I'm a 62-year-old orthopedic surgeon, trail runner, climber, and cyclist. This is my Midlife Athlete's Playbook. I've combined what I've learned from 30+ years of treating active adults, and from training through my own 50s and 60s. The physiology of aging is real, but most of the decline people accept is optional.
Aging brings real physiological changes. But lack of specific age-appropriate training brings far worse ones. A few things I've learned from three decades of treating active adults and from my own body.
After 30, muscle mass declines 3 to 8% per decade. After 50, it accelerates to 1-2% per year. The biology is real: anabolic resistance increases, satellite cell populations decline, and the signaling that drives hypertrophy becomes less efficient. But muscle still responds to progressive load at every age. The response is harder to earn, which means the training has to be more deliberate, not less.
Strength and power are not the same thing. Imagine being able to squat 400+ lbs, but can't broad jump 2 feet? Strength is how much force you can produce. Power is how fast you can produce it. In the literature, power declines roughly 3 to 3.5 percent per year in older adults, compared to 1.5 to 2 percent for strength. It's power that determines whether you catch yourself from a fall. Falls kill a lot of people over 65. While hypertrophy training remains important, you also need to dial up your power training.
The fix is resistance training with intent. Move the load at a constant speed during the concentric phase. This trains the neuromuscular system to rapidly recruit motor units, which is the component that deteriorates fastest. Most people over 50 are missing this from their programs entirely. Maintaining our neuromuscular adaptations in a robust state is a key component of master's athlete training.
Most training programs move in one direction: forward. Life doesn't. Falls and life's physical stressors happen laterally or in rotation. Injuries happen with unexpected rotation. Reaching, twisting, catching yourself on an uneven surface. These are the movement qualities that decline fastest because almost nobody trains them deliberately after 40.
Lateral hops, rotational medicine ball work, agility drills scaled to your ability, and single-leg stance with perturbation. These aren't "extras" for athletes. They're the movements that keep you functional in the real world, where physical stress almost always includes a rotational or lateral component. Train the way life actually loads you.
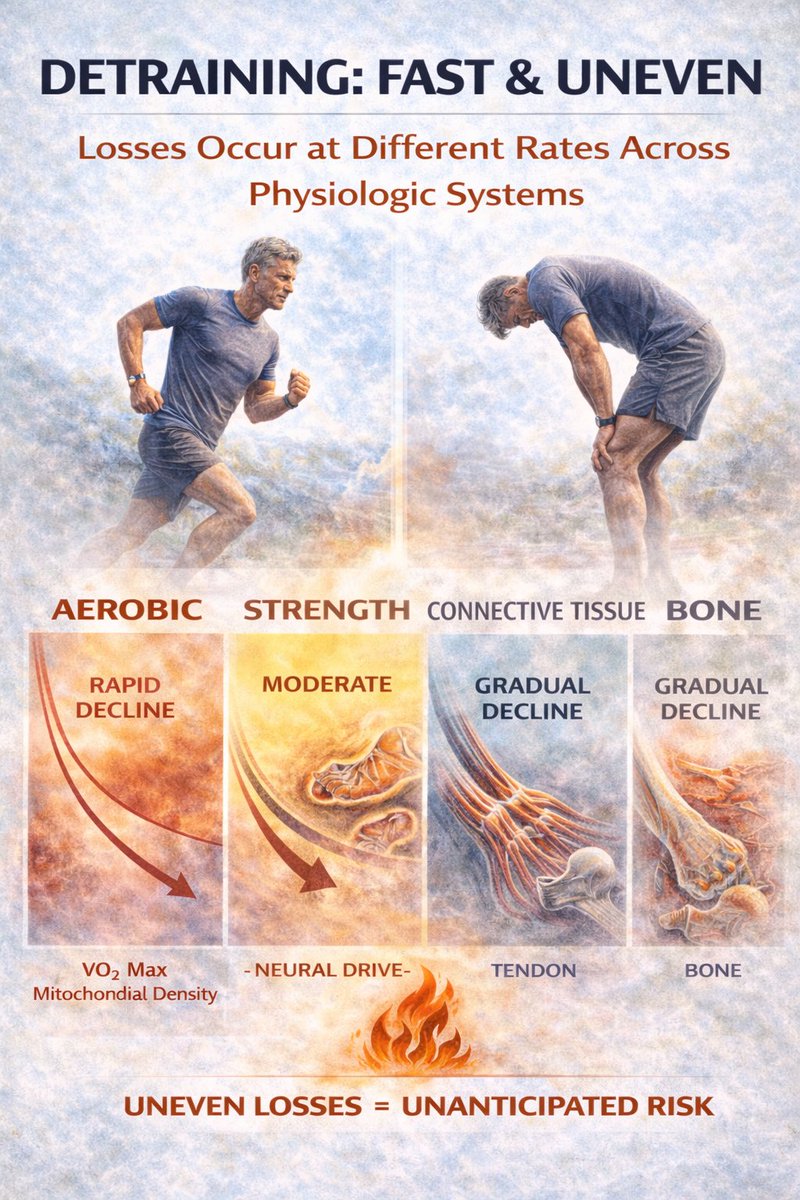
Aerobic fitness is the foundation for everything else built on it. VO2max declines roughly 10 percent per decade after 30 without deliberate training, and it's one of the strongest predictors of all-cause mortality we have. I now use my bike for volume rather than running more.
It builds and maintains my aerobic base without the joint stress and recovery burden that running at higher mileage entails. That frees up recovery capacity for the heavy lifting, the impact work, and the rotational training that cycling can't provide. The bike isn't the whole program... but it's a great way to get your volume in.
It builds and maintains my aerobic base without the joint stress and recovery burden that running at higher mileage entails. That frees up recovery capacity for the heavy lifting, the impact work, and the rotational training that cycling can't provide. The bike isn't the whole program... but it's a great way to get your volume in.
Bone density peaks in the late 20s and declines steadily after that, faster in women post-menopause, but it affects men too. Running provides some stimulus, but not enough for the spine and hip. Cycling provides almost none. The systematic reviews are consistent on this. Heavy resistance training and impact loading are the most effective tools we have for bone.
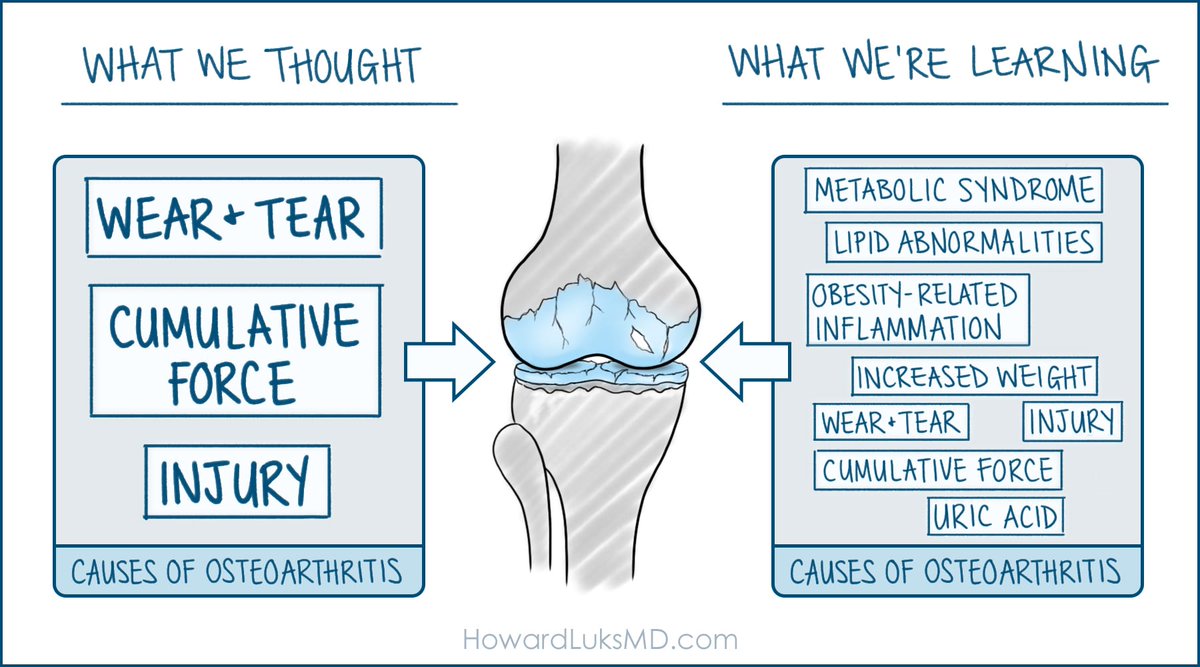
I see this constantly in the clinic. Someone stops moving because their MRI looks alarming. Meniscus tears, cartilage thinning, labral fraying. In imaging studies of pain-free adults, a very large percentage of knees show abnormalities on MRI. 69 percent of asymptomatic hips have labral tears. The scan and the symptoms often don't match. I've seen far too many imaging studies ruin a master's athlete's training program.
The decision to treat should be driven by what you can and can't do functionally, not by what the scan shows. I've watched too many people bench themselves because of a radiology report, not because of their actual capacity.
Training stress is only half of the equation. Adaptation, stronger muscles, denser bones, and better cardiovascular capacity occur during recovery.
After 50, recovery takes longer and requires more deliberate attention: sleep quality, protein timing, and scheduled rest days. Ignoring this is how people overtrain without realizing it. This will creep up on you slowly and imperceptibly... you'll probably think you need to push harder... then you're going to break.
After 50, recovery takes longer and requires more deliberate attention: sleep quality, protein timing, and scheduled rest days. Ignoring this is how people overtrain without realizing it. This will creep up on you slowly and imperceptibly... you'll probably think you need to push harder... then you're going to break.
I know... I'm tired of this topic, too. But... Protein requirements increase with age, not decrease. Older muscle is less responsive to the anabolic stimulus of a given dose of protein, so you need more to trigger the same synthetic response. The PROT-AGE group and ESPEN both recommend 1.2 to 1.6 g/kg/day for active older adults, which works out to roughly 0.6 to 0.7g per pound of body weight.
None of this is complicated, but it requires consistency measured in years. Strength, power, bone density, joint health, recovery, and protein. Each one is manageable. The physiology is on your side if you work with it rather than assuming the decline is inevitable.
I wrote up a 30+ page guide on this subject and published it here... hjluks.gumroad.com/l/oxpwg
• • •
Missing some Tweet in this thread? You can try to
force a refresh