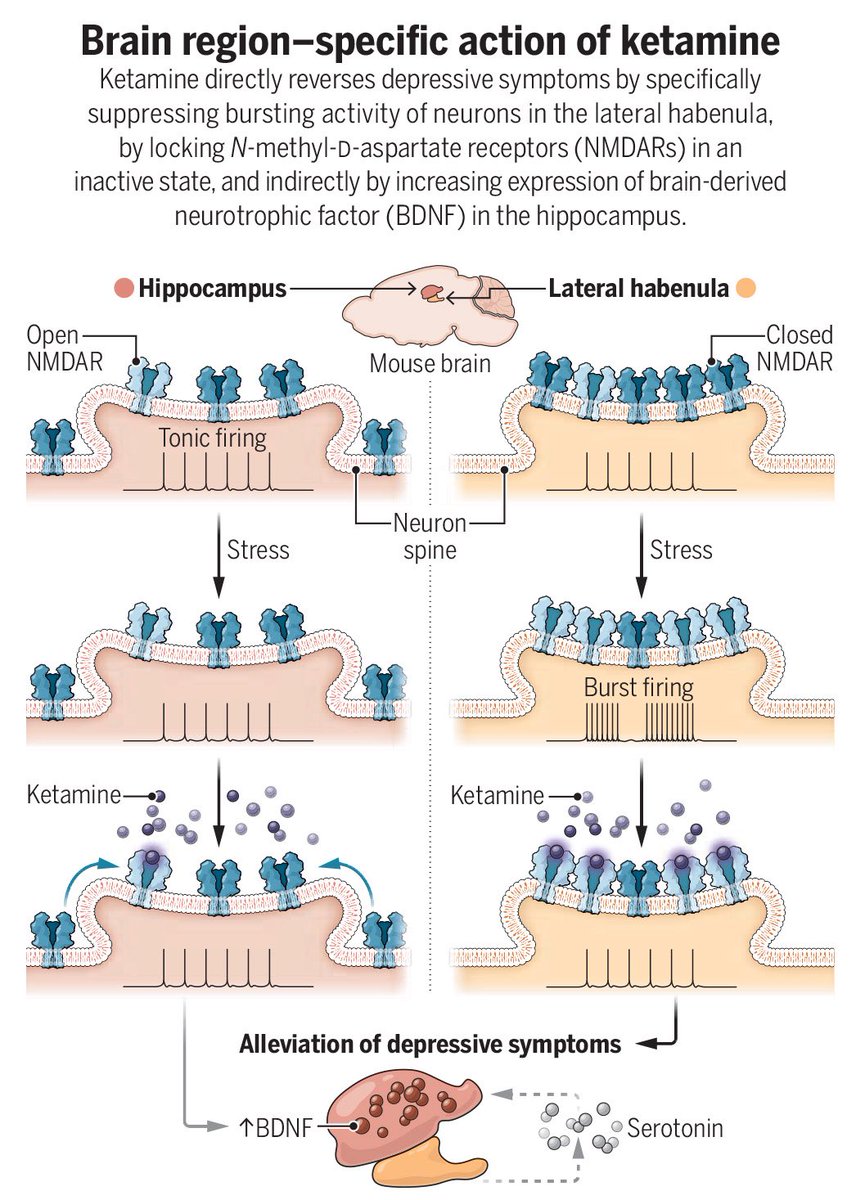
- Ketamine → GluN1/NR2B (LTD, brief glutamate bursts)
→ Memantine acts during pathological glutamate ‘flooding’
→ Ketamine acts during normal signalling bursts
- Memantine → GluN1/NR2A (LTP, prolonged glutamate exposure)
- Ketamine → GluN1/NR2B (LTD, brief glutamate bursts)
→ Memantine acts during pathological glutamate ‘flooding’
→ Ketamine acts during normal signalling bursts
4/ Calcium homeostasis
-Memantine stabilises Ca²⁺-dependent desensitised state
-Ketamine disrupts Ca²⁺ regulation (PMCA inhibition → glutamate surge)
-Memantine stabilises Ca²⁺-dependent desensitised state
-Ketamine disrupts Ca²⁺ regulation (PMCA inhibition → glutamate surge)
5/ Network effect
-Ketamine disinhibits pyramidal neurons (via GABA interneurons) → glutamate surge → antidepressant effect
-Memantine does not do this
-Ketamine disinhibits pyramidal neurons (via GABA interneurons) → glutamate surge → antidepressant effect
-Memantine does not do this
6/ Duration of binding
- Ketamine stays in channel longer → dissociation/sedation
- Memantine brief occupancy → cognitive tolerability
- Ketamine stays in channel longer → dissociation/sedation
- Memantine brief occupancy → cognitive tolerability
7/ Summary 🚨
👉Memantine dampens sustained, pathological NMDAR activity while preserving normal transmission → good tolerability; used in dementia and as adjunct where glutamatergic overactivity is suspected.
👉Ketamine transiently disrupts physiological NMDAR signalling via interneuronal disinhibition → rapid antidepressant effect with dissociative/psychotomimetic features.
I’ve covered all the above and more in the article below
psychscenehub.com/psychinsights/…
👉Memantine dampens sustained, pathological NMDAR activity while preserving normal transmission → good tolerability; used in dementia and as adjunct where glutamatergic overactivity is suspected.
👉Ketamine transiently disrupts physiological NMDAR signalling via interneuronal disinhibition → rapid antidepressant effect with dissociative/psychotomimetic features.
I’ve covered all the above and more in the article below
psychscenehub.com/psychinsights/…
• • •
Missing some Tweet in this thread? You can try to
force a refresh