Science & medicine communicator. Exposing the misinformation that harms health—and the evidence that protects it.
 2/ The story is largely recycled from journalist Dan Olmsted’s 2005 “Amish anomaly” columns.
2/ The story is largely recycled from journalist Dan Olmsted’s 2005 “Amish anomaly” columns.
 2/4 Why were children who died after day 120 classified as “alive”? Why was a child called “unvaccinated” merely because no listed dose appeared during days 60–90? And why were roughly 69% of death records left unlinked without showing whether linkage biased the sample?
2/4 Why were children who died after day 120 classified as “alive”? Why was a child called “unvaccinated” merely because no listed dose appeared during days 60–90? And why were roughly 69% of death records left unlinked without showing whether linkage biased the sample?
 2/ Definitions Matter
2/ Definitions Matter
 1/ A new Nature paper asks a deceptively simple question:
1/ A new Nature paper asks a deceptively simple question:
 2/ The key distinction:
2/ The key distinction:
 2/ Robert F. Kennedy Jr.
2/ Robert F. Kennedy Jr.
 2/ Why do scientists do this kind of research at all? In principle, because studying how pathogens change can help us understand what mutations matter, how viruses adapt, what might threaten humans, and how to design surveillance, vaccines, and treatments. The problem is that this is classic “dual-use” territory: work done for legitimate public-health reasons can also create safety or security risks if the organism, methods, or knowledge are misused or escape containment.
2/ Why do scientists do this kind of research at all? In principle, because studying how pathogens change can help us understand what mutations matter, how viruses adapt, what might threaten humans, and how to design surveillance, vaccines, and treatments. The problem is that this is classic “dual-use” territory: work done for legitimate public-health reasons can also create safety or security risks if the organism, methods, or knowledge are misused or escape containment.
 2/ Start with “like cures like.”
2/ Start with “like cures like.”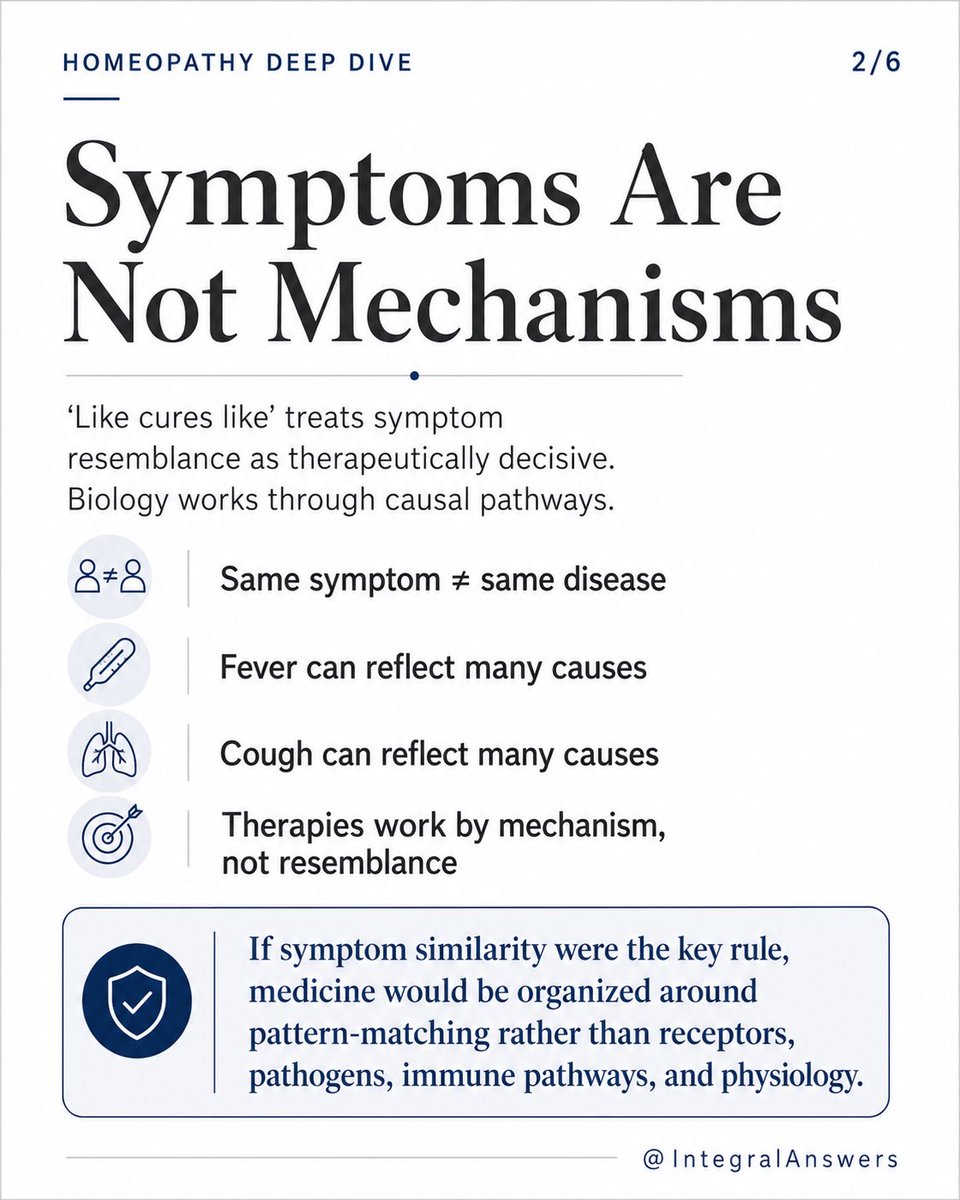
 1/ The CHD essay on retracted homeopathy studies raises one legitimate issue: retractions should be transparent, proportionate, and procedurally fair.
1/ The CHD essay on retracted homeopathy studies raises one legitimate issue: retractions should be transparent, proportionate, and procedurally fair.
 1/ Some antivaccine accounts are now arguing:
1/ Some antivaccine accounts are now arguing:
 2/ What did the Norwegian study actually find?
2/ What did the Norwegian study actually find?
 2/ The story begins in Greenland.
2/ The story begins in Greenland.
 1/ Cortisol’s Original Job
1/ Cortisol’s Original Job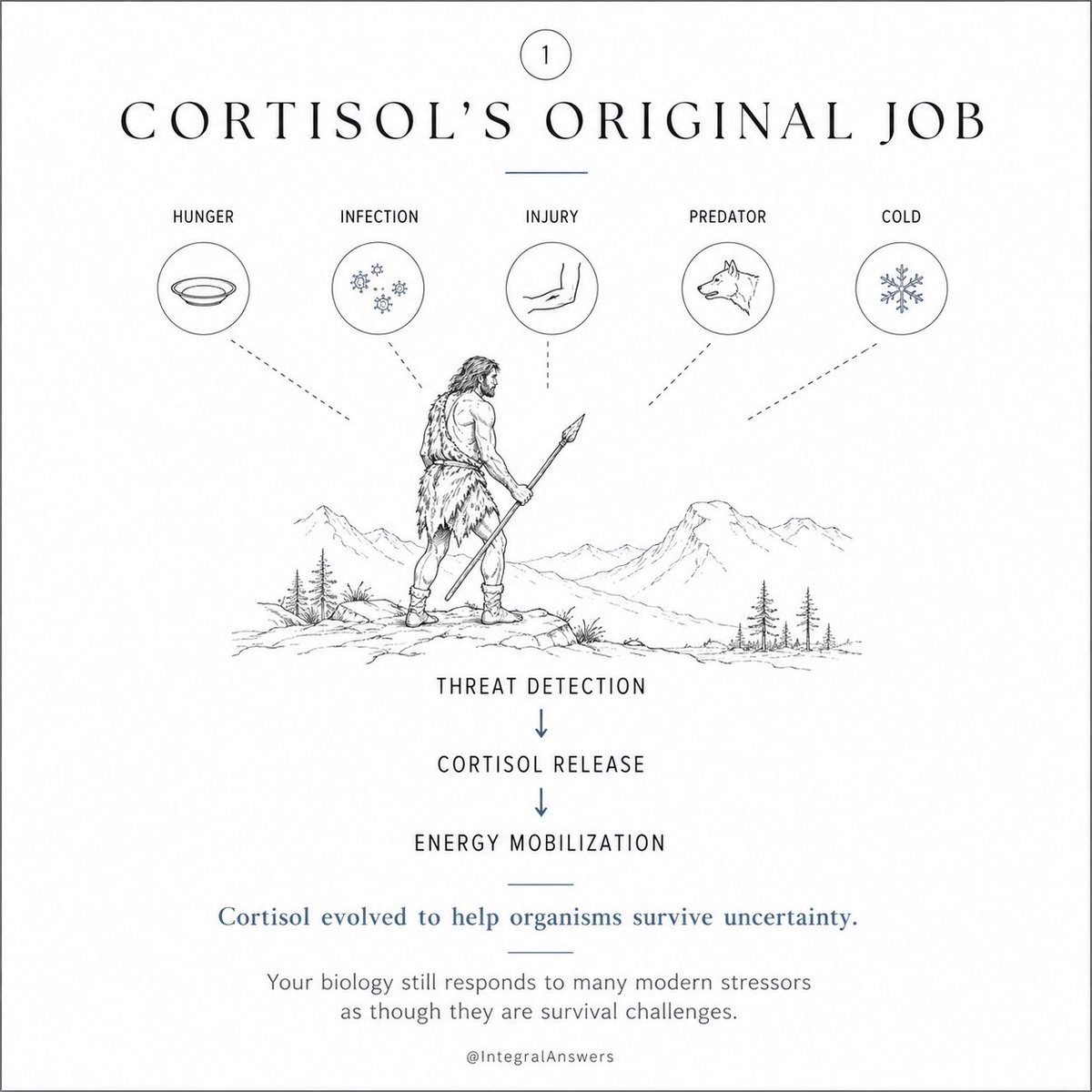
 1/ One of the most striking ideas from Ezra Klein’s conversation with Julia Belluz is that GLP-1 drugs may be teaching us something profound about obesity:
1/ One of the most striking ideas from Ezra Klein’s conversation with Julia Belluz is that GLP-1 drugs may be teaching us something profound about obesity:
 1/ Phase 1: Structural Extraction
1/ Phase 1: Structural Extraction 
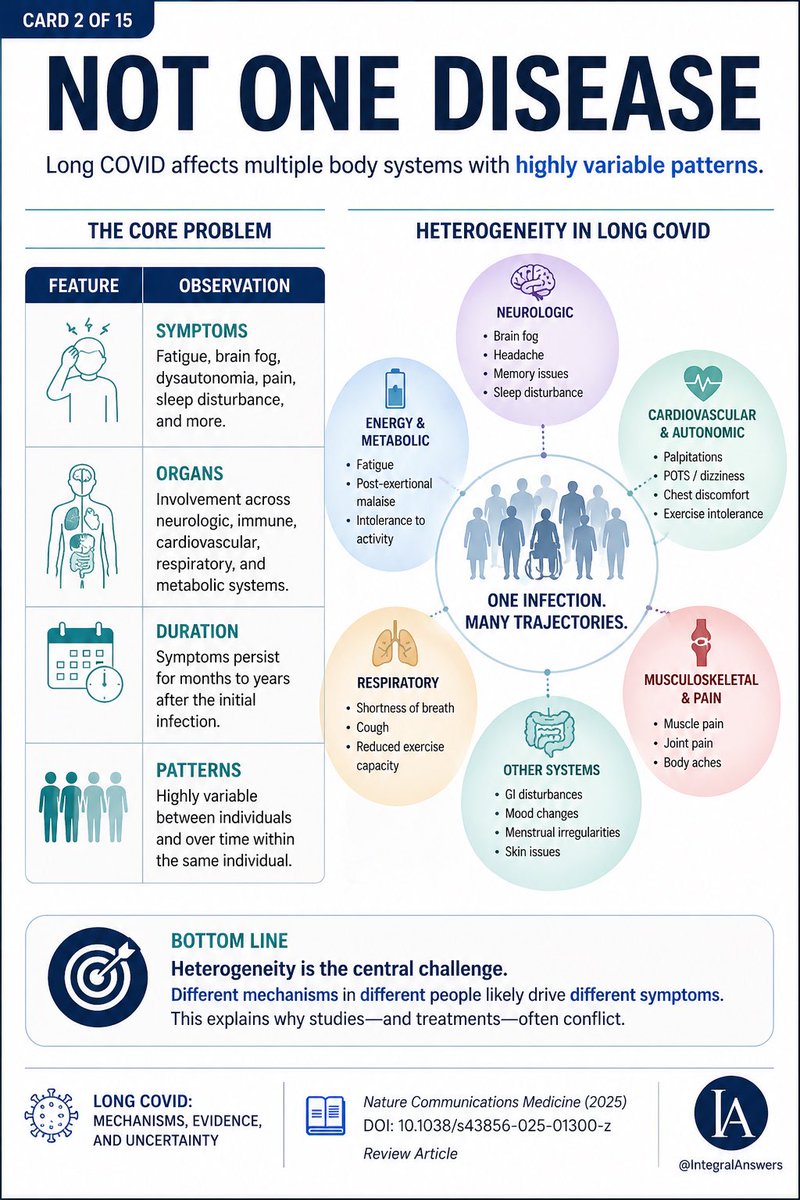
 2/15
2/15
 1/ Chronic inflammation may be one of the most important hidden drivers of modern disease.
1/ Chronic inflammation may be one of the most important hidden drivers of modern disease.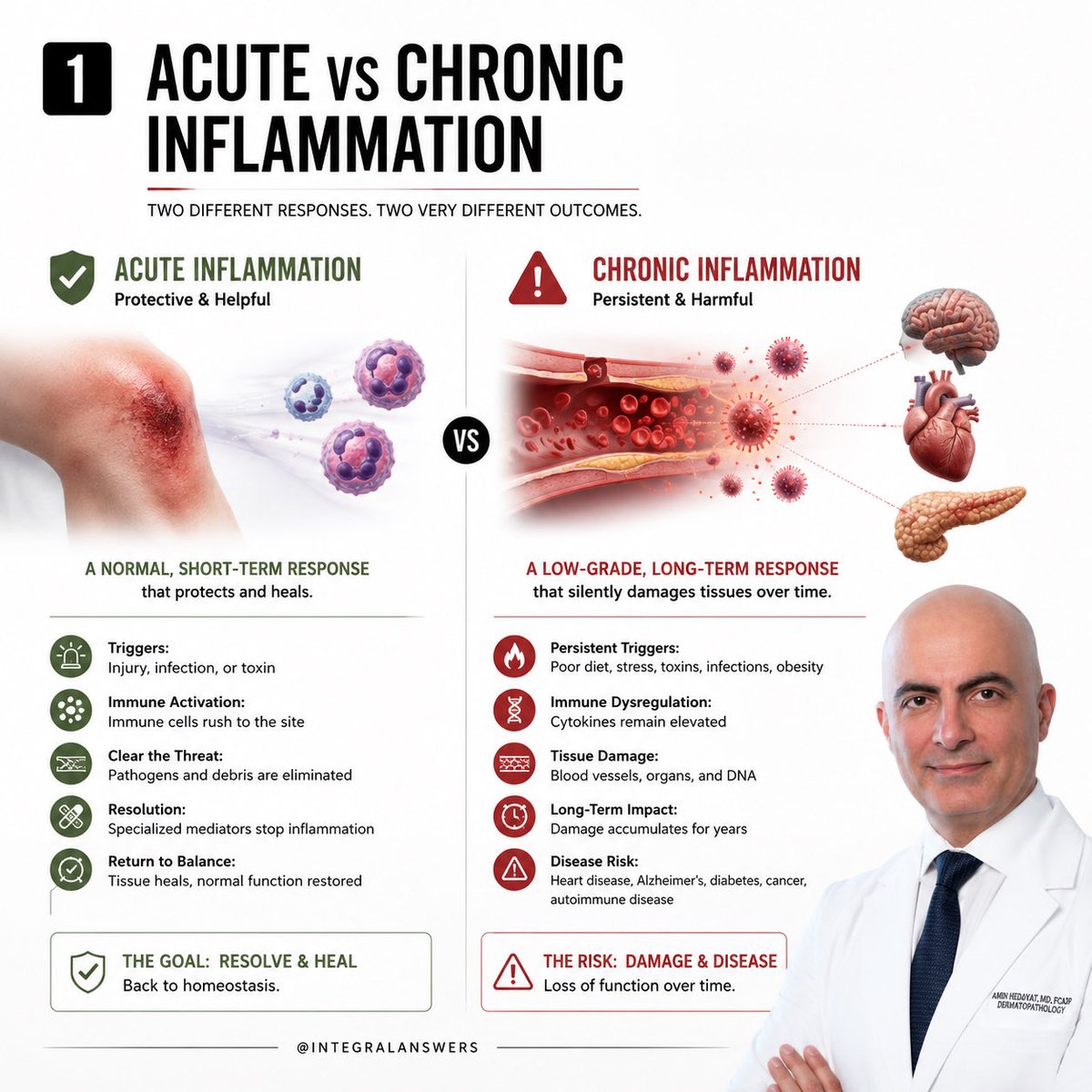
 2/ The review included:
2/ The review included: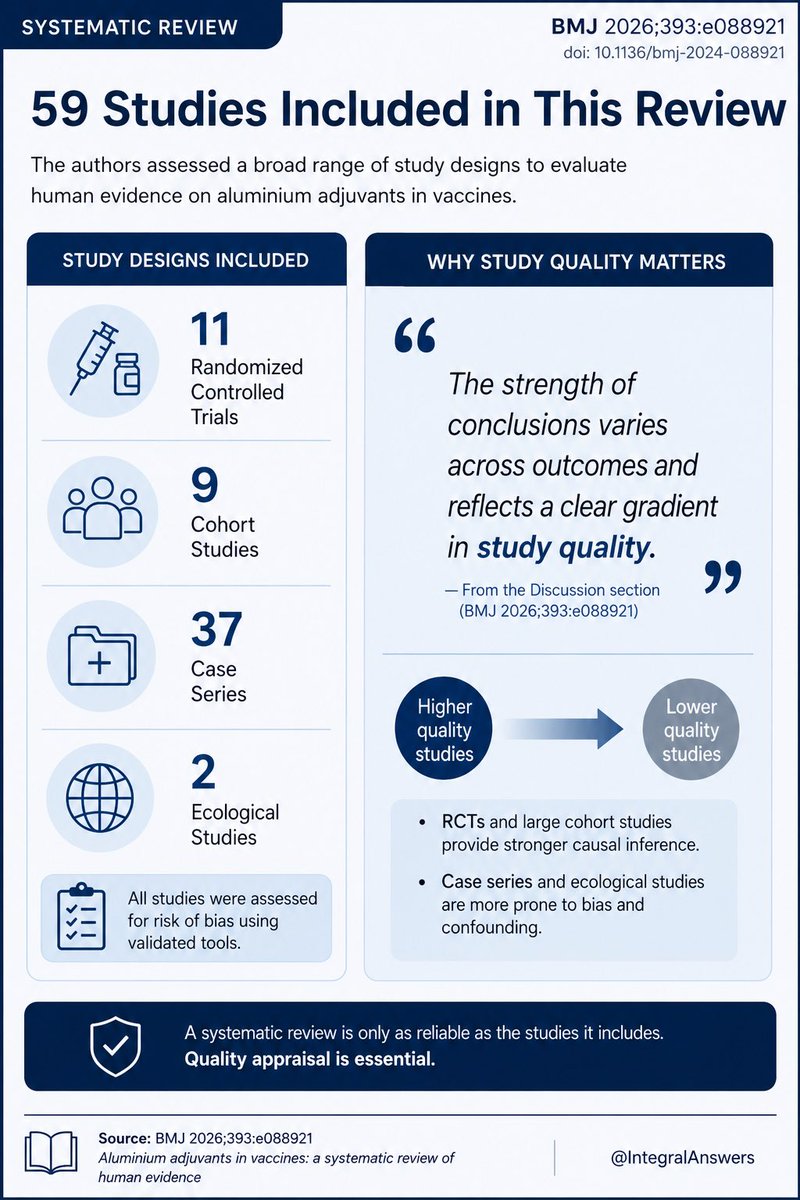
 2/ We’ve shifted from expert guidance → individual decision-making.
2/ We’ve shifted from expert guidance → individual decision-making.
 2/ The Protocol
2/ The Protocol
 2/ The biggest mistake?
2/ The biggest mistake?