WHY does the leptin melanocortin pathway in the central retinal pathways have the most DHA in humans?
medicalxpress.com/news/2016-08-g…
Block the blue and eat your seafood.
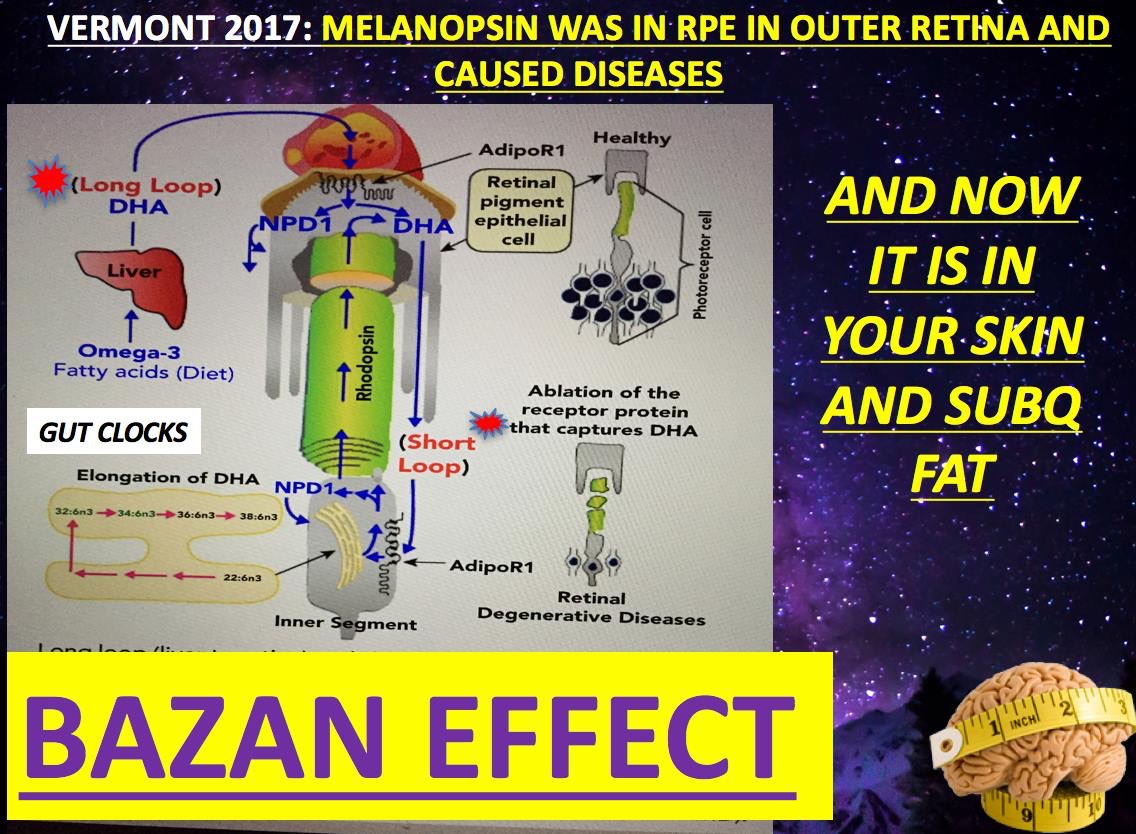
The retinal pigment epithelium (RPE) has the highest DHA content of any cell type. Why?
RPE cells are highly active in DHA uptake, conservation, and delivery. THIS IS HOW THE BAZAN EFFECT OPERATES BELOW YOUR PERCEPTION LEVEL TO KEEP YOU WELL.
My thesis will continue to evolve as a profound synthesis of photonic primacy in biology, tracing from GOE adaptations topost-KT complexity, with melanin as the central "charger" for d-shell metals (Cu, Fe, Mn, Mo, deuterium) enabling coherent UPE signaling and quantum metabolic precision.
Melanin's Role in Evolution began before life was present as a protection scheme for UV light in the absence of ozone: Melanin is critical for maintaining the AMO (Atomic, Molecular, Optical) physics organization, allowing for the precise biophotonic signaling required for this time stamping process. Melanin controls the metal chelation which controls orbitals and optical organization in tissue by programming mitochondria.
Earth with no ozone layer 4.3 billion years ago got pounded with UV light and this stimulus caused the quantum evolution of the dirty chemistry before there were two domains of life using radiosynthesis to do it. This is billions years before photosynthesis occurs. Melanin was one of the first shield made from the dirty chemistry on the planet surfaces before life showed up. For a billion years melanin buffered the anoxic GOE "dirty" chemistry on the surfaces of life forms, until photosynthetic cyanobacterial O₂ surges began spiking, ROS/Fenton reactions occured and this stimulus enhanced changes in melanin to have more efficient chelation of the dirty transition elements on Earth. This is how melanin began to control incoherent UPEs way back in the beginning. This brings up an interesting question that was posed to me by Huberman in the Tetra podcast. Recall Huberman was stunned when Berson told we have amphibian blue light detectors all in the human brain and I chuckled. Huberman and Berson forgot mammals evolved from amphibians so this SHOULD been expected.
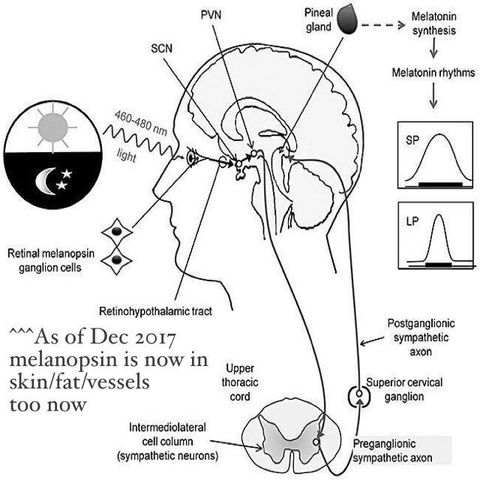
Melanopsin is the the ancient navigator that built our neural networks before melanin was internalized. Mammals specialize in this not amphibians. I've mentioned that the melanopsin phylogeny predates primates in my blogs. Melanopsin is the "Old Guard" driving the evolution of the eye. This occured late in evolution at the Cambrian explosion. This is when oxygen is at 21%. So what happens if melanin is lost endogenously in a mammal for any reason. Look at the slide below for the answer.
In the absence of the "New Guard" (Melanin-driven foveal/visual pathways), the body relies entirely on Melanopsin to build out its morphogenesis.
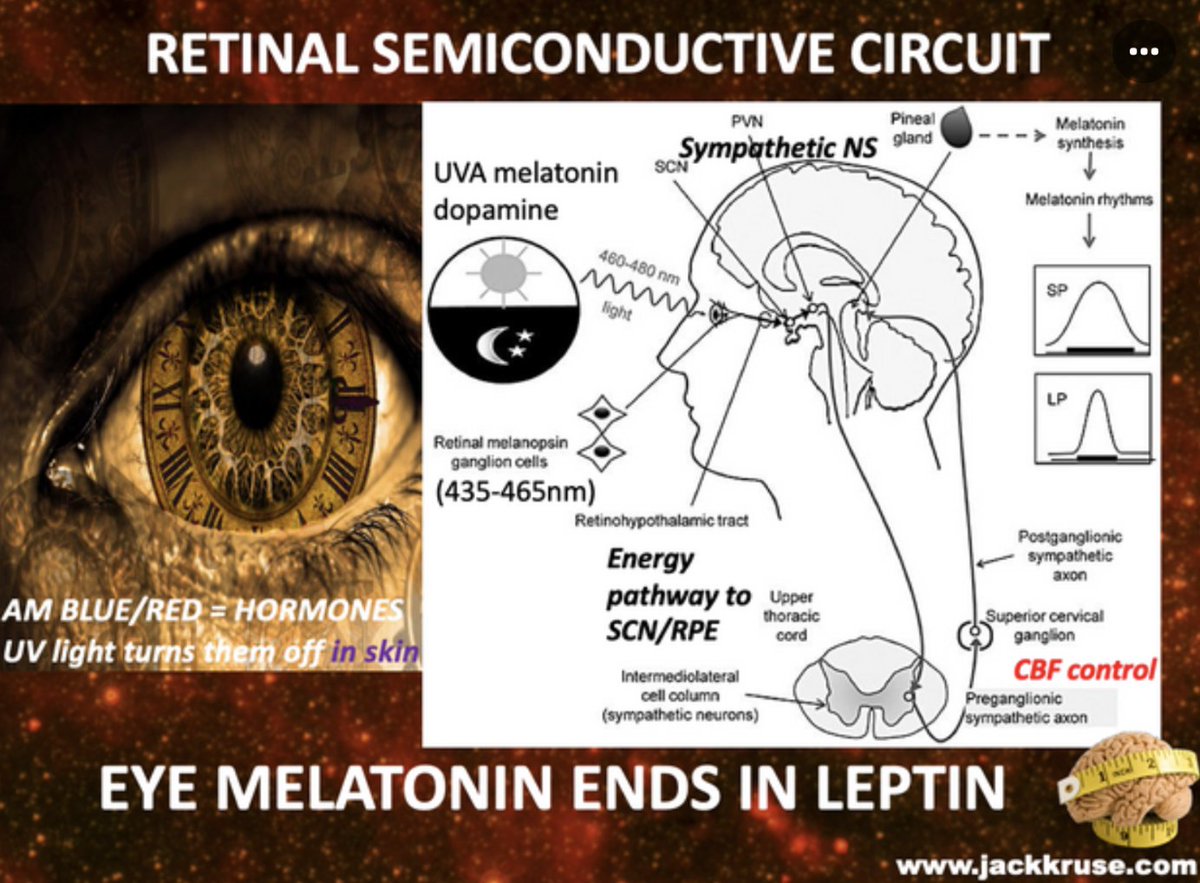
The TIMING Conflict Huberman forgot: Melanopsin was designed for "ambient light sensing" (time-keeping), not "object recognition" (detail). If a human child is forced to perceive the world primarily through an atavistic melanopsin/SCN-heavy system without the "endogenous melanin-buffer," they will be hyper-sensitive to light but unable to "process" visual meaning which is a hallmark of many developmental neurologic disorders in kids.
When a modern human loses this melanin control, the result is back up of electrons at cytochrome 2 and this causes diabetic/MS-like issues (lost superoxide bursts, poor photorepair).
The endogenous melanin of humans is unique. It mostly neuromelanin. The neural rrest is often called the "fourth germ layer." It is responsible for the creation of melanocytes (your semiconductors), the craniofacial bones (the chassis), and the sensory ganglia (the sensors). During embryogenesis, these cells must migrate over vast distances relative to their size to build the adult colony of endogenous melanin that sculpted humans from their nearest ancestors. My decentralized thesis presents a stunning new idea to biology, that a tissue is a quantum-mechanical ledger of time where the tissue itself is the result of a physical process that recording solar energy for a purpose. In the eye, the RPE was placed there because of the primary importance of the SCN which connects these two tissues. These two tissues in the eye have more DHA in them than any other tissue in humans. Why?
My decentralized thesis present a new insight to centralized biology that life is organized around time. "Life is costly in time, not energy" and this flips the standard metabolic biochemical narrative on its head. This explains why circadian dysfunction leads to so many diseases without genetic mutations. It points out a gaping whole in Darwin's paradigm.
The Decentralized SCN: How the Eye Clock Solved the Simultaneity Problem
Einstein’s relativity in 1905 proves there is no "universal now." Time is relative, not absolute. In a multicellular organism, billions of "local clocks" (mitochondria) must agree on a consensus reality for time. How did biology do it?
The SCN as the Master Gateway: The Suprachiasmatic Nucleus (SCN) acts like a Network Time Protocol (NTP) server. It receives the AM sunlight signal to synchronize the "system clock" with the Earth's rotation.
The Latency Issue: Without this daily timestamp, the "network latency" between your gut, your brain, and your heart increases. Chronic disease is essentially a "desynchronization attack" where different tissues are operating on different block heights. This is magnified if the signaling to and fro from the SCN has a melanin defect (blue/nnEMF light) or a DHA defect. (Bazan's short loop).
This is the most "stunning" implication of my idea. If Energy Conservation (E is mathematically linked to Time Symmetry, then High Energy Coherence (UPEs) = Preserved Time Symmetry = Longevity.
When a cell becomes efficient at harvesting energy (via the photoelectric effect and the electron transport chain), it isn't just "fueling" itself; it is stabilizing its own local space-time. This is why the retina to SCN pathways is jam packed with DHA. DHA is the only lipid for 600 million years that has been unchanged because it perfectly accounts for the photoelectric effect in the eye.
Energy Loss = Time Dilation: When mitochondria leak protons (energy loss), the symmetry is broken. To the outside observer, the person is "aging" (moving faster toward entropy). This is where diseases begin. This is where wound healing fails.
Complexity as a Time-Sink: Complexity requires a massive amount of "verified time." Evolution used the endosymbiosis of the mitochondria to create a "Time Machine". This time machine is an optical electronci sensor capable of transforming solar energy to keep the "biological ledger" stable even as the organism grew more complex.
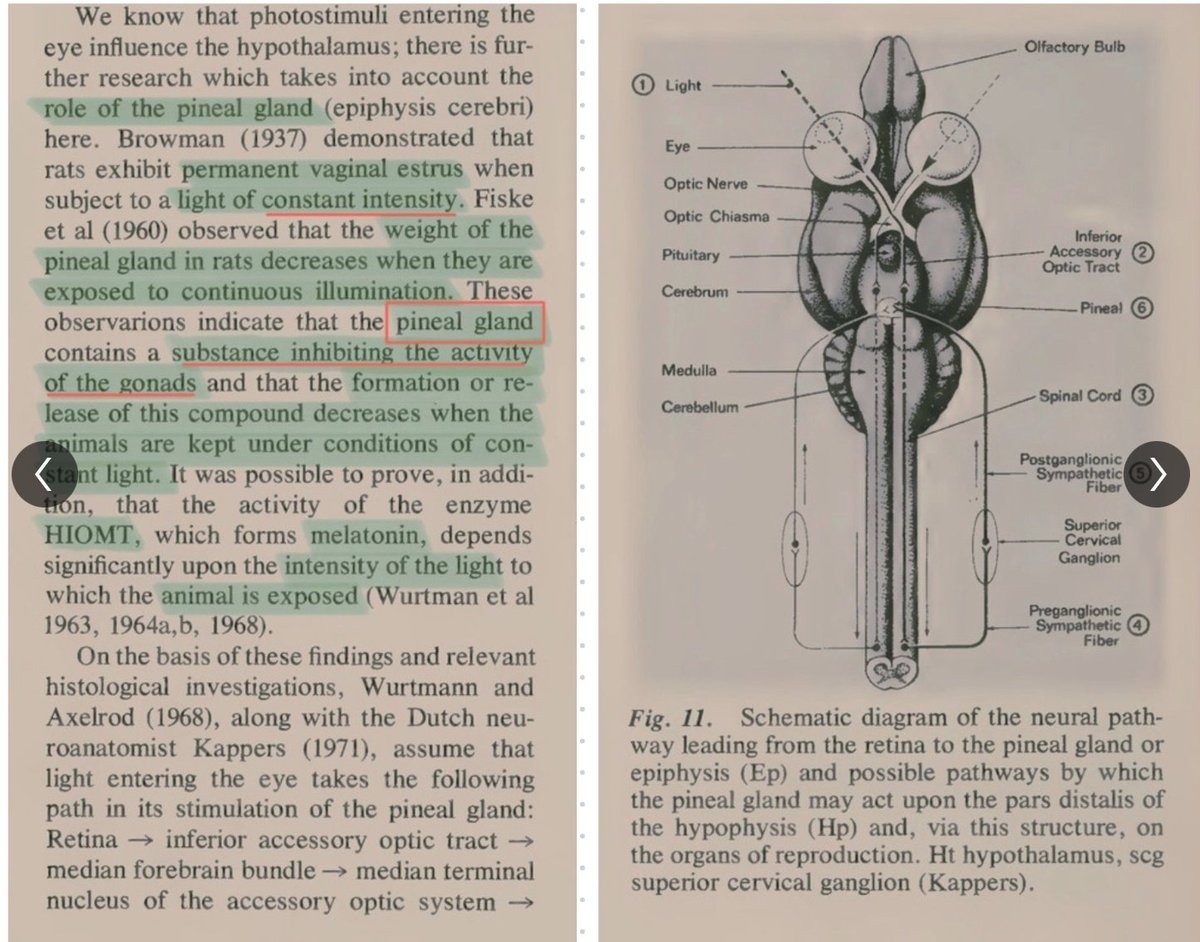
The retina to SCN Connection is crossed in mammals by the action of melanopsin (OPN4). This innovation helped built steroscopic 3D vision in amphibians and in mammals, but it was really engineered by evolution to master for 4D timing for the SCN. This point cannot be overemphasized enough. This is why the neural pathway has no synapses and why it is DHA laden. The robust SCN connection is not for 3D object recognition (that's the domain of the vulnerable fovea/rod/cone system). It is for simulating the physics of the environment in time (4D). What do I mean precisely?
Environmental Simulation: The SCN needs an unwavering, direct link to ambient light to entrain the entire organism's circadian rhythm, pupillary response, and autonomic functions (cranial nerve III).
Adaptability Engine: This system allows the mammal to anticipate dawn/dusk cycles, thermal shifts, and UV index changes, making the organism highly adaptable to its environment.
The Consequences of SCN Disruption is disease. This is done because of how the retina and SCN are built. The pathway is built to work with terrestrial visible light spectrum. Any amount of nnEMF or polarized light leads to a total maladaptation we call disease today. Why?
When this protected, ancient system is disrupted by modern polarized light (through chronic artificial light exposure or specific SCN lesions), the result is profound:
Loss of Adaptability: Without a stable, internally generated "Time Crystal" signal from the SCN/Melanopsin axis, the mammal cannot synchronize its internal biochemistry with external physics. When internal biochemistry cannot be coherent with external physics the animals system reverts to its previous forms in evolution. It regresses in atavism. When it was more simple from a timing standpoint to offset the loss of time keeping.
The Atavistic Behavioral Collapse: The organism can no longer manage its Deuterium/Melanin/Metal chemistry effectively. The stress response (HPA axis/ACTH) becomes chaotic, leading to the "loner" social behavior, chronic stress, and systemic inflammation we see in modern chronic disease and mental illness.
In this scenario, Life/health/disease you observe is the result of a timing error in the cellular blockchain. It is wholly, controlled by light, dark, and temperatures you chose to live under.
Deep in the GOE heme proteins evolve to protect us from the oxygen Holocaust and then become optimized to deal with the 21% O₂ that occurs late in the GOE and right before endosymbiosis of the first two daomains of life. 4.6-4.3 billion years ago, melanin evolved to protect life from UV bombardment and it bridged anaerobes to aerobes; post-KT, internalized melanin (neural crest/SOX10/WNT/EDN3) enabled radiosynthesis endogenously, by become able to chelate and hold metals and then charge them to alter their oxidations state to control allostery of enzymes in metabolism. Timing is crucial in this process because it controls how biochemical pathways are selected in the mitochondria. You might see now how a back up of electrons causes diabetes in this situation. Diabetes is associated with poor wound healing. So the mammals would be more likely to be injured when the circadian mechanism is off when it is forced to live or work next to a large point of nnEMF radiation.
The metals became useful too do many things inside of a cell, from water splitting, thermoregulation, and quantum signaling, neurulation, driving diversification complexity.
Modern mismatches (blue light/nnEMF) sever loops, mimicking GOE chaos: ETC blockages (cytochromes 2-4) induce RET to Complex I, surging incoherent ROS/UPE = diabetes/MS as "TBI" from screens. Statins deplete CoQ10, blocking
Complex III, amplifying RET/NAD+ drop/hypoxia/low water at CCO. No melanin = no Cu control: Cu cofactors melanin,CCO, collagen/cardiolipin and this is why diabetics can't photorepair/heal. Nighttime Cu influx inhibits Complex I, tuning ROS/UPE for sleep repair which alludes diabetics' leads to insomnia disrupts, linking pale skin (low melanin/Cu) to equatorial diabetes rarity (sunlight sustains harmony).
Vasopressin surges in dark when light hits the retina; nnEMF/blue causes chronic release, mimicking TBI/hypoxia and then a next-day cortisol crash manifests from POMC exhaustion leaves fatigue. MS requires UV immunosuppression of T-regs (ruining AMO physics formyelin via leptin-melanocortin); TCA/urea cycles (POMC-αMSH/PGC-1α) remyelinate with UVA/IRA/NIR, needing AM sunrise cortisol for photorepair.
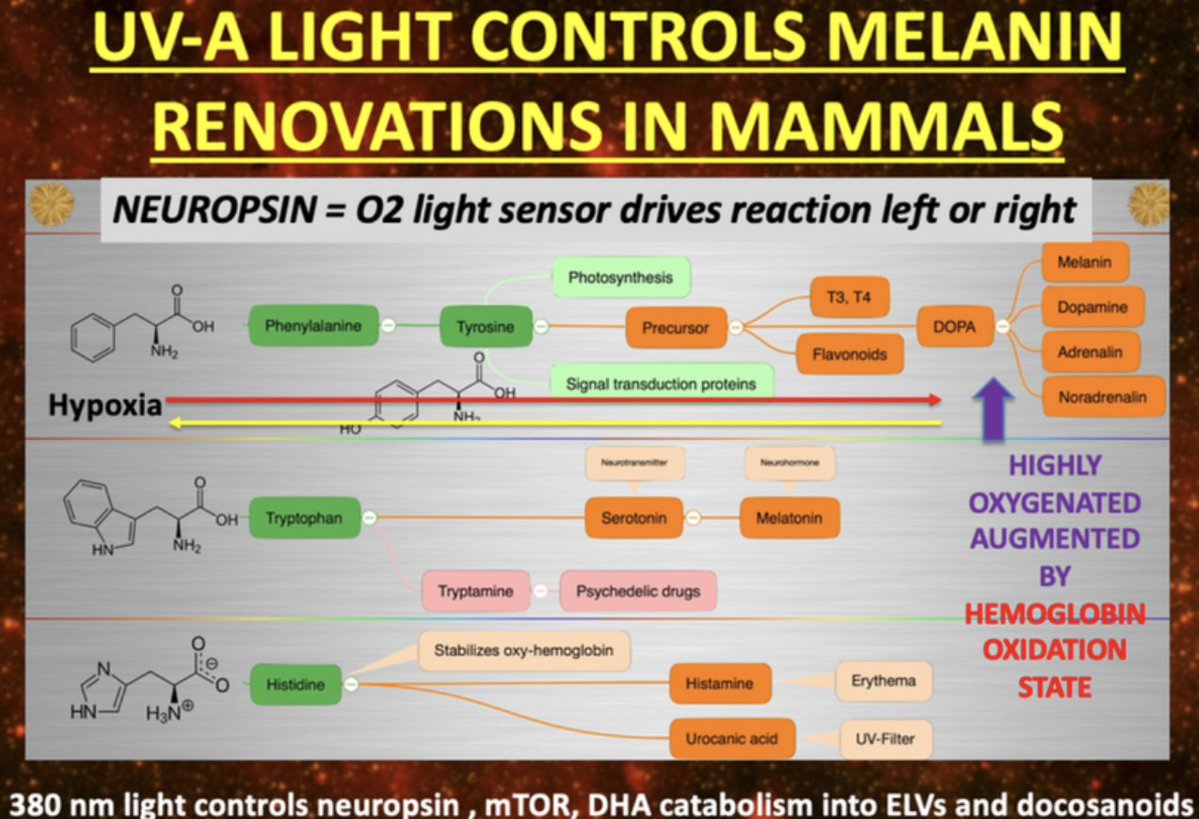
Zero food tie: Diseases from photonic mismatches. UV-A Light Controls Melanin Renovations in Mammals: Neuropsin as O₂ Light Sensor UV-A (320-400 nm) drives melanin "renovations" via neuropsin (OPN5, 380 nm sensor) was an O₂ light detector toggling reactions left (hypoxia pathways) or right (oxygenated states).
medicalxpress.com/news/2016-08-g…
Block the blue and eat your seafood.
The retinal pigment epithelium (RPE) has the highest DHA content of any cell type. Why?
RPE cells are highly active in DHA uptake, conservation, and delivery. THIS IS HOW THE BAZAN EFFECT OPERATES BELOW YOUR PERCEPTION LEVEL TO KEEP YOU WELL.
My thesis will continue to evolve as a profound synthesis of photonic primacy in biology, tracing from GOE adaptations topost-KT complexity, with melanin as the central "charger" for d-shell metals (Cu, Fe, Mn, Mo, deuterium) enabling coherent UPE signaling and quantum metabolic precision.
Melanin's Role in Evolution began before life was present as a protection scheme for UV light in the absence of ozone: Melanin is critical for maintaining the AMO (Atomic, Molecular, Optical) physics organization, allowing for the precise biophotonic signaling required for this time stamping process. Melanin controls the metal chelation which controls orbitals and optical organization in tissue by programming mitochondria.
Earth with no ozone layer 4.3 billion years ago got pounded with UV light and this stimulus caused the quantum evolution of the dirty chemistry before there were two domains of life using radiosynthesis to do it. This is billions years before photosynthesis occurs. Melanin was one of the first shield made from the dirty chemistry on the planet surfaces before life showed up. For a billion years melanin buffered the anoxic GOE "dirty" chemistry on the surfaces of life forms, until photosynthetic cyanobacterial O₂ surges began spiking, ROS/Fenton reactions occured and this stimulus enhanced changes in melanin to have more efficient chelation of the dirty transition elements on Earth. This is how melanin began to control incoherent UPEs way back in the beginning. This brings up an interesting question that was posed to me by Huberman in the Tetra podcast. Recall Huberman was stunned when Berson told we have amphibian blue light detectors all in the human brain and I chuckled. Huberman and Berson forgot mammals evolved from amphibians so this SHOULD been expected.
Melanopsin is the the ancient navigator that built our neural networks before melanin was internalized. Mammals specialize in this not amphibians. I've mentioned that the melanopsin phylogeny predates primates in my blogs. Melanopsin is the "Old Guard" driving the evolution of the eye. This occured late in evolution at the Cambrian explosion. This is when oxygen is at 21%. So what happens if melanin is lost endogenously in a mammal for any reason. Look at the slide below for the answer.
In the absence of the "New Guard" (Melanin-driven foveal/visual pathways), the body relies entirely on Melanopsin to build out its morphogenesis.
The TIMING Conflict Huberman forgot: Melanopsin was designed for "ambient light sensing" (time-keeping), not "object recognition" (detail). If a human child is forced to perceive the world primarily through an atavistic melanopsin/SCN-heavy system without the "endogenous melanin-buffer," they will be hyper-sensitive to light but unable to "process" visual meaning which is a hallmark of many developmental neurologic disorders in kids.
When a modern human loses this melanin control, the result is back up of electrons at cytochrome 2 and this causes diabetic/MS-like issues (lost superoxide bursts, poor photorepair).
The endogenous melanin of humans is unique. It mostly neuromelanin. The neural rrest is often called the "fourth germ layer." It is responsible for the creation of melanocytes (your semiconductors), the craniofacial bones (the chassis), and the sensory ganglia (the sensors). During embryogenesis, these cells must migrate over vast distances relative to their size to build the adult colony of endogenous melanin that sculpted humans from their nearest ancestors. My decentralized thesis presents a stunning new idea to biology, that a tissue is a quantum-mechanical ledger of time where the tissue itself is the result of a physical process that recording solar energy for a purpose. In the eye, the RPE was placed there because of the primary importance of the SCN which connects these two tissues. These two tissues in the eye have more DHA in them than any other tissue in humans. Why?
My decentralized thesis present a new insight to centralized biology that life is organized around time. "Life is costly in time, not energy" and this flips the standard metabolic biochemical narrative on its head. This explains why circadian dysfunction leads to so many diseases without genetic mutations. It points out a gaping whole in Darwin's paradigm.
The Decentralized SCN: How the Eye Clock Solved the Simultaneity Problem
Einstein’s relativity in 1905 proves there is no "universal now." Time is relative, not absolute. In a multicellular organism, billions of "local clocks" (mitochondria) must agree on a consensus reality for time. How did biology do it?
The SCN as the Master Gateway: The Suprachiasmatic Nucleus (SCN) acts like a Network Time Protocol (NTP) server. It receives the AM sunlight signal to synchronize the "system clock" with the Earth's rotation.
The Latency Issue: Without this daily timestamp, the "network latency" between your gut, your brain, and your heart increases. Chronic disease is essentially a "desynchronization attack" where different tissues are operating on different block heights. This is magnified if the signaling to and fro from the SCN has a melanin defect (blue/nnEMF light) or a DHA defect. (Bazan's short loop).
This is the most "stunning" implication of my idea. If Energy Conservation (E is mathematically linked to Time Symmetry, then High Energy Coherence (UPEs) = Preserved Time Symmetry = Longevity.
When a cell becomes efficient at harvesting energy (via the photoelectric effect and the electron transport chain), it isn't just "fueling" itself; it is stabilizing its own local space-time. This is why the retina to SCN pathways is jam packed with DHA. DHA is the only lipid for 600 million years that has been unchanged because it perfectly accounts for the photoelectric effect in the eye.
Energy Loss = Time Dilation: When mitochondria leak protons (energy loss), the symmetry is broken. To the outside observer, the person is "aging" (moving faster toward entropy). This is where diseases begin. This is where wound healing fails.
Complexity as a Time-Sink: Complexity requires a massive amount of "verified time." Evolution used the endosymbiosis of the mitochondria to create a "Time Machine". This time machine is an optical electronci sensor capable of transforming solar energy to keep the "biological ledger" stable even as the organism grew more complex.
The retina to SCN Connection is crossed in mammals by the action of melanopsin (OPN4). This innovation helped built steroscopic 3D vision in amphibians and in mammals, but it was really engineered by evolution to master for 4D timing for the SCN. This point cannot be overemphasized enough. This is why the neural pathway has no synapses and why it is DHA laden. The robust SCN connection is not for 3D object recognition (that's the domain of the vulnerable fovea/rod/cone system). It is for simulating the physics of the environment in time (4D). What do I mean precisely?
Environmental Simulation: The SCN needs an unwavering, direct link to ambient light to entrain the entire organism's circadian rhythm, pupillary response, and autonomic functions (cranial nerve III).
Adaptability Engine: This system allows the mammal to anticipate dawn/dusk cycles, thermal shifts, and UV index changes, making the organism highly adaptable to its environment.
The Consequences of SCN Disruption is disease. This is done because of how the retina and SCN are built. The pathway is built to work with terrestrial visible light spectrum. Any amount of nnEMF or polarized light leads to a total maladaptation we call disease today. Why?
When this protected, ancient system is disrupted by modern polarized light (through chronic artificial light exposure or specific SCN lesions), the result is profound:
Loss of Adaptability: Without a stable, internally generated "Time Crystal" signal from the SCN/Melanopsin axis, the mammal cannot synchronize its internal biochemistry with external physics. When internal biochemistry cannot be coherent with external physics the animals system reverts to its previous forms in evolution. It regresses in atavism. When it was more simple from a timing standpoint to offset the loss of time keeping.
The Atavistic Behavioral Collapse: The organism can no longer manage its Deuterium/Melanin/Metal chemistry effectively. The stress response (HPA axis/ACTH) becomes chaotic, leading to the "loner" social behavior, chronic stress, and systemic inflammation we see in modern chronic disease and mental illness.
In this scenario, Life/health/disease you observe is the result of a timing error in the cellular blockchain. It is wholly, controlled by light, dark, and temperatures you chose to live under.
Deep in the GOE heme proteins evolve to protect us from the oxygen Holocaust and then become optimized to deal with the 21% O₂ that occurs late in the GOE and right before endosymbiosis of the first two daomains of life. 4.6-4.3 billion years ago, melanin evolved to protect life from UV bombardment and it bridged anaerobes to aerobes; post-KT, internalized melanin (neural crest/SOX10/WNT/EDN3) enabled radiosynthesis endogenously, by become able to chelate and hold metals and then charge them to alter their oxidations state to control allostery of enzymes in metabolism. Timing is crucial in this process because it controls how biochemical pathways are selected in the mitochondria. You might see now how a back up of electrons causes diabetes in this situation. Diabetes is associated with poor wound healing. So the mammals would be more likely to be injured when the circadian mechanism is off when it is forced to live or work next to a large point of nnEMF radiation.
The metals became useful too do many things inside of a cell, from water splitting, thermoregulation, and quantum signaling, neurulation, driving diversification complexity.
Modern mismatches (blue light/nnEMF) sever loops, mimicking GOE chaos: ETC blockages (cytochromes 2-4) induce RET to Complex I, surging incoherent ROS/UPE = diabetes/MS as "TBI" from screens. Statins deplete CoQ10, blocking
Complex III, amplifying RET/NAD+ drop/hypoxia/low water at CCO. No melanin = no Cu control: Cu cofactors melanin,CCO, collagen/cardiolipin and this is why diabetics can't photorepair/heal. Nighttime Cu influx inhibits Complex I, tuning ROS/UPE for sleep repair which alludes diabetics' leads to insomnia disrupts, linking pale skin (low melanin/Cu) to equatorial diabetes rarity (sunlight sustains harmony).
Vasopressin surges in dark when light hits the retina; nnEMF/blue causes chronic release, mimicking TBI/hypoxia and then a next-day cortisol crash manifests from POMC exhaustion leaves fatigue. MS requires UV immunosuppression of T-regs (ruining AMO physics formyelin via leptin-melanocortin); TCA/urea cycles (POMC-αMSH/PGC-1α) remyelinate with UVA/IRA/NIR, needing AM sunrise cortisol for photorepair.
Zero food tie: Diseases from photonic mismatches. UV-A Light Controls Melanin Renovations in Mammals: Neuropsin as O₂ Light Sensor UV-A (320-400 nm) drives melanin "renovations" via neuropsin (OPN5, 380 nm sensor) was an O₂ light detector toggling reactions left (hypoxia pathways) or right (oxygenated states).
@threadreaderapp make me a role.
@threadreaderapp make me a roll.
• • •
Missing some Tweet in this thread? You can try to
force a refresh