UK COVID INQUIRY - CVF💙💜💗
@AdamWagner1 Closing Submissions
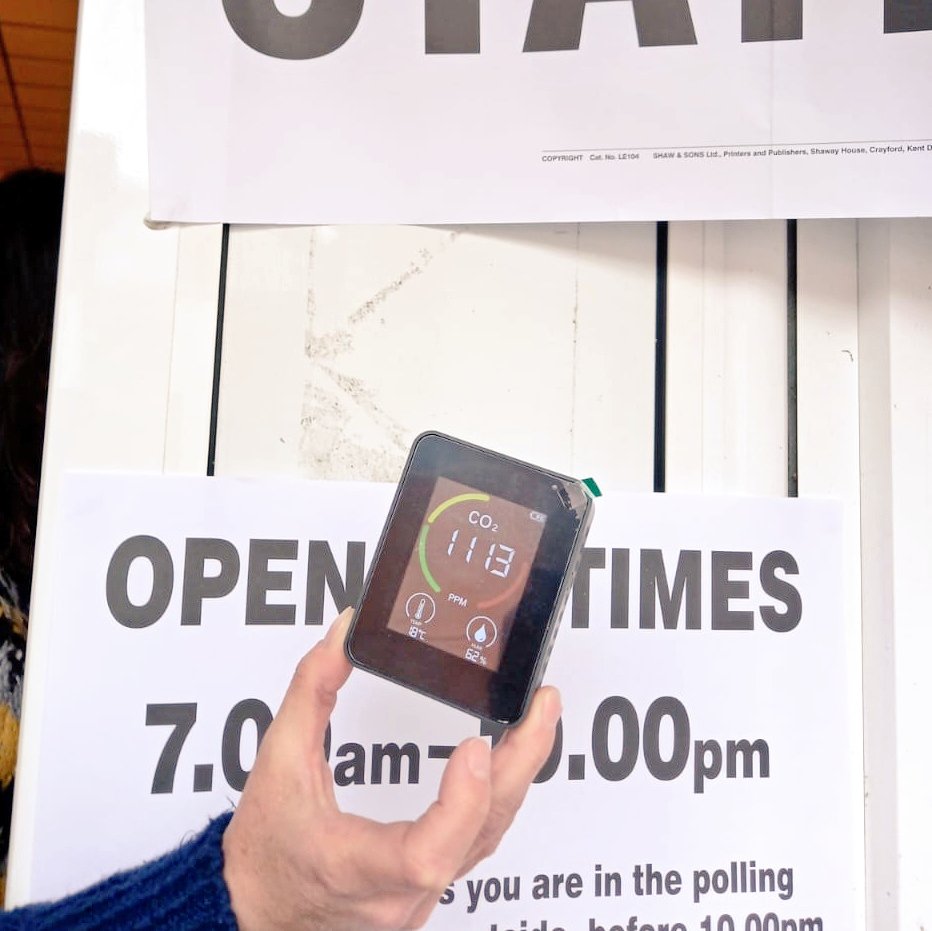
The Covid Inquiry has good ventilation protocols (as advised by CVF at the start of the Inquiry) including HEPA filters.
Under 1000ppm is therefore the safe threshold ( but without it would be under 800ppm).
1/
@AdamWagner1 Closing Submissions
The Covid Inquiry has good ventilation protocols (as advised by CVF at the start of the Inquiry) including HEPA filters.
Under 1000ppm is therefore the safe threshold ( but without it would be under 800ppm).
1/
We need to understand airborne transmission in order to make all indoor environments safer for everyone, and especially for Clinically Vulnerable people.
2/
2/
The need for Clinically Vulnerable people to have:
Safety
Support
& Status
3/
Safety
Support
& Status
3/
1. Safety
"Clinically Vulnerable people cannot reliably make themselves SAFE in indoor settings. The responsibility fall on those who design and manage the environment."
4/
"Clinically Vulnerable people cannot reliably make themselves SAFE in indoor settings. The responsibility fall on those who design and manage the environment."
4/
"In the workplace the absence of enforceable right to adjustments which control the risk of infection continues to leave Clinically Vulnerable people exposed to danger."
5/
5/
We challenged the idea that people simply fearful, but had legitimate concerns.
Prof Nazroo
"The two go together. So if you are Clinically Vulnerable then you are concerned about your heath, and if you don't have adequate protections those concerns will be amplified."
6/
Prof Nazroo
"The two go together. So if you are Clinically Vulnerable then you are concerned about your heath, and if you don't have adequate protections those concerns will be amplified."
6/
Powerful witness, @SamSmithHiggins from @CovidBereaved Cymru said
We were told you can't visit in hospital, well why not? Because, actually if you have the right ventilation, you'd have the right masks - there we no issues whatsoever!"
7/
We were told you can't visit in hospital, well why not? Because, actually if you have the right ventilation, you'd have the right masks - there we no issues whatsoever!"
7/
"The protection against airborne pathogens has to take place, upstream - at source - in the indoor environments where they might spread... and this has to happen through legal protections. Because there is no downstream protection from lawyers who can sue on your behalf."
8/
8/
Challenges accessing mental health support.
9/
9/
CVF's @lara_wong:
"The failure to provide even minimal accommodations, such as support for those who mask or outdoor events, was exclusionary."
10/
"The failure to provide even minimal accommodations, such as support for those who mask or outdoor events, was exclusionary."
10/
Stigma and hostility
Rivka Gottlieb from CBFFJ "There are ongoing issues today that could be so easily addressed:
💉 Wider access to vaccination
💨 Legislation around air quality
😷 Mask wearing in healthcare settings
that would protect the vulnerable."
11/
Rivka Gottlieb from CBFFJ "There are ongoing issues today that could be so easily addressed:
💉 Wider access to vaccination
💨 Legislation around air quality
😷 Mask wearing in healthcare settings
that would protect the vulnerable."
11/
2. Support
"Reopening was not experienced as freedom."
12/
"Reopening was not experienced as freedom."
12/
3. Status
"CVF requests that the Inquiry recommends an important step to protect those people:
the ammendment of the Equality Act to include clinical vulnerability as a protected characteristic"
13/
"CVF requests that the Inquiry recommends an important step to protect those people:
the ammendment of the Equality Act to include clinical vulnerability as a protected characteristic"
13/
Conclusion
"Before the pandemic, Clinically Vulnerable people were invisible, but they must never be invisible again."
👏👏👏 Please do share your thanks (below) to our wonderful legal team. 💕
14/
"Before the pandemic, Clinically Vulnerable people were invisible, but they must never be invisible again."
👏👏👏 Please do share your thanks (below) to our wonderful legal team. 💕
14/
• • •
Missing some Tweet in this thread? You can try to
force a refresh