The Clinical Research of the Chronic Cough After COVID-19 Infection
🚨Waking up coughing every night after COVID? #ChronicCough
🚨More possible Vagus, aka #JoffeNerve pathology! @DavidJoffe64 😉
➡️ Large retrospective study from China on post-COVID cough (primarily Omicron-era, Jan–Jun 2023):
➡️ Study population & design: 1434 outpatients (mean age ~49 years, ~67% female) with cough after SARS-CoV-2 infection, divided into 3 groups: acute (2–3 weeks, n=248), subacute (3–8 weeks, n=705), and chronic (>8 weeks, n=481) groups,
➡️ Chronic cough subgroup: 453 patients detailed via questionnaire (mean age 45, 64% female, mostly non-smokers/vaccinated). Follow-up in 233 patients at median 19 months (18–21 months range), with 17.6% (41/233) showing persistent cough.
➡️ Distinct features in chronic group (vs acute/subacute):
- Higher pre-existing rhinitis/pharyngitis history,
- More pharyngeal symptoms during cough (26.2%, p<0.001),
- Greater sensitivity to odors/cold air (19.5%, p<0.001),
- Elevated eosinophil % (1.70%) and basophil % (0.50%); lower platelet counts (p=0.006),
- More pulmonary micro-nodules on CT. Fewer acute lesions (ground-glass opacities, cord-like shadows, infectious changes; all p<0.01),
➡️ Pulmonary function in chronic cases: Partial ventilatory impairment (reduced FVC, FEV1, small airway indices, PEF, MEF25/50/75), decreased diffusing capacity (DLCO/DLCO%), ~35% abnormal ventilation, ~36% reduced diffusion,
➡️Predictors of long-term persistence (at ~19-month follow-up):
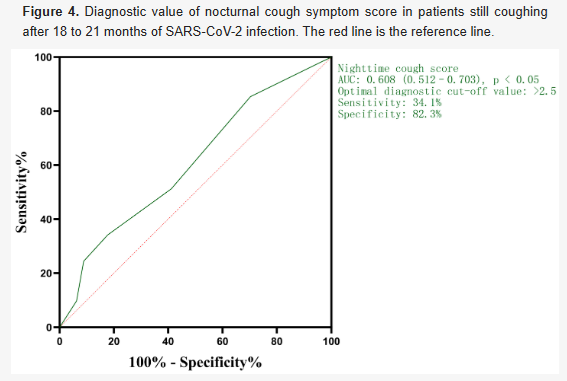
- Higher baseline nocturnal cough scores.
- Cough accompanied by chest tightness (more frequent in persistent cases, p=0.022).
- Binary logistic regression: Nocturnal score (OR 1.72 per point) and chest tightness (OR 3.5) as independent predictors.
- Nocturnal score showed modest diagnostic value (AUC 0.608, cut-off 2.5).
➡️Other notes: No major differences in age, gender, smoking, many chronic patients had phlegm (63%), chest tightness/wheezing (72%), limited response to common treatments.
➡️Sadly, this study provides no evidence or insights into whether reinfections or vaccination status modifies the risk, course, or persistence of post-COVID chronic cough, leaving these as unexplored variables!
➡️Well-noted limitations.
‼️Significant clinical importance in a broader long COVID context: Chronic cough affects 10–20%+ of survivors long-term, often clustering with dyspnoea/fatigue. Identifying predictors like above helps prioritize identifying these long Covid subsets, reduces unnecessary testing, and should further guide research into shared neuroinflammatory mechanisms across long COVID symptoms.
‼️Reminder: Neurogenic cough is strongly and directly related to the vagus nerve (cranial nerve X).
Neurogenic cough is fundamentally a vagus nerve dysfunction, specifically hypersensitivity or neuropathy of its sensory airway branches, turning a protective reflex into a chronic, self-perpetuating cycle rather than a simple respiratory symptom.
‼️So, according to the authors, severe nocturnal cough combined with chest tightness emerges as a powerful, independent indication of post-COVID chronic cough that can last for up to nearly two years(study duration), pointing to a separate, likely NEUROGENIC or airway-hyperresponsive entity rather than just an unusually lingering phase of the original acute inflammatory process.
#AvoidSars2 #AvoidReinfections
mdpi.com/2077-0383/15/6…
🚨Waking up coughing every night after COVID? #ChronicCough
🚨More possible Vagus, aka #JoffeNerve pathology! @DavidJoffe64 😉
➡️ Large retrospective study from China on post-COVID cough (primarily Omicron-era, Jan–Jun 2023):
➡️ Study population & design: 1434 outpatients (mean age ~49 years, ~67% female) with cough after SARS-CoV-2 infection, divided into 3 groups: acute (2–3 weeks, n=248), subacute (3–8 weeks, n=705), and chronic (>8 weeks, n=481) groups,
➡️ Chronic cough subgroup: 453 patients detailed via questionnaire (mean age 45, 64% female, mostly non-smokers/vaccinated). Follow-up in 233 patients at median 19 months (18–21 months range), with 17.6% (41/233) showing persistent cough.
➡️ Distinct features in chronic group (vs acute/subacute):
- Higher pre-existing rhinitis/pharyngitis history,
- More pharyngeal symptoms during cough (26.2%, p<0.001),
- Greater sensitivity to odors/cold air (19.5%, p<0.001),
- Elevated eosinophil % (1.70%) and basophil % (0.50%); lower platelet counts (p=0.006),
- More pulmonary micro-nodules on CT. Fewer acute lesions (ground-glass opacities, cord-like shadows, infectious changes; all p<0.01),
➡️ Pulmonary function in chronic cases: Partial ventilatory impairment (reduced FVC, FEV1, small airway indices, PEF, MEF25/50/75), decreased diffusing capacity (DLCO/DLCO%), ~35% abnormal ventilation, ~36% reduced diffusion,
➡️Predictors of long-term persistence (at ~19-month follow-up):
- Higher baseline nocturnal cough scores.
- Cough accompanied by chest tightness (more frequent in persistent cases, p=0.022).
- Binary logistic regression: Nocturnal score (OR 1.72 per point) and chest tightness (OR 3.5) as independent predictors.
- Nocturnal score showed modest diagnostic value (AUC 0.608, cut-off 2.5).
➡️Other notes: No major differences in age, gender, smoking, many chronic patients had phlegm (63%), chest tightness/wheezing (72%), limited response to common treatments.
➡️Sadly, this study provides no evidence or insights into whether reinfections or vaccination status modifies the risk, course, or persistence of post-COVID chronic cough, leaving these as unexplored variables!
➡️Well-noted limitations.
‼️Significant clinical importance in a broader long COVID context: Chronic cough affects 10–20%+ of survivors long-term, often clustering with dyspnoea/fatigue. Identifying predictors like above helps prioritize identifying these long Covid subsets, reduces unnecessary testing, and should further guide research into shared neuroinflammatory mechanisms across long COVID symptoms.
‼️Reminder: Neurogenic cough is strongly and directly related to the vagus nerve (cranial nerve X).
Neurogenic cough is fundamentally a vagus nerve dysfunction, specifically hypersensitivity or neuropathy of its sensory airway branches, turning a protective reflex into a chronic, self-perpetuating cycle rather than a simple respiratory symptom.
‼️So, according to the authors, severe nocturnal cough combined with chest tightness emerges as a powerful, independent indication of post-COVID chronic cough that can last for up to nearly two years(study duration), pointing to a separate, likely NEUROGENIC or airway-hyperresponsive entity rather than just an unusually lingering phase of the original acute inflammatory process.
#AvoidSars2 #AvoidReinfections
mdpi.com/2077-0383/15/6…
• • •
Missing some Tweet in this thread? You can try to
force a refresh