MENINGITIS B TRANSMISSION
There’s been a lot of discussion online and in the media about how exactly Meningitis B spreads.
A lot of it is conflicting & confusing.
So let’s put opinions & hearsay aside and take a proper look at what the latest science actually tells us…
🧵
There’s been a lot of discussion online and in the media about how exactly Meningitis B spreads.
A lot of it is conflicting & confusing.
So let’s put opinions & hearsay aside and take a proper look at what the latest science actually tells us…
🧵

The UK National Institute for Health & Care Excellence (NICE) states that bacterial meningitis and meningococcal disease is transmitted by the following 3 modes:
▪️ aerosol
▪️droplets
▪️direct contact
cks.nice.org.uk/topics/meningi…
▪️ aerosol
▪️droplets
▪️direct contact
cks.nice.org.uk/topics/meningi…
The first of these modes of transmission, AEROSOL, has been the subject of heated debate.
Let’s look at why…
Notice the second line:
“Transmission usually requires either frequent or prolonged close contact.”
At first, this may seem contradictory with aerosol transmission…
Let’s look at why…
Notice the second line:
“Transmission usually requires either frequent or prolonged close contact.”
At first, this may seem contradictory with aerosol transmission…
‘Aerosols’ are the smaller, lighter respiratory particles which have the potential to remain airborne for many hours and to travel considerable distances.
So, if aerosols are a factor, why does the guidance suggest that transmission of meningococcus bacteria needs close contact?
So, if aerosols are a factor, why does the guidance suggest that transmission of meningococcus bacteria needs close contact?
Well, there’s one more very important factor to consider…
…and that’s how long the meningococcus bacteria (Neisseria meningitidis) can survive in the air after being exhaled.
Very little was known about the survival of this bacteria in aerosols until recently…
…and that’s how long the meningococcus bacteria (Neisseria meningitidis) can survive in the air after being exhaled.
Very little was known about the survival of this bacteria in aerosols until recently…
Ongoing research at Bristol University has been studying this for the past few years.
Their research has revealed that there is a “significant drop in survival after just 15 secs of aerosolisation, with some strains showing little survival after 5 mins”.
meningitisnow.org/meningitis-exp…
Their research has revealed that there is a “significant drop in survival after just 15 secs of aerosolisation, with some strains showing little survival after 5 mins”.
meningitisnow.org/meningitis-exp…
So that helps explain why “prolonged & close contact” is often cited as being required.
The bacteria *is* in aerosols but - unlike viruses like Covid & measles which can survive in the air for hours - the meningococcus bacteria doesn’t live very long once exhaled in aerosols.
The bacteria *is* in aerosols but - unlike viruses like Covid & measles which can survive in the air for hours - the meningococcus bacteria doesn’t live very long once exhaled in aerosols.

The study also revealed some factors which can extend the survival rate of meningococcus bacteria.
For example, all tested strains showed longer survival times when relative humidity was increased.
In a crowded nightclub, thick with vaping smoke, could this have been a factor?
For example, all tested strains showed longer survival times when relative humidity was increased.
In a crowded nightclub, thick with vaping smoke, could this have been a factor?
So, now we know that the meningococcus bacteria typically only lives for a few minutes in exhaled aerosols, we can start to visualise what’s happening…
The contagious person will be exhaling BOTH aerosols & droplets containing the bacteria 💨
The contagious person will be exhaling BOTH aerosols & droplets containing the bacteria 💨
As independent expert witness to the Covid Inquiry, Professor Clive Beggs, unequivocally confirmed during his testimony:
There is no situation or scenario where someone could produce a respiratory droplet without ALSO generating significant amounts of aerosols.
There is no situation or scenario where someone could produce a respiratory droplet without ALSO generating significant amounts of aerosols.
The heavier droplets behave ballistically and fall rapidly to the ground…
…whereas the aerosols are lighter and float in the air, spreading outwards in a ‘plume’.
And, of course, the closer you are to the infected person, the denser that plume of aerosols will be.
…whereas the aerosols are lighter and float in the air, spreading outwards in a ‘plume’.
And, of course, the closer you are to the infected person, the denser that plume of aerosols will be.
However, because the bacteria doesn’t survive very long in the air (only a few minutes or so), the concentration of bacteria-laden aerosols doesn’t build up and accumulate in the same way as it does for a virus like Covid which remains infectious in the air for hours.
That said, in a crowded poorly ventilated setting, aerosols can still reach many people in the few minutes it remains viable.
And remember, someone carrying meningococcus will be breathing continuously, producing a steady stream of bacteria-laden (albeit short-lived) aerosols.
And remember, someone carrying meningococcus will be breathing continuously, producing a steady stream of bacteria-laden (albeit short-lived) aerosols.
And so this is where the confusion arises…
Near-field transmission is indeed dominant for meningococcus bacteria, but it is BOTH the aerosols and the droplets which are responsible for that near-field transmission.
Near-field transmission is indeed dominant for meningococcus bacteria, but it is BOTH the aerosols and the droplets which are responsible for that near-field transmission.
In fact, scientific papers on the safe handling of the meningococcal bacteria (Neisseria meningitidis) in laboratories suggest that transmission MAINLY occurs by formation of aerosols generated in the nasopharynx.

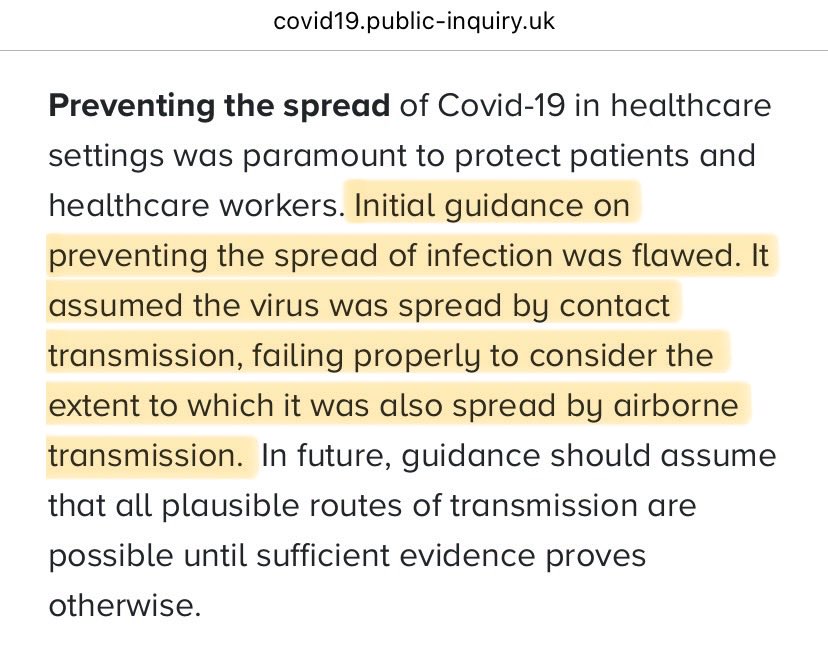
This is also why the Covid Inquiry report has been crystal clear in its findings that “it is no longer appropriate” to rely on the dichotomy between droplets & aerosols.
You can’t have droplets without aerosols.
Failing to guard against aerosol transmission puts people at risk.
You can’t have droplets without aerosols.
Failing to guard against aerosol transmission puts people at risk.

That’s because different mitigations work for different modes of transmission.
😷 Fluid resistant surgical masks may provide some protection against droplets, but do NOT protect against aerosol transmission.
😷 FFP2/3 masks (respirators) are needed to protect against aerosols.
😷 Fluid resistant surgical masks may provide some protection against droplets, but do NOT protect against aerosol transmission.
😷 FFP2/3 masks (respirators) are needed to protect against aerosols.
Here’s another clip from the Covid Inquiry…
…this time from Richard Brunt, Director at the Health & Safety Executive (HSE), explaining how surgical masks may offer limited protection against droplet transmission, but do NOT protect against AIRBORNE transmission.
…this time from Richard Brunt, Director at the Health & Safety Executive (HSE), explaining how surgical masks may offer limited protection against droplet transmission, but do NOT protect against AIRBORNE transmission.
It’s been encouraging to see so many people sensibly wearing masks to protect themselves in the midst of this Meningitis B outbreak…
…but it concerns me that they’re not being given enough information by public health officials on the right TYPE of mask to protect themselves.
…but it concerns me that they’re not being given enough information by public health officials on the right TYPE of mask to protect themselves.
I also worry about the healthcare workers administering the vaccines, coming into close contact with hundreds of students who may potentially be carrying the meningococcus bacteria.
Loose-fitting surgical masks do NOT provide adequate protection against aerosol transmission.
Loose-fitting surgical masks do NOT provide adequate protection against aerosol transmission.

Worse still, some health officials are actively telling people NOT to wear masks because they can:
“create the wrong message”
“spread panic”
“revive memories of Covid”
What utterly absurd reasons to not recommend masking!
This advice may cost lives.
kidneycareuk.org/news-from-kidn…
“create the wrong message”
“spread panic”
“revive memories of Covid”
What utterly absurd reasons to not recommend masking!
This advice may cost lives.
kidneycareuk.org/news-from-kidn…

I really think those in change of infection control for this Meningitis B outbreak need to take an urgent look at the Covid Inquiry report published just a few days ago.
There are no excuses anymore.
The govt MUST NOT make the same mistakes again.
We MUST learn from the past.
There are no excuses anymore.
The govt MUST NOT make the same mistakes again.
We MUST learn from the past.
• • •
Missing some Tweet in this thread? You can try to
force a refresh