THE NANOPARTICLE REVOLUTION: Re-educating the Blood-Brain Barrier.
New research from a Spanish and Chinese consortium has unveiled a "supramolecular drug" capable of repairing the BBB's natural waste-disposal system to treat Alzheimer’s.
A thread on the future of AD therapy.
New research from a Spanish and Chinese consortium has unveiled a "supramolecular drug" capable of repairing the BBB's natural waste-disposal system to treat Alzheimer’s.
A thread on the future of AD therapy.
1/ The Problem: In Alzheimer’s, the Blood-Brain Barrier (BBB) stops working as a filter and starts acting as a wall.
Toxic proteins like Aβ build up because the brain's natural "trash shoot" is broken.
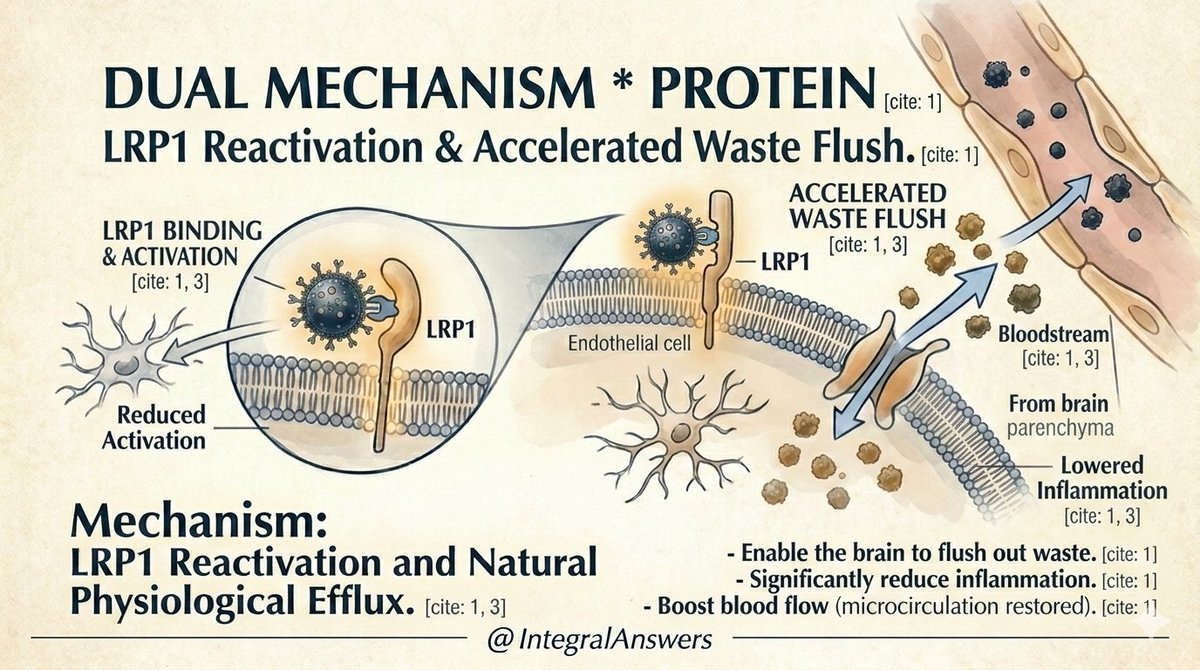
The Solution: Activating the endogenous efflux pump.
Toxic proteins like Aβ build up because the brain's natural "trash shoot" is broken.
The Solution: Activating the endogenous efflux pump.
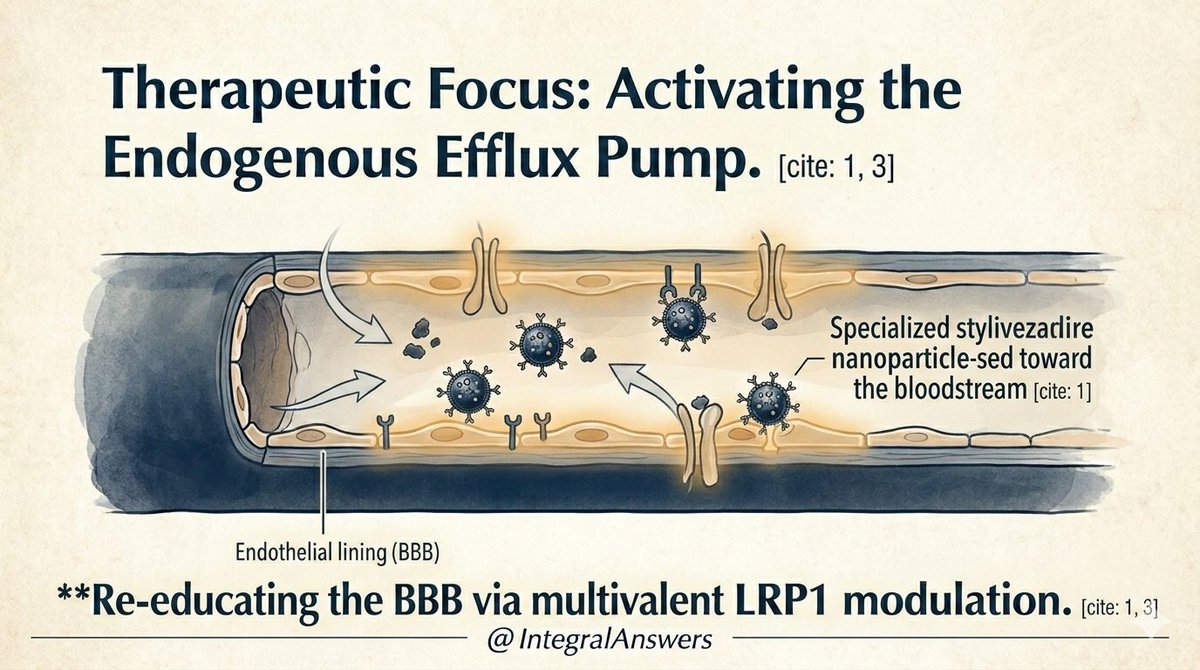
2/ This breakthrough is a global effort. By combining material synthesis expertise from China with biological validation from Spain, researchers created a nanoparticle that doesn't just deliver drugs—it heals the barrier itself.

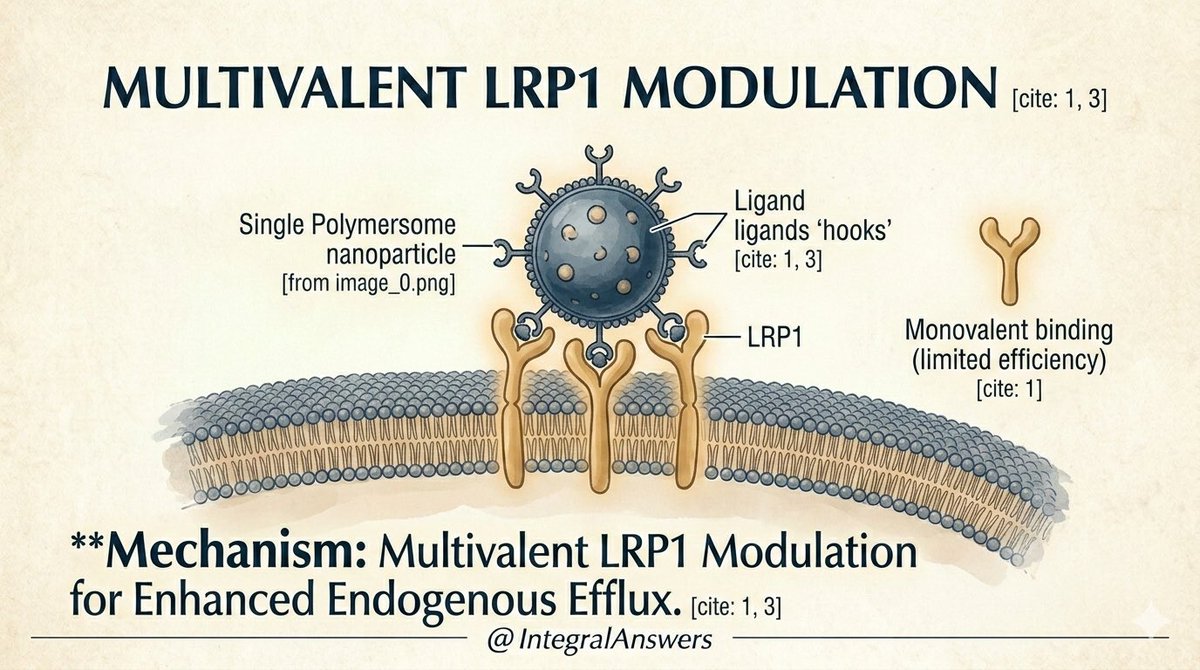
3/ The Secret Sauce: Multivalency.
Traditional drugs often use a "single-key" approach. These new polymersomes use multiple "hooks" to bind to LRP1 receptors simultaneously. This multivalent binding creates a much stronger and faster response.
Traditional drugs often use a "single-key" approach. These new polymersomes use multiple "hooks" to bind to LRP1 receptors simultaneously. This multivalent binding creates a much stronger and faster response.
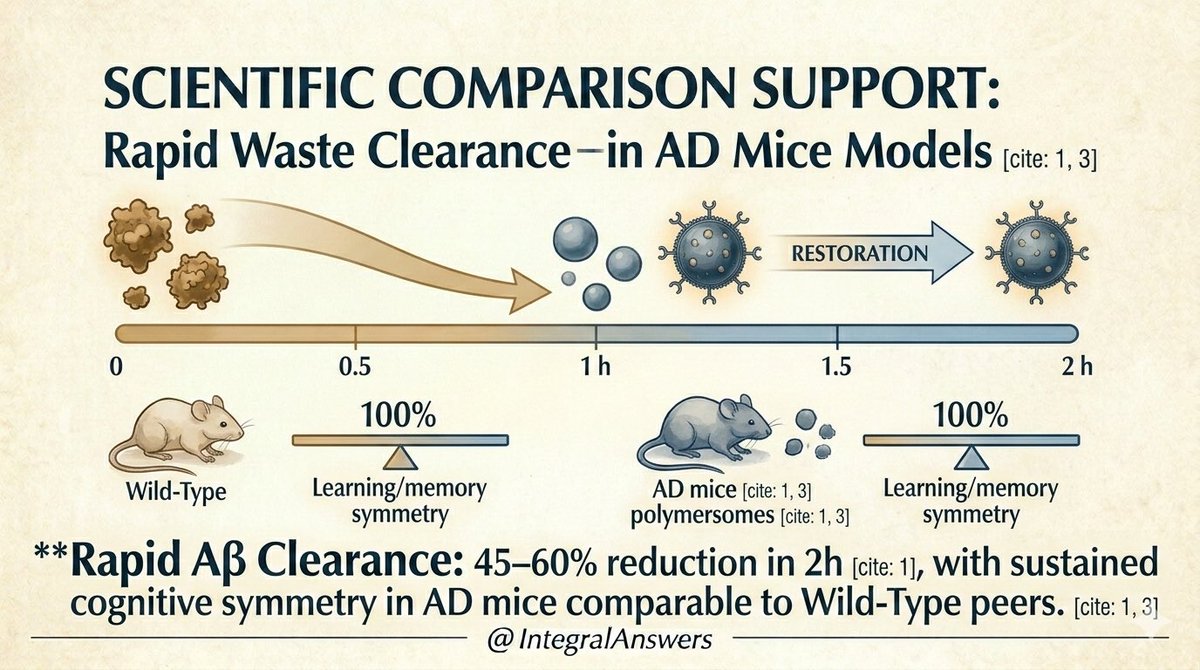
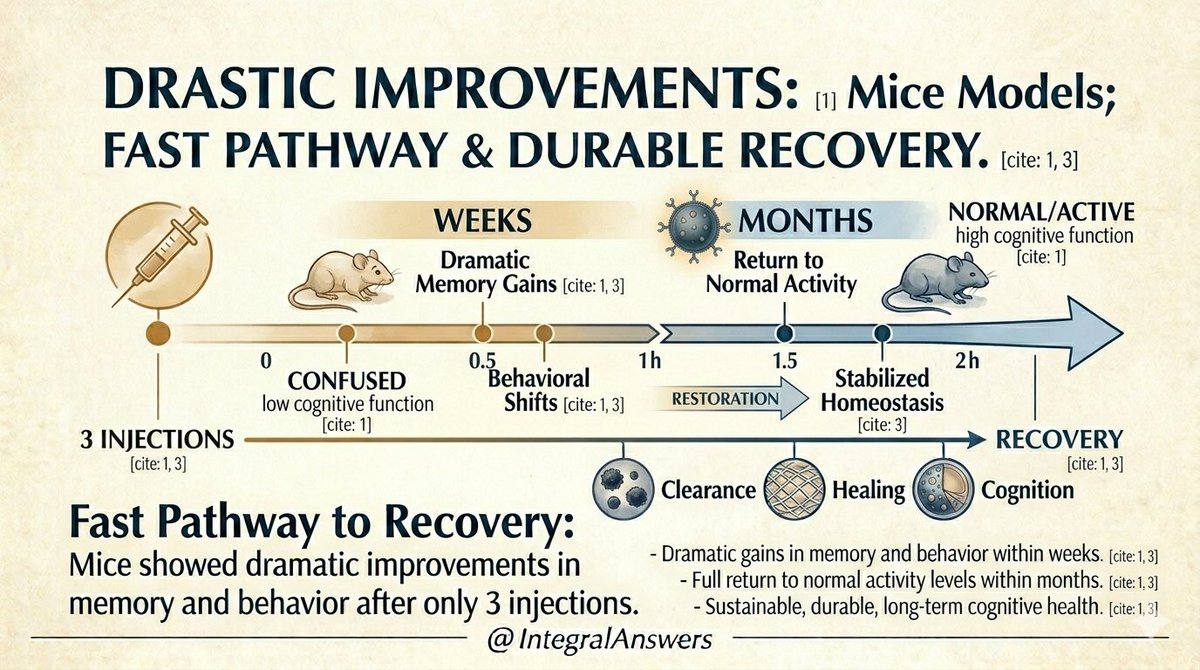
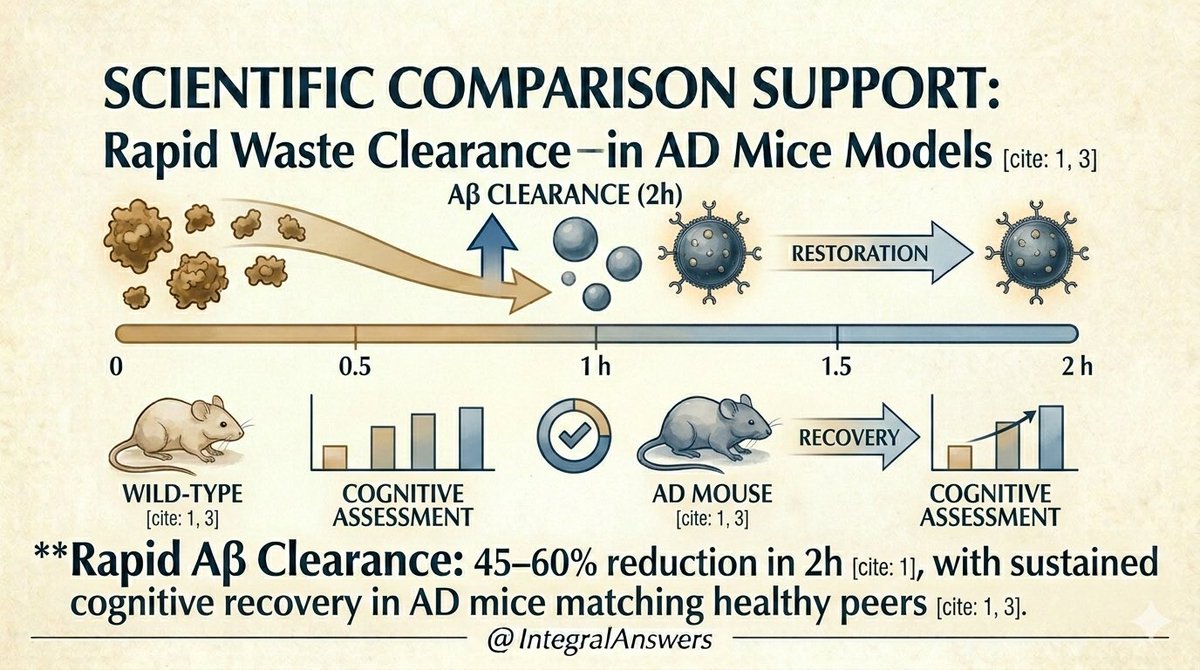
4/ The Results: Speed.
In AD mice models, this method achieved a 45–60% reduction in brain Aβ levels within just 2 hours of administration. This is an unprecedented rate of clearance compared to existing experimental therapies.
In AD mice models, this method achieved a 45–60% reduction in brain Aβ levels within just 2 hours of administration. This is an unprecedented rate of clearance compared to existing experimental therapies.
5/ Dual Mechanism.
The polymersomes don't just clear plaque; they restore the physiological health of the endothelial cells. This reactivates the natural "flushing" mechanism, allowing the brain to maintain its own cleanliness.
The polymersomes don't just clear plaque; they restore the physiological health of the endothelial cells. This reactivates the natural "flushing" mechanism, allowing the brain to maintain its own cleanliness.
6/ Long-term Impact.
It’s not just a temporary fix. In studies, just 3 injections led to sustained cognitive recovery and behavioral symmetry with healthy peers that lasted for up to 6 months.
It’s not just a temporary fix. In studies, just 3 injections led to sustained cognitive recovery and behavioral symmetry with healthy peers that lasted for up to 6 months.
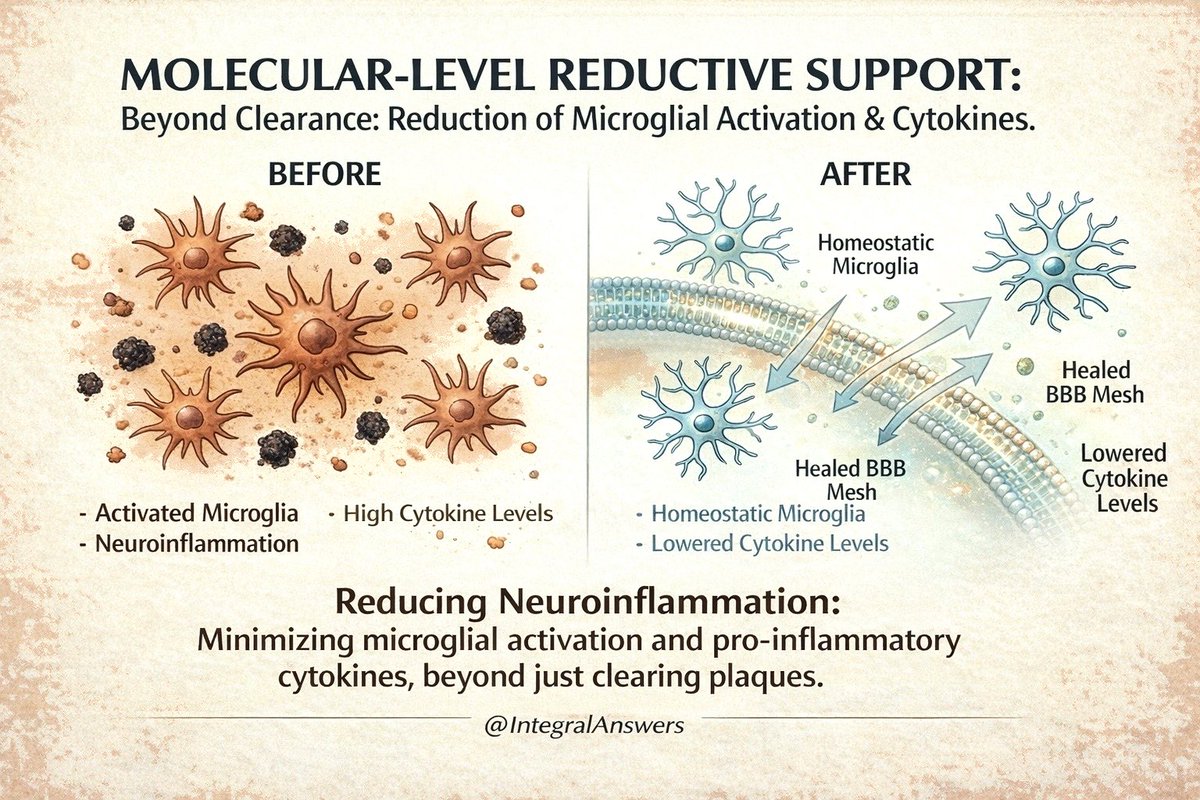
7/ Beyond the Plaque.
By repairing the BBB and clearing waste, the treatment significantly reduces microglial activation and pro-inflammatory cytokines. It heals the environment, it doesn't just scrub the surface.
By repairing the BBB and clearing waste, the treatment significantly reduces microglial activation and pro-inflammatory cytokines. It heals the environment, it doesn't just scrub the surface.
8/ A Paradigm Shift.
Current mAbs (like lecanemab) focus on dissolving plaques directly, which can cause vascular stress (ARIA).
Polymersomes focus on "barrier healing"—using the body’s own exit ramps to remove waste safely.
Current mAbs (like lecanemab) focus on dissolving plaques directly, which can cause vascular stress (ARIA).
Polymersomes focus on "barrier healing"—using the body’s own exit ramps to remove waste safely.
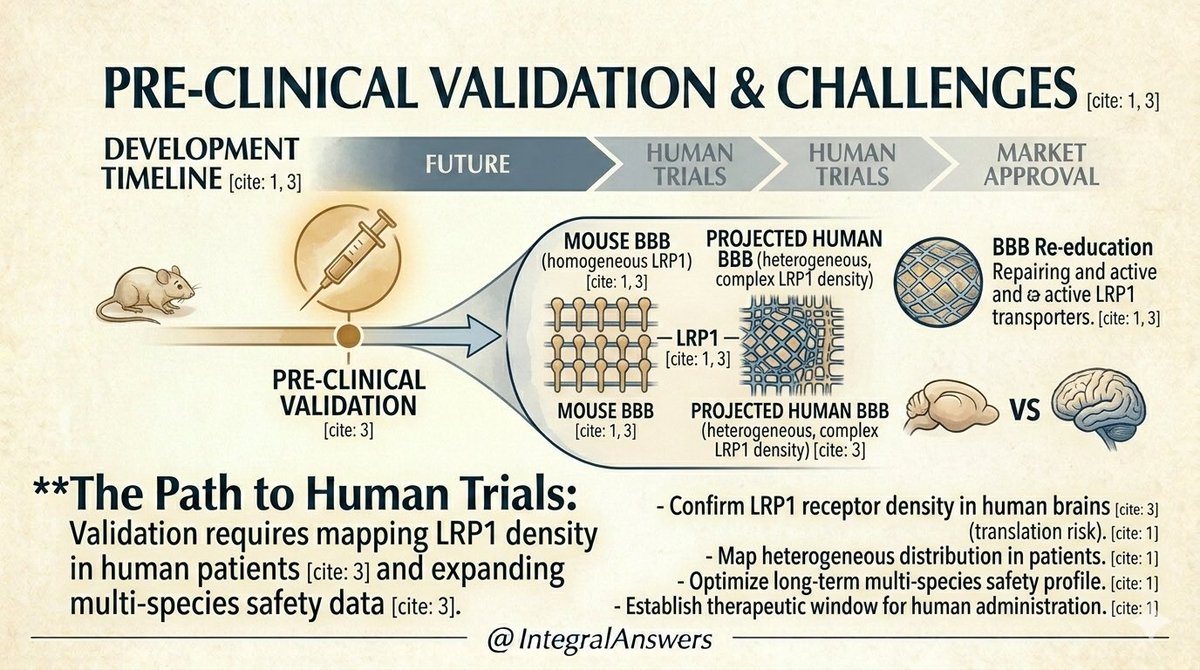
9/ The Hurdles.
While the mouse data is revolutionary, human brains are more complex. We must now map LRP1 receptor density in human patients to ensure the "translational mapping" is accurate for clinical use.
While the mouse data is revolutionary, human brains are more complex. We must now map LRP1 receptor density in human patients to ensure the "translational mapping" is accurate for clinical use.
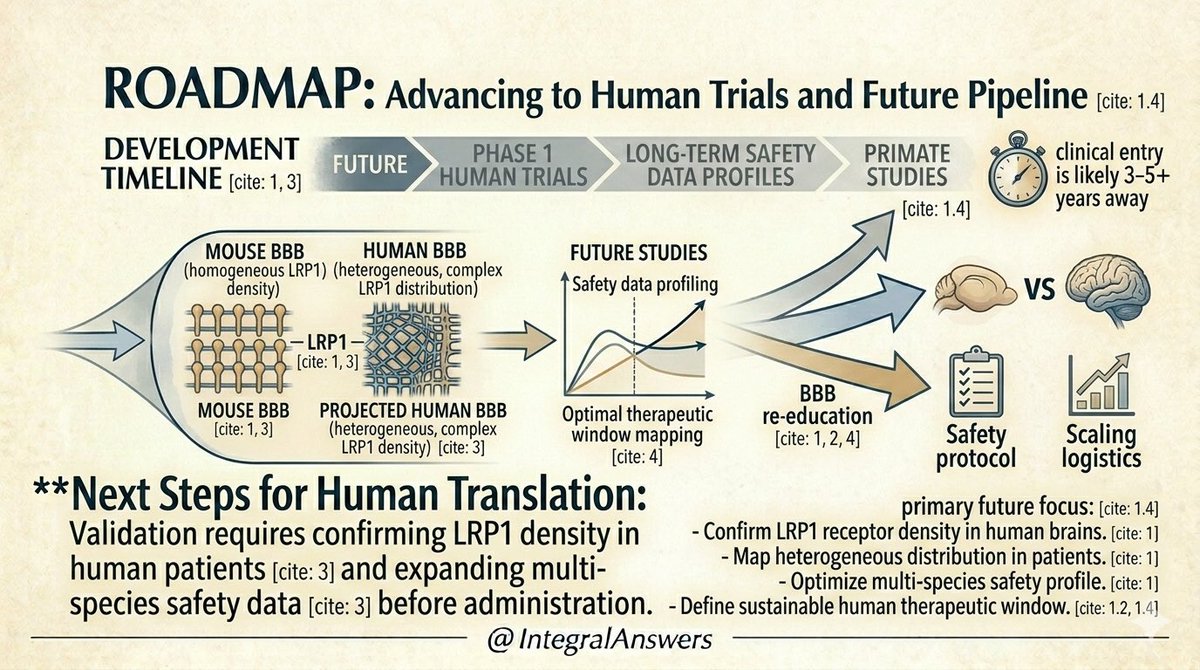
10/ The Timeline.
What’s next? Primate studies and long-term safety profiling. While we are likely 3–5+ years away from human Phase 1 trials, the roadmap for "re-educating" the BBB is now officially open.
What’s next? Primate studies and long-term safety profiling. While we are likely 3–5+ years away from human Phase 1 trials, the roadmap for "re-educating" the BBB is now officially open.
11/ The Foundation.
All data presented is grounded in the latest research. Precision matters.
Citations:
* Xiang et al. (2025). Nature Nanotech.
* Ruiz-Perez et al. (2025).
* Mazin (2025).
* Frontiers (2025).
All data presented is grounded in the latest research. Precision matters.
Citations:
* Xiang et al. (2025). Nature Nanotech.
* Ruiz-Perez et al. (2025).
* Mazin (2025).
* Frontiers (2025).
• • •
Missing some Tweet in this thread? You can try to
force a refresh