Long-Term Thyroid Complications Post-COVID-19: A Systematic Review
🚨COVID-19 didn’t just hit your lungs, it may even hijack your Thyroid for life.
➡️This systematic review from Quatar examines long-term thyroid complications following COVID-19 infection, analysing 28 studies involving 419 patients drawn from a pool of over 408,000 COVID-19 cases.
➡️Overview of their findings:
1. Thyroid disorders:
Subacute thyroiditis (SAT, most common hyperthyroid issue, n=80), thyrotoxicosis (n=35), hyperthyroidism including Graves’ disease (n=23), isolated high T3/T4, hypothyroidism (n=147, often subclinical or Hashimoto’s-related), central hypothyroidism, and non-thyroidal illness syndrome (NTIS),
2. Patterns:
Many cases (especially SAT and thyrotoxicosis) can be transient, resolving within months. However, autoimmune conditions like Graves’ or Hashimoto’s frequently persisted or recurred,
3. Incidence:
SAT risk was significantly elevated post-COVID (HR 1.93–2.30 vs. controls), some studies noted 6.8% incidence within 3 months post-recovery,
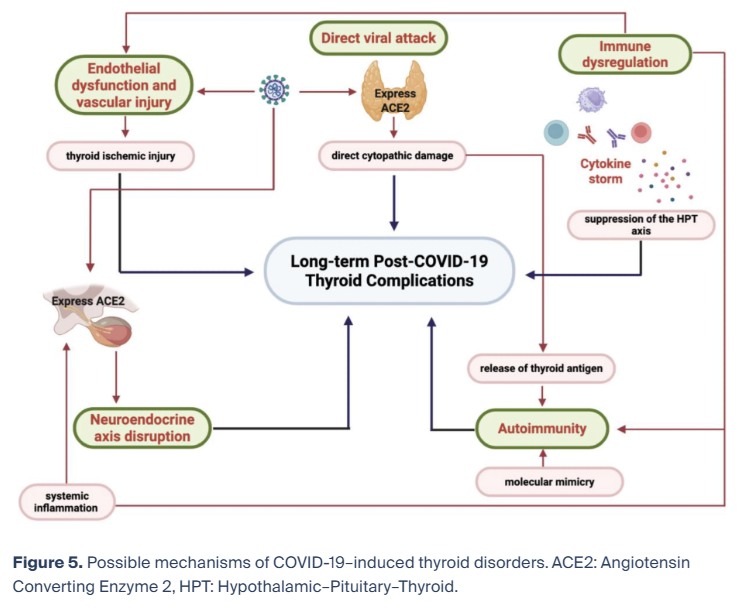
4. Mechanisms:
Direct viral damage via ACE2 receptors on thyroid cells, cytokine storm suppressing the hypothalamic-pituitary-thyroid axis, post-viral autoimmunity (molecular mimicry), vascular injury, and neuroendocrine disruption,
5. Limitations:
Data from 18 countries, but many studies lacked full hormone/autoantibody details or long follow-up, limiting incidence estimates,
6. Recommendations:
Review recommends routine thyroid function screening (TSH, free T4/T3) in the months after recovery, especially for severe cases or those with ongoing symptoms, and calls for integrated long COVID care!
➡️This review highlights COVID-19 as a multisystem disease with lasting endocrine effects, particularly in severe or symptomatic survivors.
‼️Sadly, this review remains silent on vaccines and reinfections impact, leaving open the critical question of how they may alter the trajectory of COVID-triggered autoimmune thyroid disease.
‼️Nonetheless, COVID-19 can trigger persistent autoimmune thyroid destruction that may even never fully resolve, turning a respiratory virus into a lifelong endocrine threat for many survivors.
‼️So, this review establishes that COVID-19 can permanently reprogram thyroid immunity in a subset of survivors, making systematic endocrine surveillance a necessary part of post-infection follow-up! You’re warned again!
#AvoidSars2 #AvoidReinfections
mdpi.com/2076-2607/14/3…
🚨COVID-19 didn’t just hit your lungs, it may even hijack your Thyroid for life.
➡️This systematic review from Quatar examines long-term thyroid complications following COVID-19 infection, analysing 28 studies involving 419 patients drawn from a pool of over 408,000 COVID-19 cases.
➡️Overview of their findings:
1. Thyroid disorders:
Subacute thyroiditis (SAT, most common hyperthyroid issue, n=80), thyrotoxicosis (n=35), hyperthyroidism including Graves’ disease (n=23), isolated high T3/T4, hypothyroidism (n=147, often subclinical or Hashimoto’s-related), central hypothyroidism, and non-thyroidal illness syndrome (NTIS),
2. Patterns:
Many cases (especially SAT and thyrotoxicosis) can be transient, resolving within months. However, autoimmune conditions like Graves’ or Hashimoto’s frequently persisted or recurred,
3. Incidence:
SAT risk was significantly elevated post-COVID (HR 1.93–2.30 vs. controls), some studies noted 6.8% incidence within 3 months post-recovery,
4. Mechanisms:
Direct viral damage via ACE2 receptors on thyroid cells, cytokine storm suppressing the hypothalamic-pituitary-thyroid axis, post-viral autoimmunity (molecular mimicry), vascular injury, and neuroendocrine disruption,
5. Limitations:
Data from 18 countries, but many studies lacked full hormone/autoantibody details or long follow-up, limiting incidence estimates,
6. Recommendations:
Review recommends routine thyroid function screening (TSH, free T4/T3) in the months after recovery, especially for severe cases or those with ongoing symptoms, and calls for integrated long COVID care!
➡️This review highlights COVID-19 as a multisystem disease with lasting endocrine effects, particularly in severe or symptomatic survivors.
‼️Sadly, this review remains silent on vaccines and reinfections impact, leaving open the critical question of how they may alter the trajectory of COVID-triggered autoimmune thyroid disease.
‼️Nonetheless, COVID-19 can trigger persistent autoimmune thyroid destruction that may even never fully resolve, turning a respiratory virus into a lifelong endocrine threat for many survivors.
‼️So, this review establishes that COVID-19 can permanently reprogram thyroid immunity in a subset of survivors, making systematic endocrine surveillance a necessary part of post-infection follow-up! You’re warned again!
#AvoidSars2 #AvoidReinfections
mdpi.com/2076-2607/14/3…
• • •
Missing some Tweet in this thread? You can try to
force a refresh