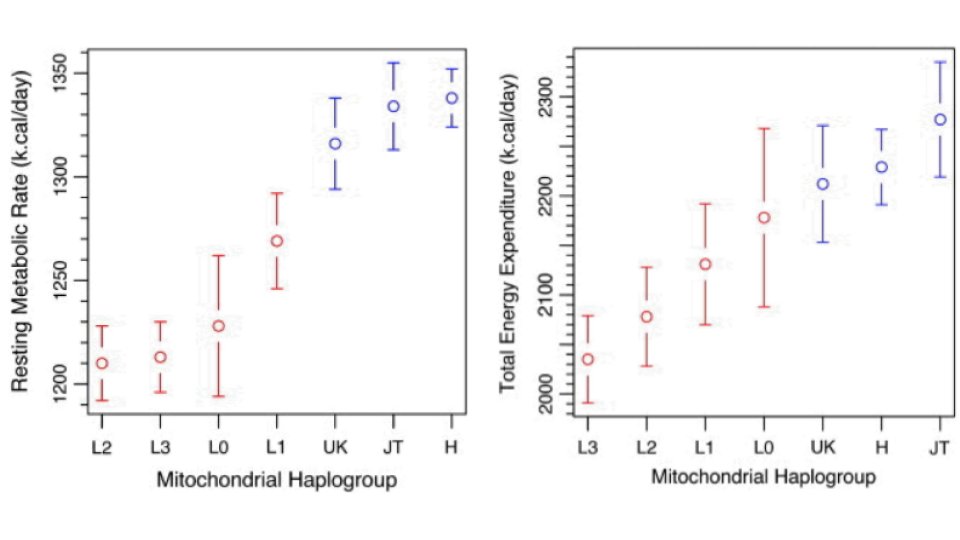
Resting metabolic rate and total energy expenditure tend to differ, on average, across human mitochondrial haplogroups, after adjusting for age, sex, and lean mass.
For example, L haplotypes tend to have lower resting metabolic rate and total energy expenditure compared to UK, JT, and H.
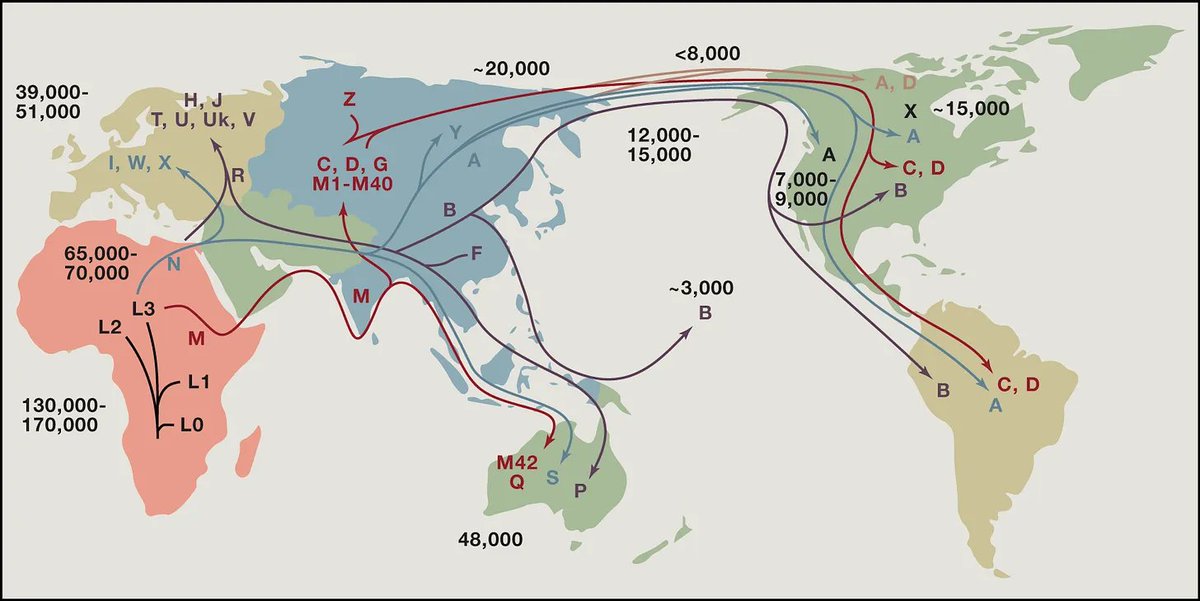
L haplogroups originated in Africa and tend to be more "coupled," which basically means more efficient at ATP synthesis.
UK, H, and JT haplogroups arose in more Northern latitudes (colder climates) and tend to be more uncoupled, i.e. produce more heat.
For example, L haplotypes tend to have lower resting metabolic rate and total energy expenditure compared to UK, JT, and H.
L haplogroups originated in Africa and tend to be more "coupled," which basically means more efficient at ATP synthesis.
UK, H, and JT haplogroups arose in more Northern latitudes (colder climates) and tend to be more uncoupled, i.e. produce more heat.
• • •
Missing some Tweet in this thread? You can try to
force a refresh