💥💥💥BOOM💥💥💥
Recently released Australian Road Deaths data confirm that the @epiphare study claiming that COVID vaccination reduced road deaths by 32% was, as suspected, a complete fake.
See next tweet for the analysis and sources.
Paper: jamanetwork.com/journals/jaman… x.com/sudokuvariante…
Recently released Australian Road Deaths data confirm that the @epiphare study claiming that COVID vaccination reduced road deaths by 32% was, as suspected, a complete fake.
See next tweet for the analysis and sources.
Paper: jamanetwork.com/journals/jaman… x.com/sudokuvariante…
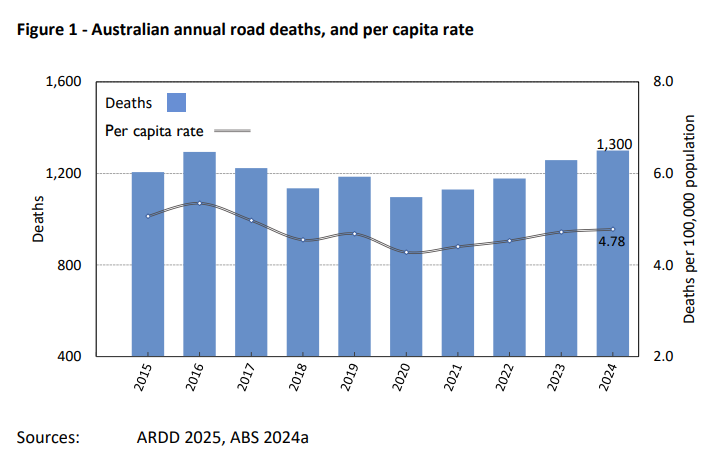
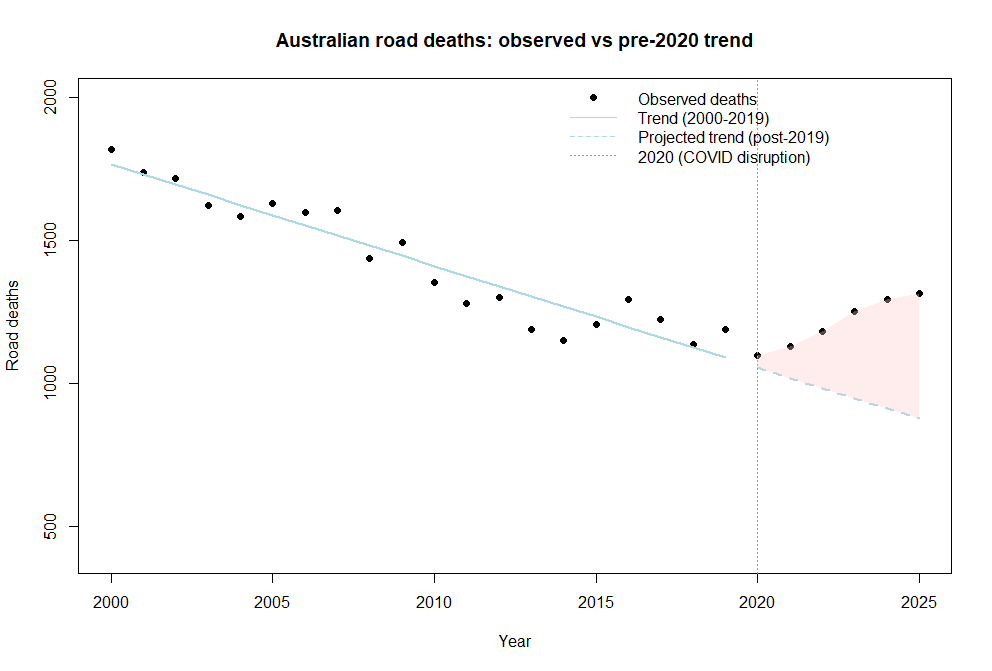
Here are the actual road deaths data plotted from the Australian BITRE data repository using a trendline for 2000-2019 (excluding 2020 as it was a quiet year)
The pink area shows the inflection and increase in road deaths over the predicted number.
Note that road deaths have a downward trend despite an increase in population (due to safety measures and slowing of traffic).
The pink area shows the inflection and increase in road deaths over the predicted number.
Note that road deaths have a downward trend despite an increase in population (due to safety measures and slowing of traffic).
So the question becomes...
"what is the probability that - if the @epiphare study was real (showing a 32% reduction in road deaths after vaccination) - the Australian road deaths (where nearly 100% of the adult population was vaccinated) would increase by 36%"?
"what is the probability that - if the @epiphare study was real (showing a 32% reduction in road deaths after vaccination) - the Australian road deaths (where nearly 100% of the adult population was vaccinated) would increase by 36%"?
Well if you're a Bayesian mathematician like @profnfenton you can do that by Bayes but..
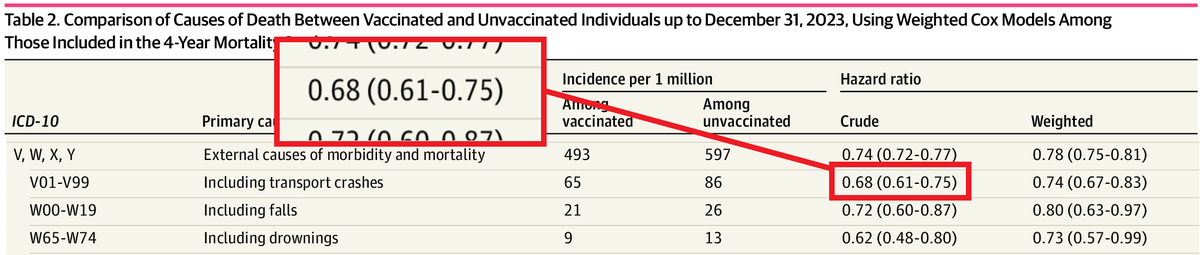
For the rest of us we can use the provided 95% confidence interval from @epiphare which is here in table 2:
[0.68 (0.61-0.75)]
to estimate the probability that there was an increase...
For the rest of us we can use the provided 95% confidence interval from @epiphare which is here in table 2:
[0.68 (0.61-0.75)]
to estimate the probability that there was an increase...
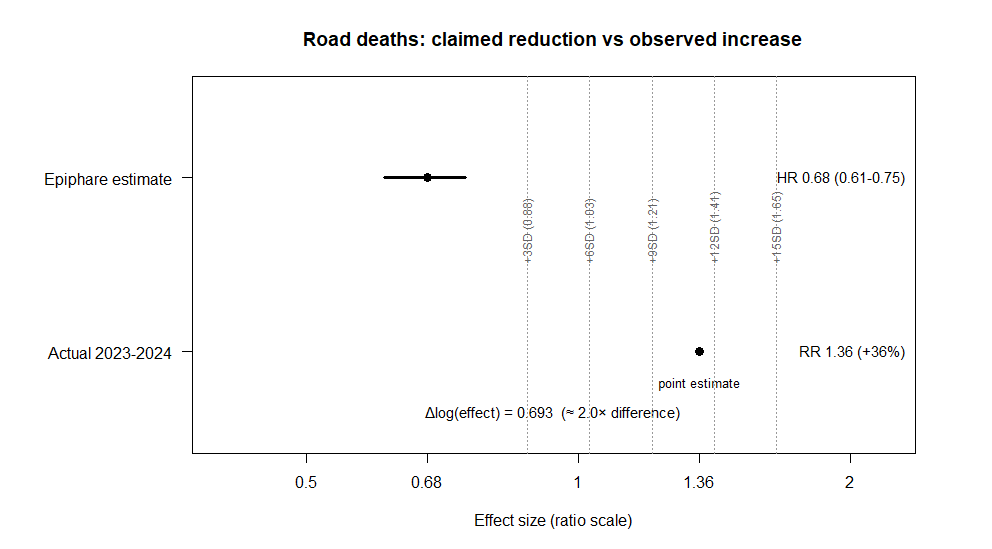
By working out how many standard deviations from that Epiphare estimate the real Australian data (+36% increase, based on 2023-2024 data) is... And then calculating the probability of that point estimator.
And here you are
And here you are
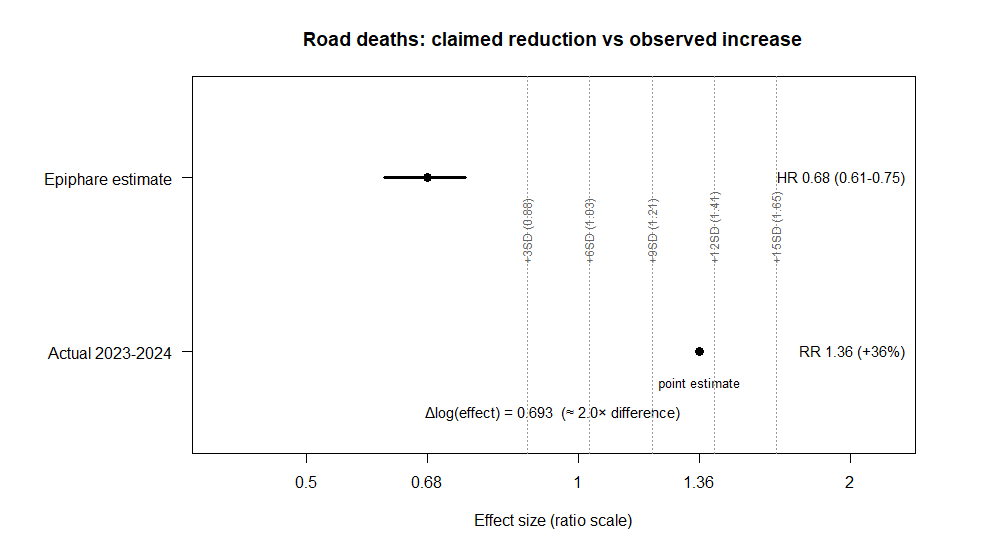
What this shows is that the Aus real-life value is is over 10 sigma outside Epiphare's own upper estimate of the miraculous "risk reduction for car crashes"
This is impossible. That is, there are so many zeroes on this probability it cannot exist.
(p<0.0000000000000000001)
This is impossible. That is, there are so many zeroes on this probability it cannot exist.
(p<0.0000000000000000001)
So, either @Epiphare fabricated a paper (by producing biased data that they didn't check) to support a claim that was never rational..
Or the Australian BITRE bureau did.
I know who my money is on.
jamanetwork.com/journals/jaman…
Or the Australian BITRE bureau did.
I know who my money is on.
jamanetwork.com/journals/jaman…
Sources:
R-code
itty.bitty.site/R--code-for-Bi…
BITRE report
bitre.gov.au/sites/default/…
BITRE data repository
bitre.gov.au/statistics/saf…
Limitations:
The data are not adjusted for population as this is likely to overestimate the discordance and the road death numbers have their own built-in confounder that is not independent of the population. Furthermore, the vaccination rate of the population is unknown but claimed to be over 95% of adults. It is assumed that the population is 100% vaccinated for this exercise as it would be illogical to expect the increase in road deaths to be wholly attributed to the small number of unvaccinated adults (<2%) in the population given the Epiphare estimator.
Different trend lines can be curated giving a different value of the estimator but the magnitude of the discordance is still huge.
@MaryanneDemasi @DrJulieSladden @Fynnderella1 @sudokuvariante @DrJBhattacharya @Kevin_McKernan @canceledmouse @jsm2334 @franklin_reeder @boriquagato @AGHuff @Johnincarlisle @TonyNikolic10
R-code
itty.bitty.site/R--code-for-Bi…
BITRE report
bitre.gov.au/sites/default/…
BITRE data repository
bitre.gov.au/statistics/saf…
Limitations:
The data are not adjusted for population as this is likely to overestimate the discordance and the road death numbers have their own built-in confounder that is not independent of the population. Furthermore, the vaccination rate of the population is unknown but claimed to be over 95% of adults. It is assumed that the population is 100% vaccinated for this exercise as it would be illogical to expect the increase in road deaths to be wholly attributed to the small number of unvaccinated adults (<2%) in the population given the Epiphare estimator.
Different trend lines can be curated giving a different value of the estimator but the magnitude of the discordance is still huge.
@MaryanneDemasi @DrJulieSladden @Fynnderella1 @sudokuvariante @DrJBhattacharya @Kevin_McKernan @canceledmouse @jsm2334 @franklin_reeder @boriquagato @AGHuff @Johnincarlisle @TonyNikolic10
• • •
Missing some Tweet in this thread? You can try to
force a refresh