Orthopedic Surgeon, author, trail runner, very amateur cyclist. Exits x 3. Join 20,000 + subscribers on Substack.
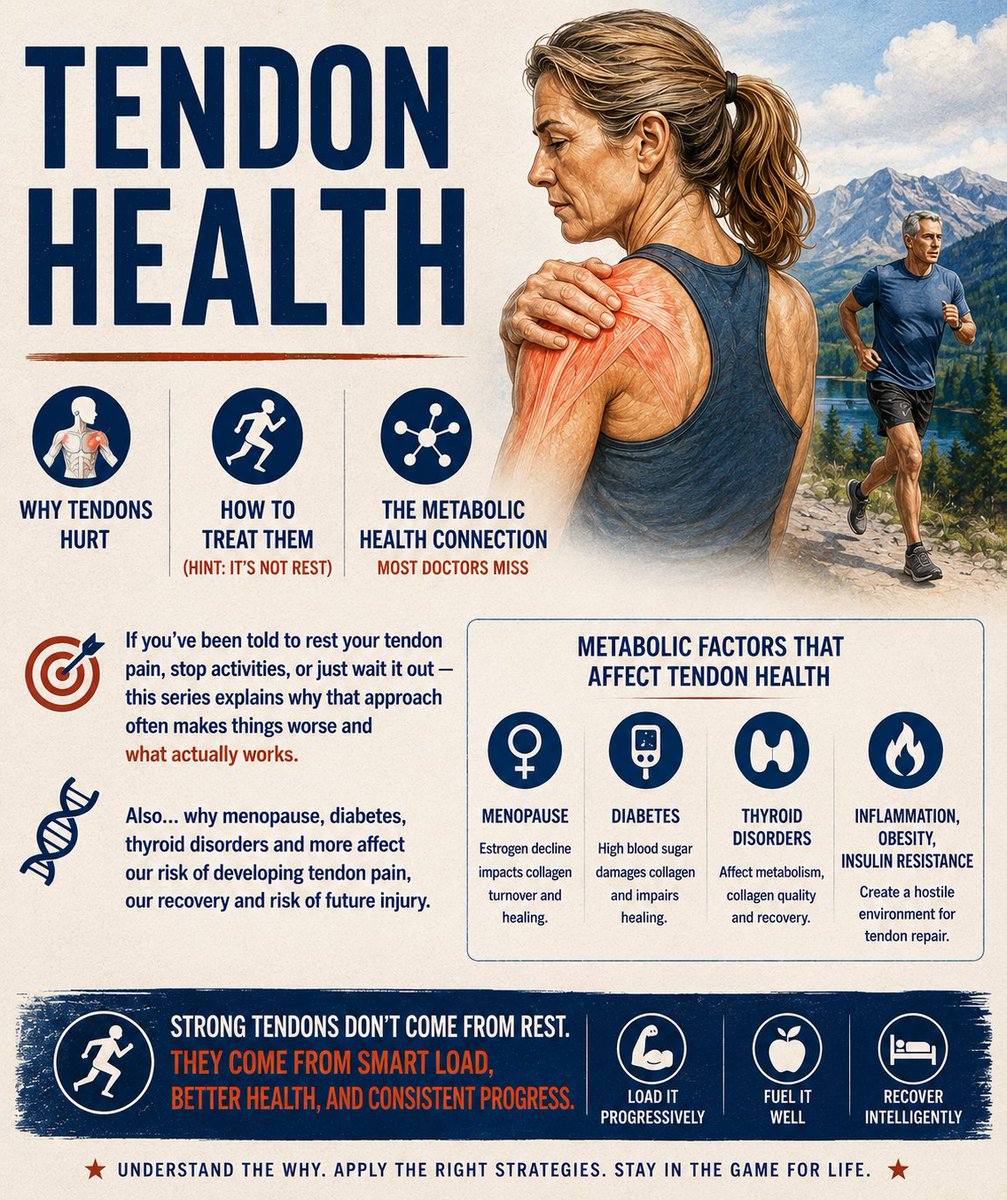 Most tendon pain is not caused by a single traumatic event. Tendinopathy is the most common cause of tendon pain. It is a failed response to loading over time. Simply put... Your tendon was asked to do more than it was adapted to handle, and the rate of breakdown exceeded the rate of repair.
Most tendon pain is not caused by a single traumatic event. Tendinopathy is the most common cause of tendon pain. It is a failed response to loading over time. Simply put... Your tendon was asked to do more than it was adapted to handle, and the rate of breakdown exceeded the rate of repair. 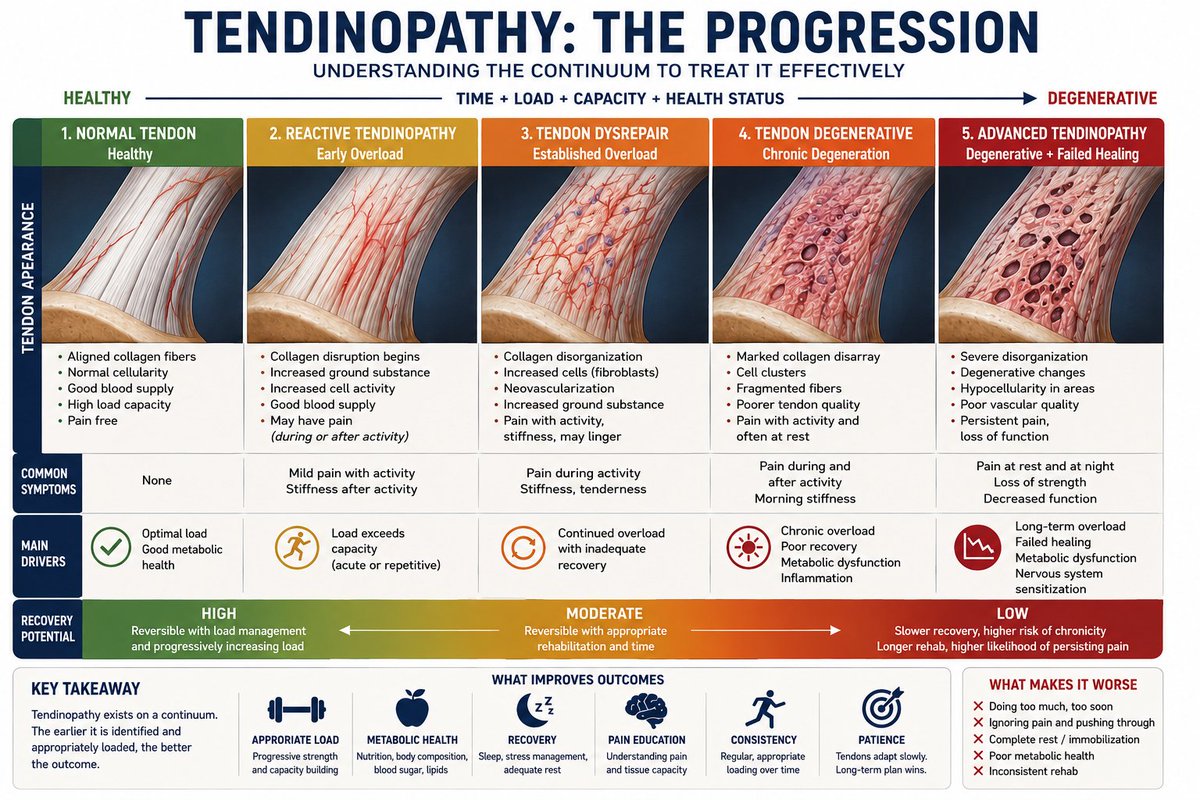
 Perimenopausal women are disproportionately affected, and we need to look at the receptor-level interactions.
Perimenopausal women are disproportionately affected, and we need to look at the receptor-level interactions. I have spent three decades across an exam room table from people who are trying to figure out why their body stopped being the thing they could count on.
I have spent three decades across an exam room table from people who are trying to figure out why their body stopped being the thing they could count on.
 2/
2/ 2/
2/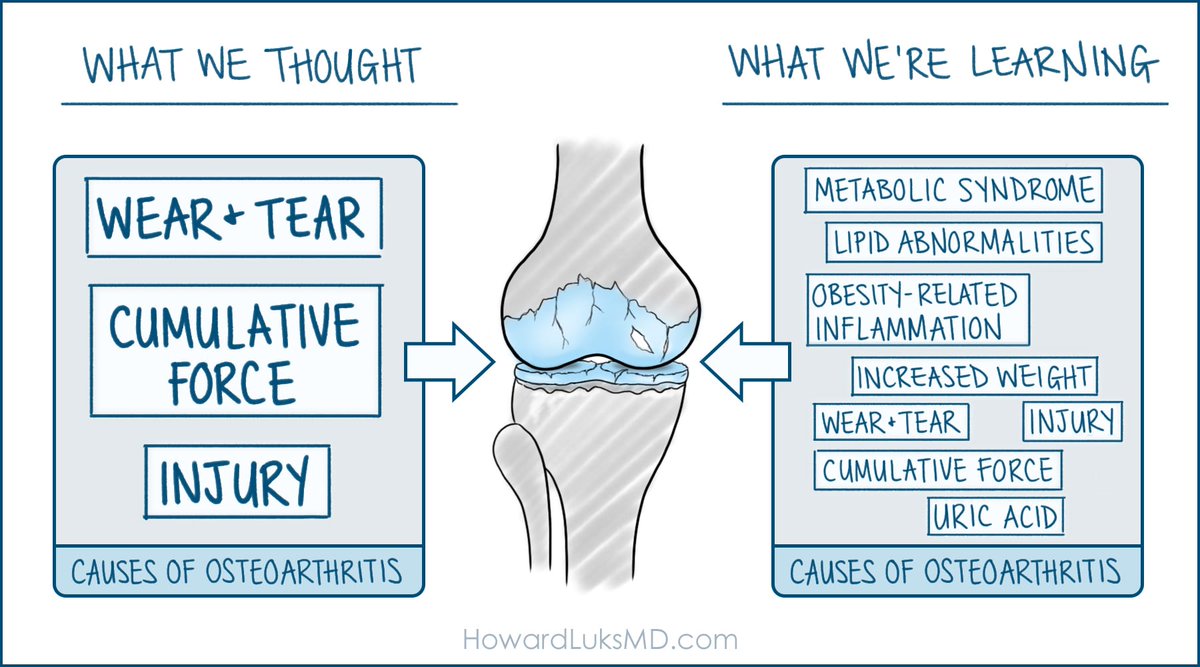 Here's a useful fact to set the stage for this discussion: Hand osteoarthritis is far more common in people with obesity.
Here's a useful fact to set the stage for this discussion: Hand osteoarthritis is far more common in people with obesity. 2/ Most returning athletes underestimate two things:
2/ Most returning athletes underestimate two things:
 Most people mismanage their diagnosis of knee arthritis. It's not their fault... They make wrong assumptions... and they narrow their lives further.
Most people mismanage their diagnosis of knee arthritis. It's not their fault... They make wrong assumptions... and they narrow their lives further.