
Dermatology is wrong about the sun.
And it's killing people.
I'm a dermatologist. 226 publications. I should know.
Avoiding the sun increases the risk of dying as much as being a smoker.
We can fix it.
For decades, dermatology's message has been simple: avoid the sun. Wear sunscreen. Seek shade. UV causes skin cancer. End of discussion.
That message is incomplete and outdated.
People are dying because of it. Lots of people.
The evidence has gotten strong enough that the field needs to update it.🧵
And it's killing people.
I'm a dermatologist. 226 publications. I should know.
Avoiding the sun increases the risk of dying as much as being a smoker.
We can fix it.
For decades, dermatology's message has been simple: avoid the sun. Wear sunscreen. Seek shade. UV causes skin cancer. End of discussion.
That message is incomplete and outdated.
People are dying because of it. Lots of people.
The evidence has gotten strong enough that the field needs to update it.🧵
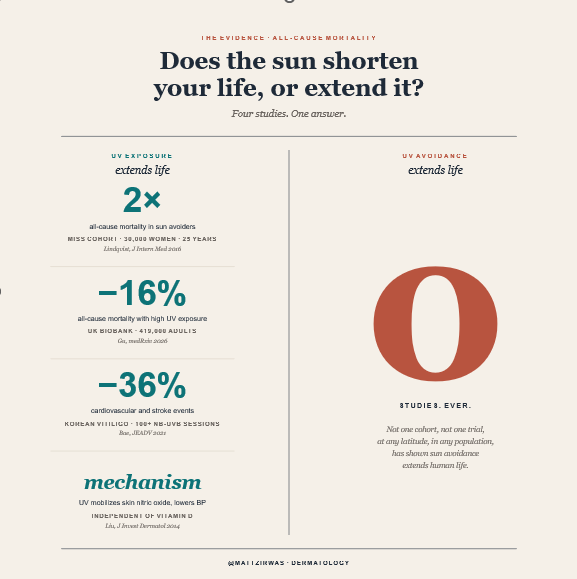
The Data
The MISS cohort followed over 29,500 Swedish women for 25 years.
Women who avoided the sun died at the same rate as smokers who got the most sun.
Read that again. Sun avoidance carried mortality risk comparable to smoking.
The effect was driven primarily by cardiovascular mortality.
Women with the lowest sun exposure had a 60% higher rate of cardiovascular death compared to those with the highest exposure.
The MISS cohort followed over 29,500 Swedish women for 25 years.
Women who avoided the sun died at the same rate as smokers who got the most sun.
Read that again. Sun avoidance carried mortality risk comparable to smoking.
The effect was driven primarily by cardiovascular mortality.
Women with the lowest sun exposure had a 60% higher rate of cardiovascular death compared to those with the highest exposure.
The UK Biobank confirmed it in about 400,000 participants.
Higher UV exposure was associated with 19% lower cardiovascular mortality, 12% lower cancer mortality, and 15% lower all-cause mortality.
But maybe sun-seekers are just healthier people?
More active, more outdoorsy, more likely to exercise?
Higher UV exposure was associated with 19% lower cardiovascular mortality, 12% lower cancer mortality, and 15% lower all-cause mortality.
But maybe sun-seekers are just healthier people?
More active, more outdoorsy, more likely to exercise?
A Korean study of over 12,000 vitiligo patients tightened the causal case.
Patients who received 100+ sessions of narrowband UVB phototherapy — sitting still in a light box in a clinic — had 36% fewer cardiovascular and cerebrovascular events.
This isn't perfect (adherence still correlates with health behaviors) but it strips out most of the "outdoor lifestyle" confounding that haunts cohort studies.
UV exposure itself appears to be doing real work.
And Korea is at about the same latitutude as California.
Patients who received 100+ sessions of narrowband UVB phototherapy — sitting still in a light box in a clinic — had 36% fewer cardiovascular and cerebrovascular events.
This isn't perfect (adherence still correlates with health behaviors) but it strips out most of the "outdoor lifestyle" confounding that haunts cohort studies.
UV exposure itself appears to be doing real work.
And Korea is at about the same latitutude as California.
The Mechanism
Your skin stores large reserves of nitrogen oxides — nitrate, nitrite, and S-nitrosothiols.
When UV hits your skin, it releases nitric oxide from these stores into your bloodstream.
Nitric oxide dilates your arteries.
Your blood pressure drops.
Your skin stores large reserves of nitrogen oxides — nitrate, nitrite, and S-nitrosothiols.
When UV hits your skin, it releases nitric oxide from these stores into your bloodstream.
Nitric oxide dilates your arteries.
Your blood pressure drops.
This happens independently of temperature. A study of 342,000 dialysis patients across 2,178 US clinics showed that UV radiation lowered blood pressure even after adjusting for outdoor temperature.
Hypertension is the leading cause of premature death and disability worldwide, responsible for 18% of all deaths globally.
Blood pressure correlates directly with latitude — how far you live from the equator, which directly determines how much UV your skin receives.
About 25% of the variance in population blood pressure is explained by latitude alone.
Blood pressure is 5-6 mmHg higher in winter than summer. That seasonal swing maps directly onto the 23% higher cardiovascular mortality in winter.
Hypertension is the leading cause of premature death and disability worldwide, responsible for 18% of all deaths globally.
Blood pressure correlates directly with latitude — how far you live from the equator, which directly determines how much UV your skin receives.
About 25% of the variance in population blood pressure is explained by latitude alone.
Blood pressure is 5-6 mmHg higher in winter than summer. That seasonal swing maps directly onto the 23% higher cardiovascular mortality in winter.
The Vitamin D Red Herring
People with higher vitamin D levels are healthier.
This is true.
But vitamin D is largely a marker of UV exposure, not the cause of the benefit.
If you have high vitamin D, it means you're getting UV.
The UV is what's helping you.
Not the vitamin D.
People with higher vitamin D levels are healthier.
This is true.
But vitamin D is largely a marker of UV exposure, not the cause of the benefit.
If you have high vitamin D, it means you're getting UV.
The UV is what's helping you.
Not the vitamin D.
The two largest randomized controlled trials of vitamin D supplementation — VITAL (25,000+ participants) and ViDA (5,000+ participants) — both found no reduction in cardiovascular disease or cancer.
A New England Journal of Medicine editorial in 2022 concluded the general population should stop taking vitamin D supplements.
Vitamin D supplements have minimal health benefit if you're not at risk for osteoporosis.
Dermatology's official position is still: avoid the sun, take vitamin D.
The first half increases your cardiovascular risk.
The second half doesn't fix it.
A New England Journal of Medicine editorial in 2022 concluded the general population should stop taking vitamin D supplements.
Vitamin D supplements have minimal health benefit if you're not at risk for osteoporosis.
Dermatology's official position is still: avoid the sun, take vitamin D.
The first half increases your cardiovascular risk.
The second half doesn't fix it.
"Where's The RCT?"
Here's the part nobody talks about: the gold-standard study can't be done.
You can't blind UV exposure.
You could randomize people to a recommendation — "get regular sun exposure" vs. "avoid the sun strictly" — but everyone knows what arm they're in. Adherence will be partial and uneven.
The sun-exposure group will see dermatologists more often and catch skin cancers earlier (surveillance bias).
The avoidance group may compensate with statins, BP meds, exercise... Whatever effect exists gets attenuated.
This is the same evidentiary problem as smoking and lung cancer — never RCT'd. Dietary sodium and blood pressure — weak RCT data, recommendations made anyway. Seatbelts and mortality — never RCT'd.
Public health has always relied on Bradford Hill criteria when randomization is structurally impossible.
Here's the part nobody talks about: the gold-standard study can't be done.
You can't blind UV exposure.
You could randomize people to a recommendation — "get regular sun exposure" vs. "avoid the sun strictly" — but everyone knows what arm they're in. Adherence will be partial and uneven.
The sun-exposure group will see dermatologists more often and catch skin cancers earlier (surveillance bias).
The avoidance group may compensate with statins, BP meds, exercise... Whatever effect exists gets attenuated.
This is the same evidentiary problem as smoking and lung cancer — never RCT'd. Dietary sodium and blood pressure — weak RCT data, recommendations made anyway. Seatbelts and mortality — never RCT'd.
Public health has always relied on Bradford Hill criteria when randomization is structurally impossible.
Run those on UV and cardiovascular mortality: Strength, consistency, dose-response, mechanism, coherence, temporality.
That's most of Bradford Hill cleared.
This is approximately the ceiling of evidence that can ever exist for this question.
Demanding RCT-level certainty for a question that can't be put in an RCT is a way of never updating.
We could do a RCT with NBUVB. I'm in favor of that. It'd be expensive, take years. We should start now.
But the sun is free and available now.
That's most of Bradford Hill cleared.
This is approximately the ceiling of evidence that can ever exist for this question.
Demanding RCT-level certainty for a question that can't be put in an RCT is a way of never updating.
We could do a RCT with NBUVB. I'm in favor of that. It'd be expensive, take years. We should start now.
But the sun is free and available now.
The Math
Cardiovascular disease kills about 700,000 Americans per year.
If optimizing UV exposure reduced cardiovascular deaths by even 20% — well below what the cohort hazard ratios would predict — that's 140,000 lives per year.
Take the most unrealistic, best-case scenario for sun avoidance. Imagine — impossibly — that completely eliminating UV exposure prevented every single skin cancer death. Melanoma, squamous cell, basal cell, all of it.
That's about 15,000 deaths per year.
140,000 vs 15,000.
Even granting sun avoidance impossibly optimistic benefits and lowballing what sun exposure does, the asymmetry is enormous.
And the real-world numbers are likely more lopsided — outdoor workers have no increased melanoma risk compared to indoor workers, and most melanoma risk comes from intermittent overexposure, not consistent moderate exposure.
Cardiovascular disease kills about 700,000 Americans per year.
If optimizing UV exposure reduced cardiovascular deaths by even 20% — well below what the cohort hazard ratios would predict — that's 140,000 lives per year.
Take the most unrealistic, best-case scenario for sun avoidance. Imagine — impossibly — that completely eliminating UV exposure prevented every single skin cancer death. Melanoma, squamous cell, basal cell, all of it.
That's about 15,000 deaths per year.
140,000 vs 15,000.
Even granting sun avoidance impossibly optimistic benefits and lowballing what sun exposure does, the asymmetry is enormous.
And the real-world numbers are likely more lopsided — outdoor workers have no increased melanoma risk compared to indoor workers, and most melanoma risk comes from intermittent overexposure, not consistent moderate exposure.
Why Hasn't This Changed Anything?
First, the good reason.
Every dermatologist has seen patients die of melanoma. We see it and it hurts and we feel like we can do something about it.
What dermatologists don't see is that they've had even more patients die of heart attacks and strokes, and if they do see it they don't know they might have been part of the cause.
Dermatologists are supposed to be the sun experts. What we say is what goes. So if we say "sun is bad," the house of medicine listens. It shouldn't.
Now for the bad reason.
Nobody has figured out how to make money off sunlight. There's no drug to sell. No program to push. No device to patent. No supplement to market. The intervention is free and available to everyone.
So no health guru or influencer has any reason to talk about it. With nobody talking about it, guidelines don't change.
First, the good reason.
Every dermatologist has seen patients die of melanoma. We see it and it hurts and we feel like we can do something about it.
What dermatologists don't see is that they've had even more patients die of heart attacks and strokes, and if they do see it they don't know they might have been part of the cause.
Dermatologists are supposed to be the sun experts. What we say is what goes. So if we say "sun is bad," the house of medicine listens. It shouldn't.
Now for the bad reason.
Nobody has figured out how to make money off sunlight. There's no drug to sell. No program to push. No device to patent. No supplement to market. The intervention is free and available to everyone.
So no health guru or influencer has any reason to talk about it. With nobody talking about it, guidelines don't change.
What I Actually Tell My Patients
Get regular, moderate sun exposure. Don't burn. Don't avoid the sun like it's poison, because the best obtainable evidence says that's more dangerous than the sun itself.
I'm a dermatologist saying this.
But I don't make money treating skin cancer, wrinkles, or age spots. I only treat eczema and rashes. Going outside helps eczema. If this advice sticks, it hurts my business.
But maybe that's why I can see this in a way other dermatologists can't. I'm not biased from seeing skin cancer every day. I just see the evidence.
Posting this will hurt my standing with my colleagues.
I have every professional incentive to keep telling you to stay inside and wear SPF 50. I'll get blowback. Lots of blowback.
But I follow the evidence.
And the evidence is clear.
Dermatology is wrong.
Excessively avoiding the sun kills people.
It's time for a change.
Get regular, moderate sun exposure. Don't burn. Don't avoid the sun like it's poison, because the best obtainable evidence says that's more dangerous than the sun itself.
I'm a dermatologist saying this.
But I don't make money treating skin cancer, wrinkles, or age spots. I only treat eczema and rashes. Going outside helps eczema. If this advice sticks, it hurts my business.
But maybe that's why I can see this in a way other dermatologists can't. I'm not biased from seeing skin cancer every day. I just see the evidence.
Posting this will hurt my standing with my colleagues.
I have every professional incentive to keep telling you to stay inside and wear SPF 50. I'll get blowback. Lots of blowback.
But I follow the evidence.
And the evidence is clear.
Dermatology is wrong.
Excessively avoiding the sun kills people.
It's time for a change.
I’m paying to promote this thread.
Nothing to sell. Just think it matters, a lot.
Finally, this is not medical advice.
Every person is unique. Autoimmune disease, certain medications, family history, personal history… it all matters. I’m talking about population level evidence. The vast majority of people should be getting sun intentionally and thoughtfully. But I don’t know if you’re one of those people.
________________________________________
**References**
1. Lindqvist PG, et al. J Intern Med. 2016
2. Lindqvist PG, et al. J Intern Med. 2014
3. Stevenson AC, et al. Health Place. 2024
4. Gu J, et al. medRxiv. 2026
5. Bae JM, et al. J Eur Acad Dermatol Venereol. 2021
6. Liu D, et al. J Invest Dermatol. 2014
7. Weller RB. J Invest Dermatol. 2024
Nothing to sell. Just think it matters, a lot.
Finally, this is not medical advice.
Every person is unique. Autoimmune disease, certain medications, family history, personal history… it all matters. I’m talking about population level evidence. The vast majority of people should be getting sun intentionally and thoughtfully. But I don’t know if you’re one of those people.
________________________________________
**References**
1. Lindqvist PG, et al. J Intern Med. 2016
2. Lindqvist PG, et al. J Intern Med. 2014
3. Stevenson AC, et al. Health Place. 2024
4. Gu J, et al. medRxiv. 2026
5. Bae JM, et al. J Eur Acad Dermatol Venereol. 2021
6. Liu D, et al. J Invest Dermatol. 2014
7. Weller RB. J Invest Dermatol. 2024
Here are the Spotify and Apple Podcast links to a podcast episode we did last year with Dr. Richard Weller, a dermatologist in the UK who is literally the world expert on this.
He comes on around 16:30.
open.spotify.com/episode/0uLOp3…
podcasts.apple.com/us/podcast/lit…
He comes on around 16:30.
open.spotify.com/episode/0uLOp3…
podcasts.apple.com/us/podcast/lit…
I didn't realize there was a podcast out from Dr. Weller - the world expert on this topic - the guy who did the research and showed the mechanism.
https://x.com/WellerRichard/status/2000936163763425662?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh




