Don't Let Your Lives "Narrow"!!
I've been an orthopedic surgeon for 30 years.
The thing I watch happen to people, more than any injury or surgery, is refer to as the narrowing.
Most of my patients have no idea it's happening to them. They think it's just aging. It's not. 🧵
I've been an orthopedic surgeon for 30 years.
The thing I watch happen to people, more than any injury or surgery, is refer to as the narrowing.
Most of my patients have no idea it's happening to them. They think it's just aging. It's not. 🧵
The narrowing is the slow shrinking of what your body will let you do... or what you assume your body can or should be doing at your age.
You used to carry four grocery bags. Now you take two. You used to sit on the floor with the grandkids. Now you sit on the couch and watch. You used to take the stairs two at a time. Now you hold the rail.
If you're under 80 and you lie down for an injection... you shouldn't need a two armed lift to sit back up. Granted... in some instances you will... but I'm speaking about the "healthy" 60-70 something that can't because they never recognized this loss of ability and never did something about it.
You used to carry four grocery bags. Now you take two. You used to sit on the floor with the grandkids. Now you sit on the couch and watch. You used to take the stairs two at a time. Now you hold the rail.
If you're under 80 and you lie down for an injection... you shouldn't need a two armed lift to sit back up. Granted... in some instances you will... but I'm speaking about the "healthy" 60-70 something that can't because they never recognized this loss of ability and never did something about it.
Nobody decides to narrow their lives intentionally. You don't wake up one morning and choose a smaller life.
Your body quietly loses some capacity, and your daily choices adjust to the loss, and within a few years the smaller version is your new normal.
And the memory of the larger version gets filed away under "when I was younger."
Your body quietly loses some capacity, and your daily choices adjust to the loss, and within a few years the smaller version is your new normal.
And the memory of the larger version gets filed away under "when I was younger."
Patients tell me about the narrowing every single day. They just don't use that word.
They say: "I can't do what I used to do."
They say: "I'm getting older."
They say: "That's just what happens at my age."
And they say it as if it's a law of physics.
They say: "I can't do what I used to do."
They say: "I'm getting older."
They say: "That's just what happens at my age."
And they say it as if it's a law of physics.
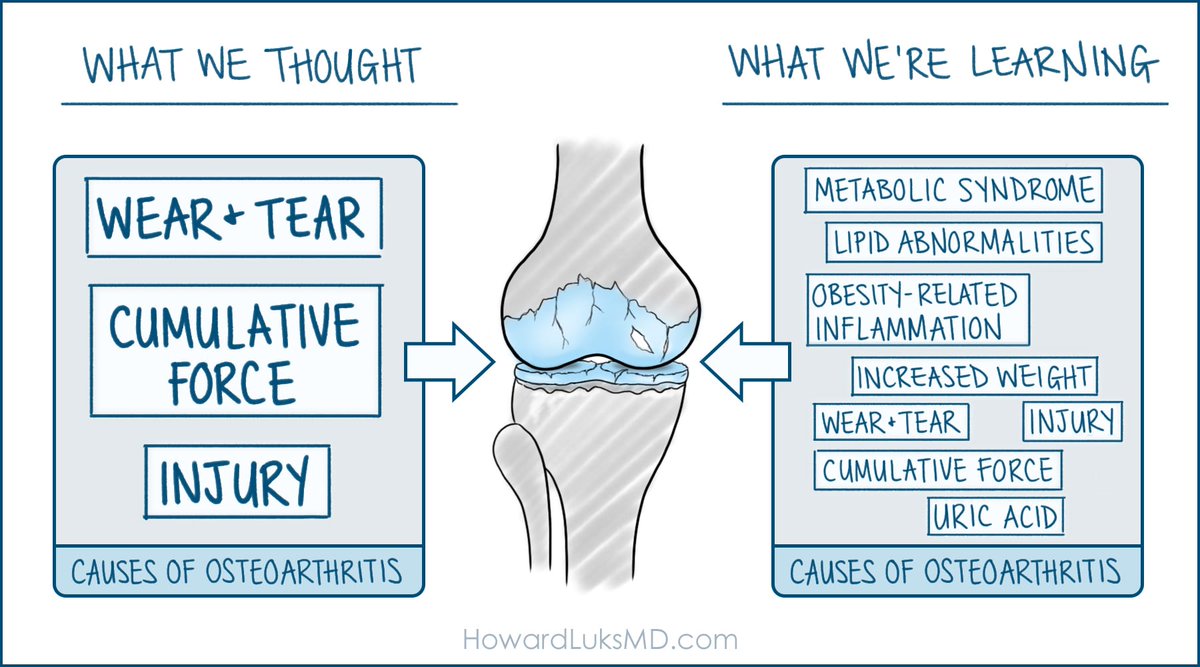
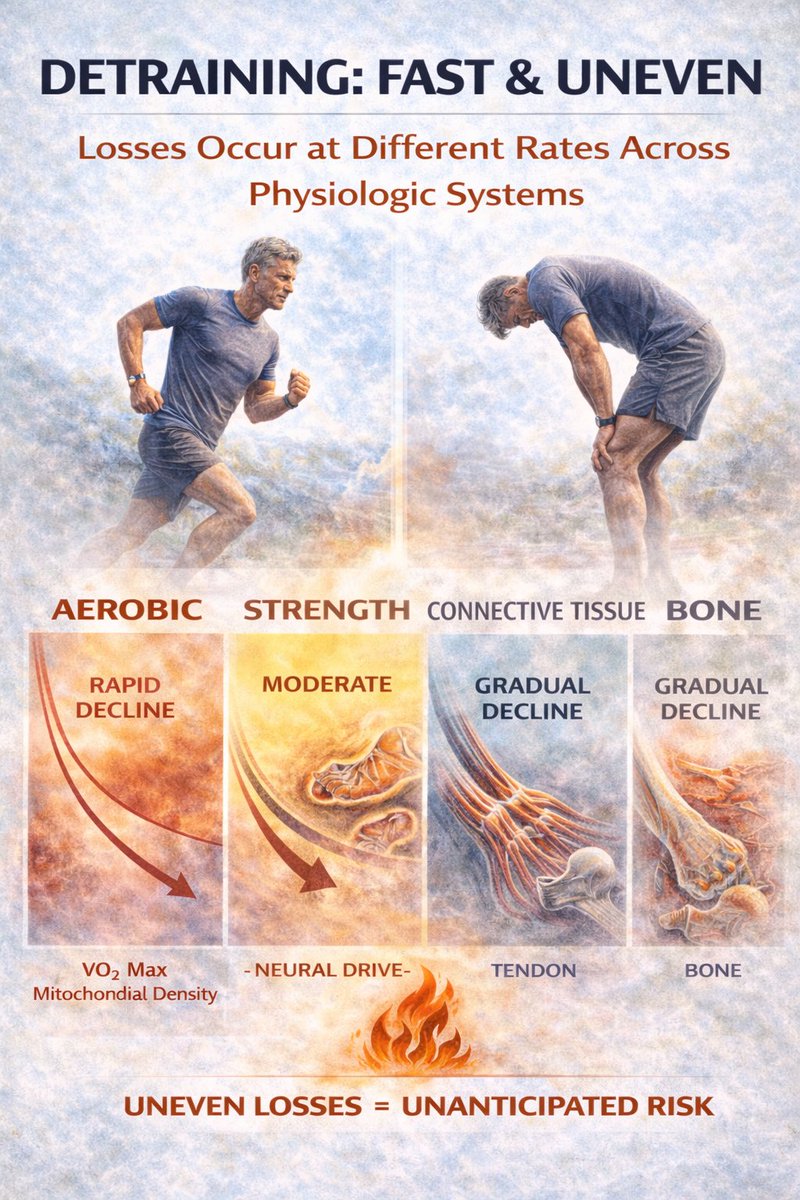
Yes! Some decline is real and unavoidable. VO2 max drops. Max heart rate drops. Strength drops. Power drops faster than strength. Quickness drops. Proprioception drops. I see these changes in the gym all the time. Especially power and quickness.
But... The unavoidable decline is only a small fraction of what most people are actually losing.
The rest, the bigger part, the part that turns a sixty-year-old into a frail seventy-year-old, is not aging.
It is disuse.
The rest, the bigger part, the part that turns a sixty-year-old into a frail seventy-year-old, is not aging.
It is disuse.
The cruelest part of the narrowing is that people normalize it. They don't question it. They talk about capacities they've lost as if losing them was scheduled.
They simply adjust their lives and activities to their list of limitations.
They simply adjust their lives and activities to their list of limitations.
When patients see me running, climbing, lifting at 62, a common response is: "Well, you're different. You're built for this."
I was not uniquely built for this. I built myself for this. Every week, on purpose, for decades.
What they see as genetic luck is accumulated work.
I was not uniquely built for this. I built myself for this. Every week, on purpose, for decades.
What they see as genetic luck is accumulated work.
Most of my patients could be doing most of what I do.
Not all of them. Some have real structural problems. Some have diseases and disabilities. Some are genuinely limited.
But the majority are limited by the decade or two of training they did not do.
Not all of them. Some have real structural problems. Some have diseases and disabilities. Some are genuinely limited.
But the majority are limited by the decade or two of training they did not do.
Once the narrowing starts, it accelerates on its own.
You stop lifting heavy things. Your muscles lose fast-twitch fibers. You get weaker. You lift even less. You lose more. The loss feels like aging. You accept it. The loop tightens.
You stop lifting heavy things. Your muscles lose fast-twitch fibers. You get weaker. You lift even less. You lose more. The loss feels like aging. You accept it. The loop tightens.
Again... aging brings some changes. VO2 max declines about 10% per decade in sedentary adults. Strength declines slowly starting in the forties. Power declines about twice as fast as strength after fifty. Bone density drops. Balance degrades.
Get over it... you still have agency and lost abilities to recover.
Get over it... you still have agency and lost abilities to recover.
The slope and severity of every one of those declines is profoundly modifiable with training. The sedentary decline curves are not the human decline curves. They are the untrained decline curves.
Trained adults in their seventies routinely outperform untrained adults in their fifties.
Trained adults in their seventies routinely outperform untrained adults in their fifties.
The gap between what aging takes from you and what disuse takes from you is huge. Most people can't tell the two apart, because nobody showed them the difference.
They live inside a body that is losing capacity fast, and they attribute the whole thing to a calendar.
They live inside a body that is losing capacity fast, and they attribute the whole thing to a calendar.
I have watched patients in their seventies start from positions that would make a physical therapist flinch, and rebuild themselves into versions of themselves their own families barely recognized.
Not by becoming athletes. By doing small, specific work, consistently, for months and then years.
Not by becoming athletes. By doing small, specific work, consistently, for months and then years.
The body remains responsive to training well into the seventies and eighties. This is one of the best-established findings in the literature on aging.
Almost nobody's doctor tells them about it.
Almost nobody's doctor tells them about it.
The patients who reverse the narrowing are not the ones with the best genetics, or the best knees, or the best circumstances.
They are the ones who decided to do something.
Something made them stop accepting the losses as inevitable, and they started doing things differently from that day forward.
They are the ones who decided to do something.
Something made them stop accepting the losses as inevitable, and they started doing things differently from that day forward.
What have you already stopped doing?
Not what you can't do, exactly. What have you quietly stopped doing over the last five or ten years, without ever making a real decision about it?
Not what you can't do, exactly. What have you quietly stopped doing over the last five or ten years, without ever making a real decision about it?
And more importantly: did your body actually tell you to stop, or did you assume you needed to?
one of the most common finding in my office is that patients have stopped doing things their bodies could still do, on the basis of assumptions that were never tested.
They basically narrowed preemptively.
one of the most common finding in my office is that patients have stopped doing things their bodies could still do, on the basis of assumptions that were never tested.
They basically narrowed preemptively.
Most of the narrowing in your life right now is reversible. I have watched it happen in thousands of patients. It is not a miracle. It is just the body doing what the body does when you start asking it to do something again.
The door you thought had closed is usually still open.
The door you thought had closed is usually still open.

I am not a one-off. I am a sixty-two-year-old who decided not to let my life narrow, and who did the specific work to back the decision up, for long enough that the work is now visible from the outside.
You can do this too. At any age I am likely to be talking to.
Start where you are. Start this week.
You can do this too. At any age I am likely to be talking to.
Start where you are. Start this week.

More depth...
howardluksmd.substack.com/p/training-at-…
howardluksmd.substack.com/p/training-at-…
• • •
Missing some Tweet in this thread? You can try to
force a refresh