HANTAVIRUS OUTBREAK 🧵
Following the WHO press briefing, I wanted to compile a thread with the key points.
1/ ISOLATION OF PASSENGERS
Concerningly, it seems the WHO are NOT recommending to isolate cruise ship passengers (even high-risk contacts) UNLESS they develop symptoms.
Following the WHO press briefing, I wanted to compile a thread with the key points.
1/ ISOLATION OF PASSENGERS
Concerningly, it seems the WHO are NOT recommending to isolate cruise ship passengers (even high-risk contacts) UNLESS they develop symptoms.
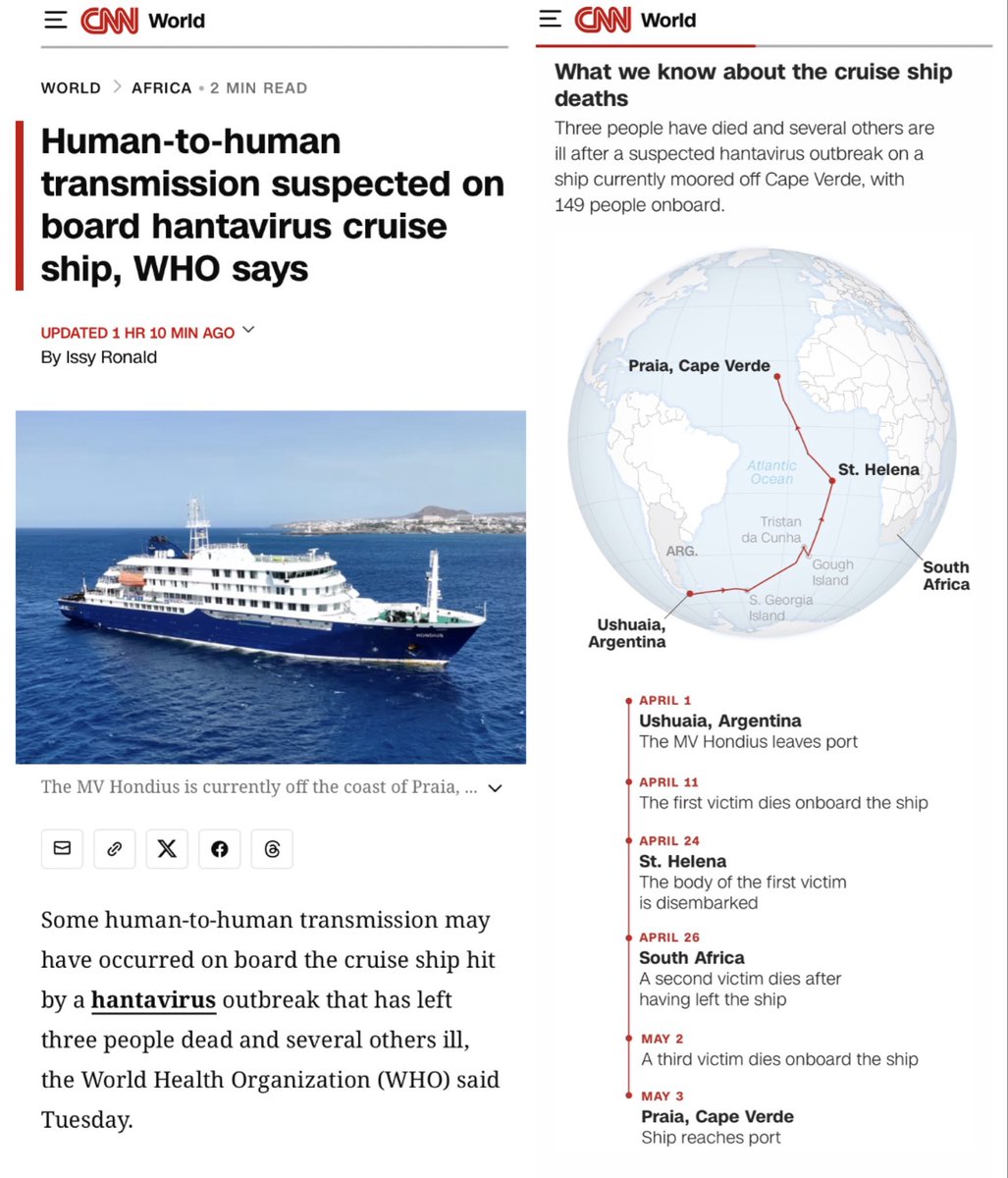
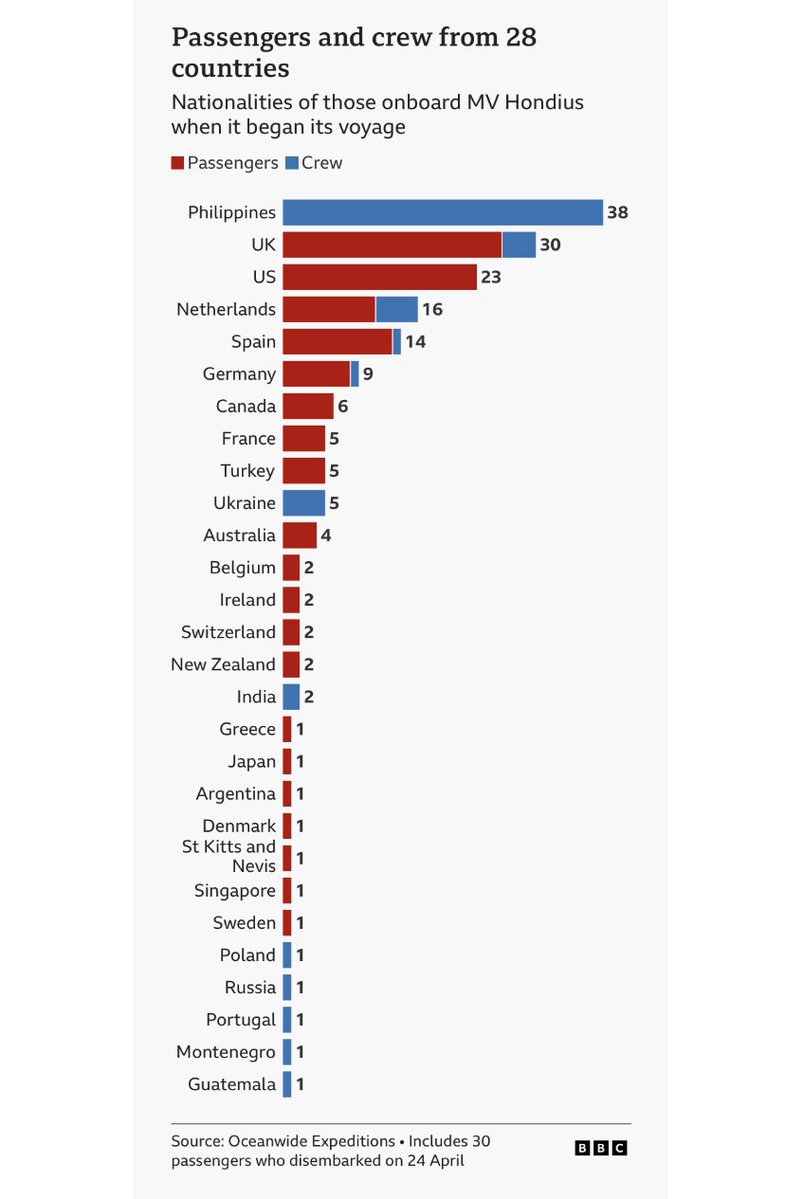
Just to quickly recap, it has been confirmed that the passengers & crew (including the 30 who disembarked on 24 April in St Helena) come from a total of 28 different countries.
The full breakdown of countries for both passengers 🟥 & crew 🟦 is detailed below ⬇️
The full breakdown of countries for both passengers 🟥 & crew 🟦 is detailed below ⬇️
When the 146 people remaining on the ship are repatriated to their home countries, each country will adopt their own local protocols.
However, the WHO are only recommending:
▪️SYMPTOMATIC cases ➡️ isolation
▪️ASYMPTOMATIC cases ➡️ monitoring
However, the WHO are only recommending:
▪️SYMPTOMATIC cases ➡️ isolation
▪️ASYMPTOMATIC cases ➡️ monitoring
The WHO’s recommended approach of ONLY isolating symptomatic people (whilst monitoring asymptomatic people) relies entirely on one BIG assumption…
…namely that people are ONLY infectious AFTER the onset of symptoms.
But is this strategy supported by the evidence? 🤔
…namely that people are ONLY infectious AFTER the onset of symptoms.
But is this strategy supported by the evidence? 🤔
The International Hantavirus Society issued an important statement yesterday which brings this entire strategy into question.
They clarify that “the precise timing of infectiousness remains incompletely defined”.
Infected people MAY be infectious before clear symptoms develop.
They clarify that “the precise timing of infectiousness remains incompletely defined”.
Infected people MAY be infectious before clear symptoms develop.

You can read the full statement from the International Hantavirus Society and members of the international hantavirus research & clinical community at this link ⬇️
zenodo.org/records/200752…
zenodo.org/records/200752…

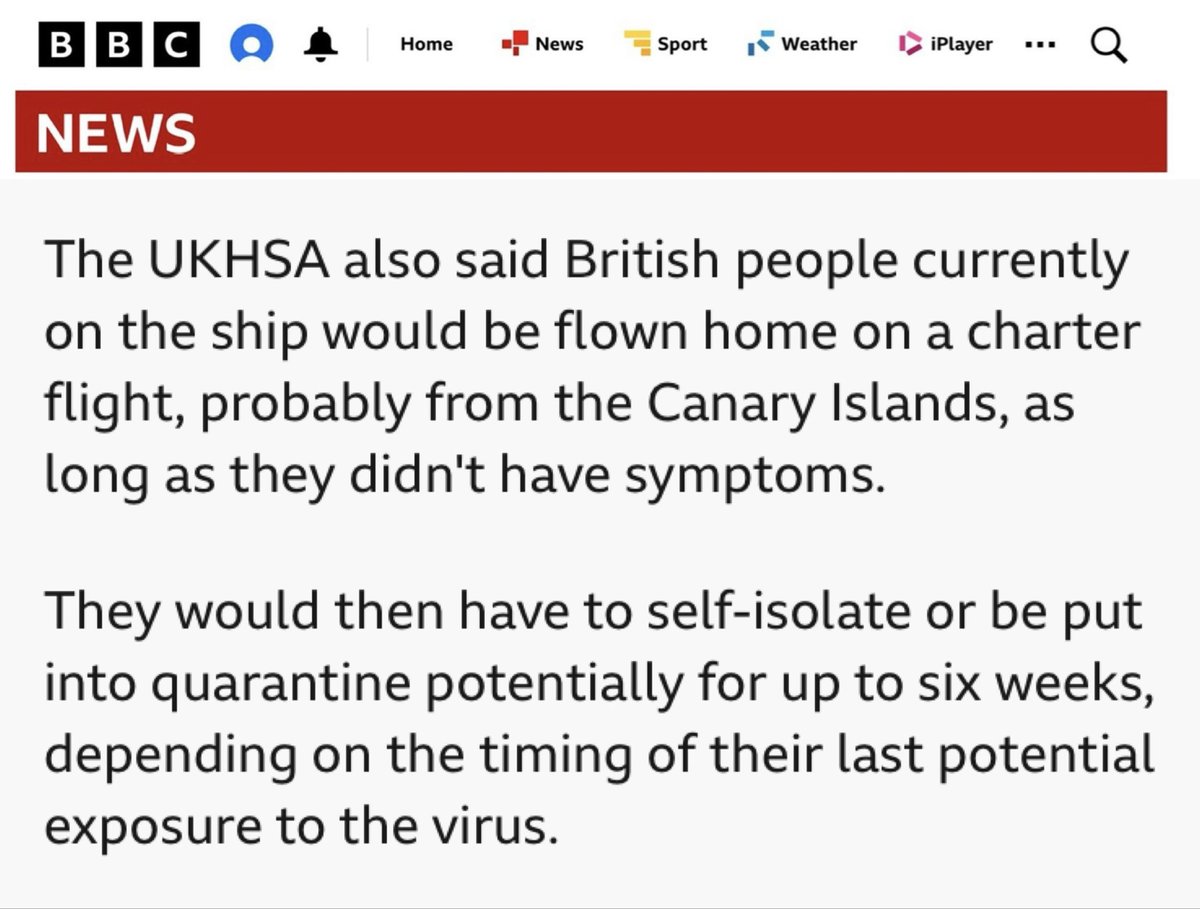
Thankfully some countries (like the UK & Spain) have confirmed that they are sensibly ignoring the WHO guidance and adopting a more cautious approach, asking ALL passengers departing the ship to self-isolate or quarantine for up to 6 weeks.
bbc.co.uk/news/live/cy59…
bbc.co.uk/news/live/cy59…
The US have also confirmed that the 17 Americans currently on the ship will be evacuated to a specialist quarantine facility in Nebraska upon repatriation to the US.
(Duration of quarantine is not yet confirmed).
cdc.gov/media/releases…
(Duration of quarantine is not yet confirmed).
cdc.gov/media/releases…
2/ MODES OF TRANSMISSION
Maria Van Kerkhove was clear that the Andes Virus is known to transmit from human-to-human.
She then went on to emphasise that transmission occurs “mainly among close contacts, either providing clinical care or people who’ve had close physical contact”.
Maria Van Kerkhove was clear that the Andes Virus is known to transmit from human-to-human.
She then went on to emphasise that transmission occurs “mainly among close contacts, either providing clinical care or people who’ve had close physical contact”.
This is nice & reassuring, but is it actually supported by the evidence?
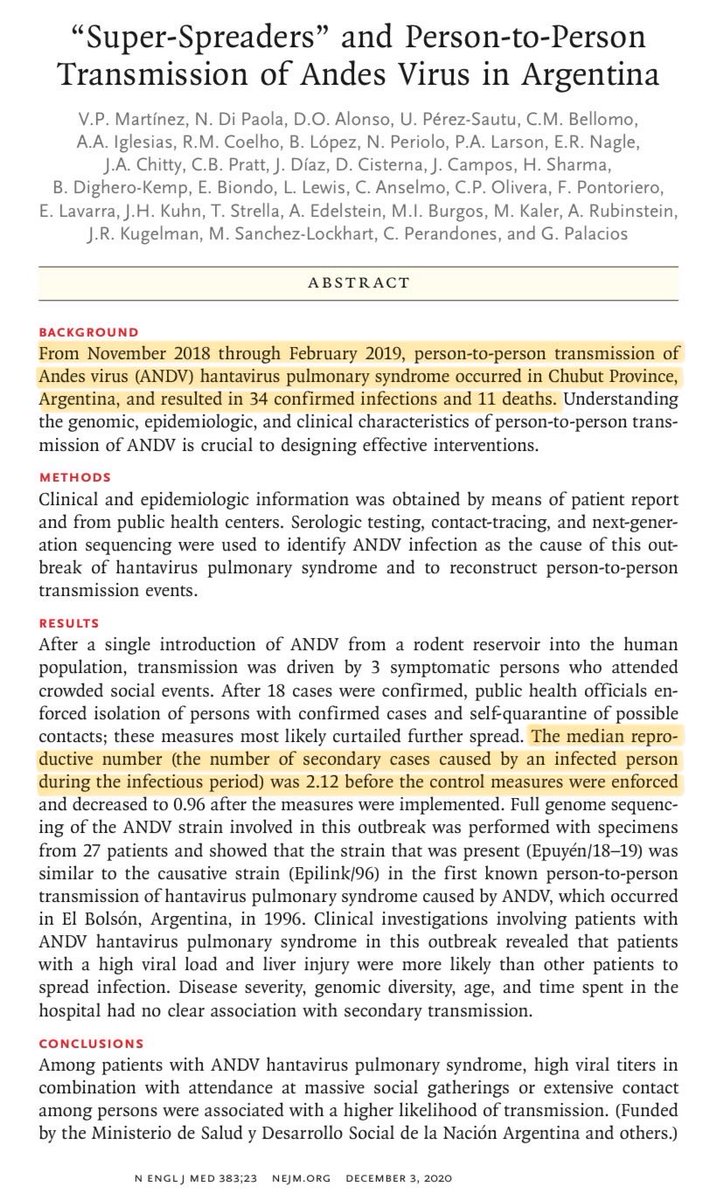
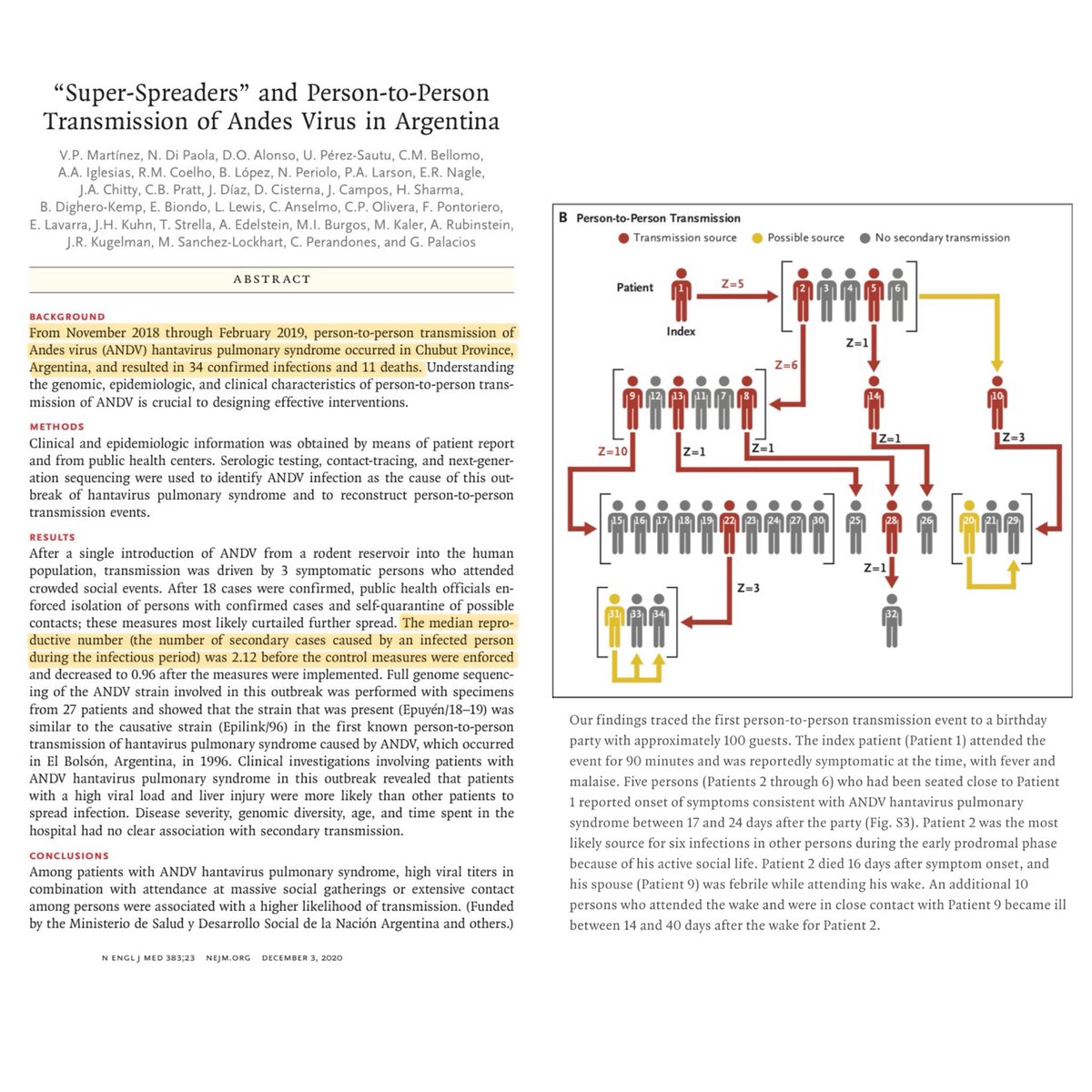
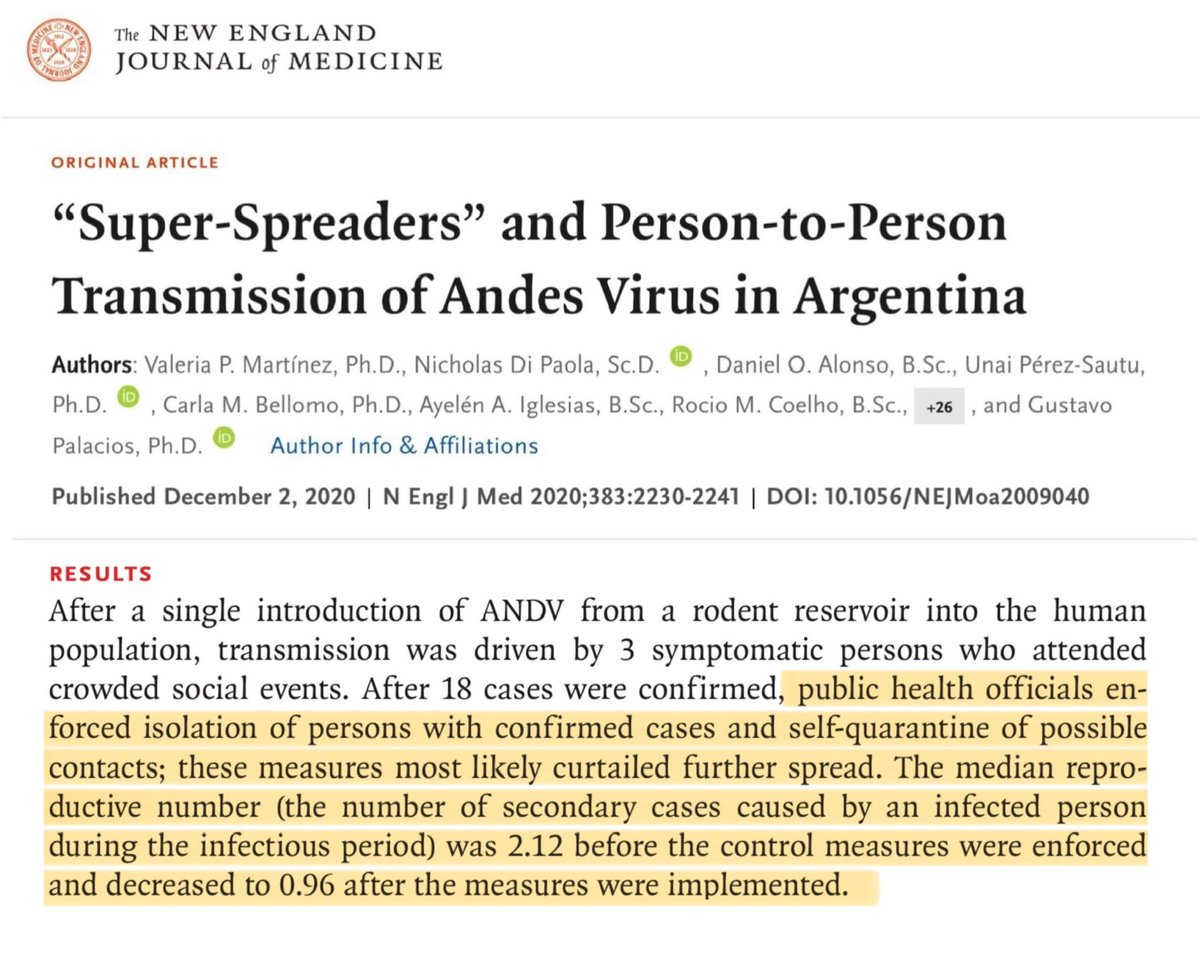
In 2018, there was a major Andes Virus outbreak in Argentina which led to 34 cases & 11 deaths.
The outbreak had an R0 of 2.1 before strict quarantine measures were enforced.
nejm.org/doi/full/10.10…
In 2018, there was a major Andes Virus outbreak in Argentina which led to 34 cases & 11 deaths.
The outbreak had an R0 of 2.1 before strict quarantine measures were enforced.
nejm.org/doi/full/10.10…
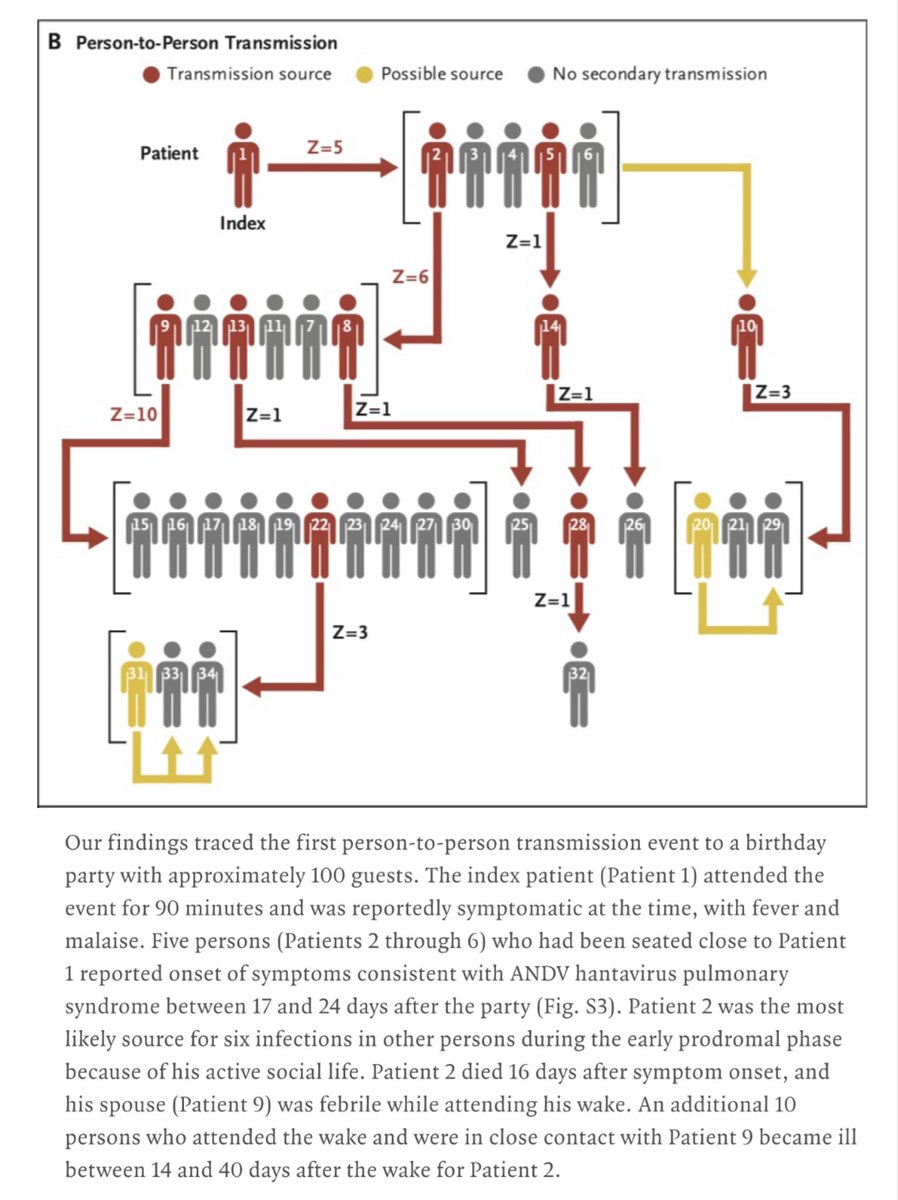
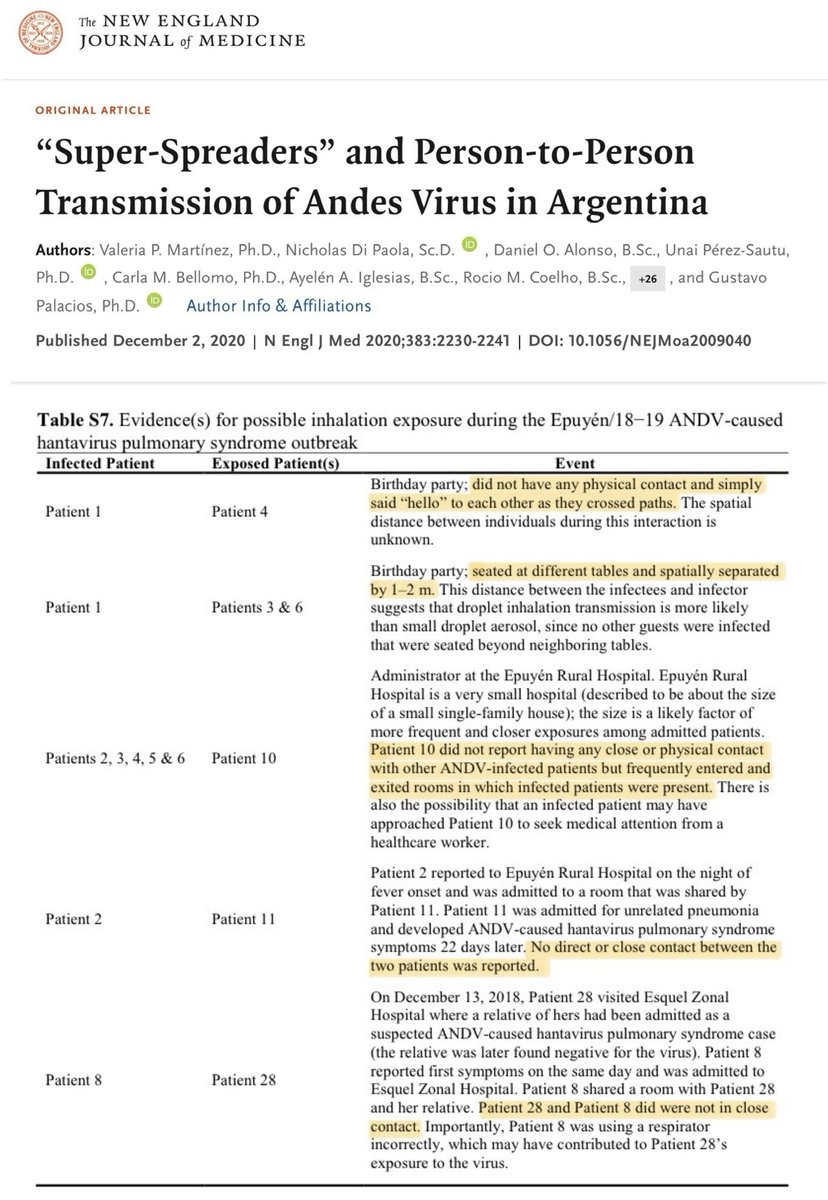
Importantly, detailed investigations into this Andes Virus outbreak in Argentina in 2018 clearly revealed that multiple transmissions had taken place WITHOUT CLOSE CONTACT.
The table below summarises the circumstances of these transmissions ⬇️
The table below summarises the circumstances of these transmissions ⬇️
The 2018 Andes Virus ‘Superspreader’ study also states that:
“On the basis of both the epidemiologic and genomic investigations of person-to-person transmission events, it appears that inhalation of droplets or *aerosolised virions* may have been the routes of infection.”
“On the basis of both the epidemiologic and genomic investigations of person-to-person transmission events, it appears that inhalation of droplets or *aerosolised virions* may have been the routes of infection.”

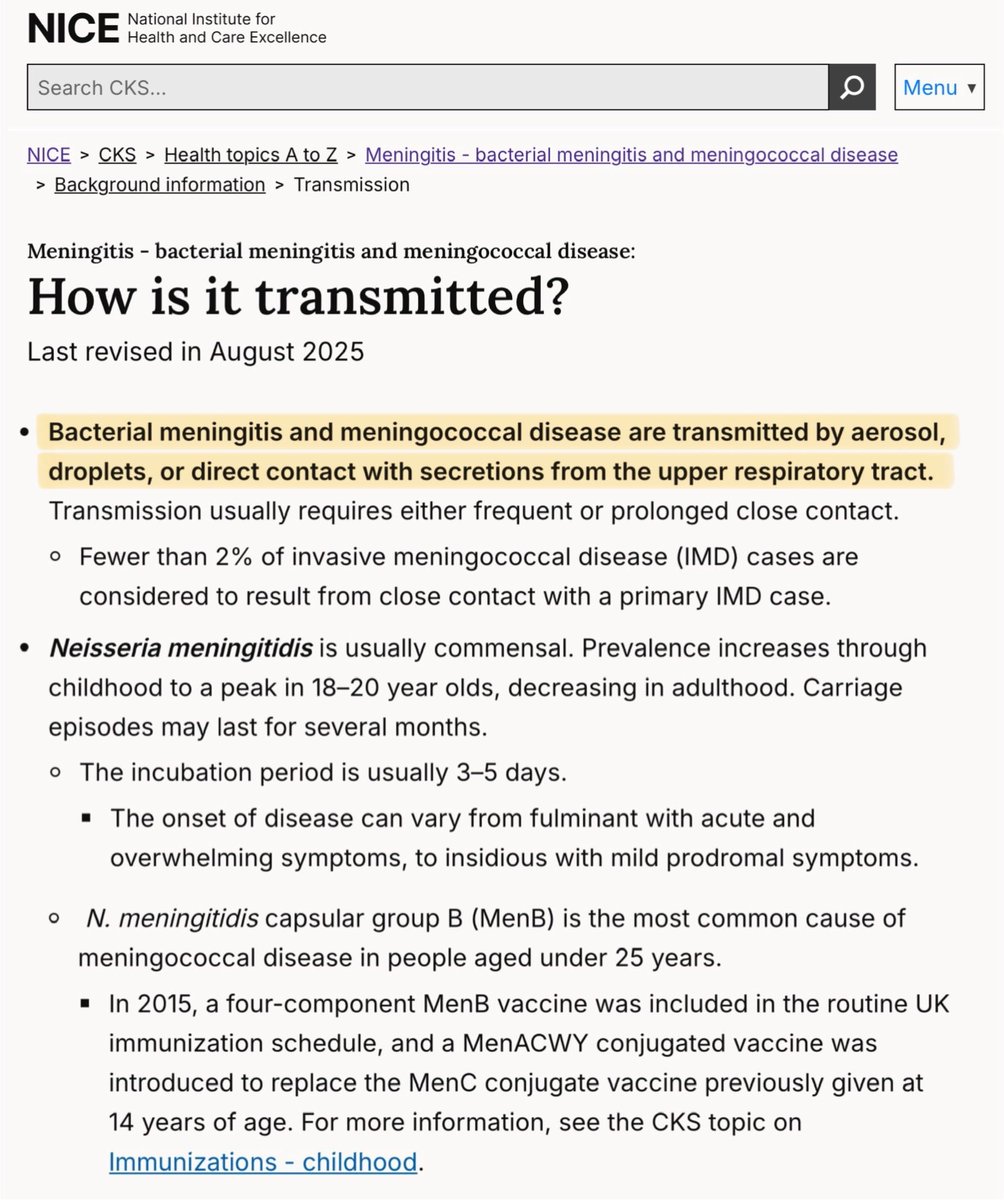
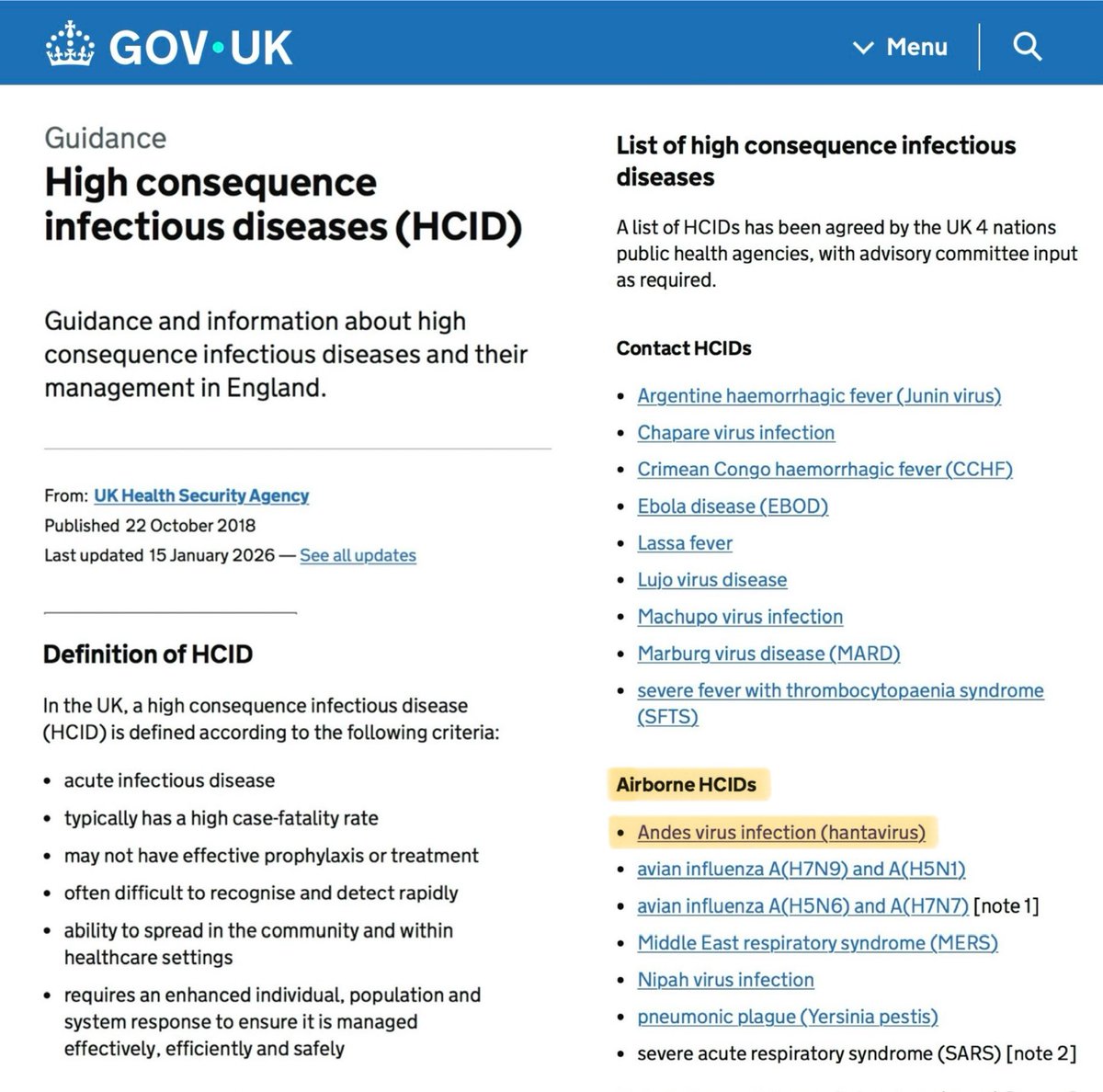
It’s also worth noting that the UK classify the Andes Virus (hantavirus) as an AIRBORNE High Consequence Infectious Disease (HCID).
Please note the key word there: AIRBORNE.
gov.uk/guidance/high-…
Please note the key word there: AIRBORNE.
gov.uk/guidance/high-…
However, despite all this readily available evidence that Andes Virus may well be airborne, María Van Kerkhove was on a calm-mongering mission.
Again & again, she confidently reassured listeners that the virus only spreads via “close intimate contact”.
“This is not SARS-CoV-2”
Again & again, she confidently reassured listeners that the virus only spreads via “close intimate contact”.
“This is not SARS-CoV-2”
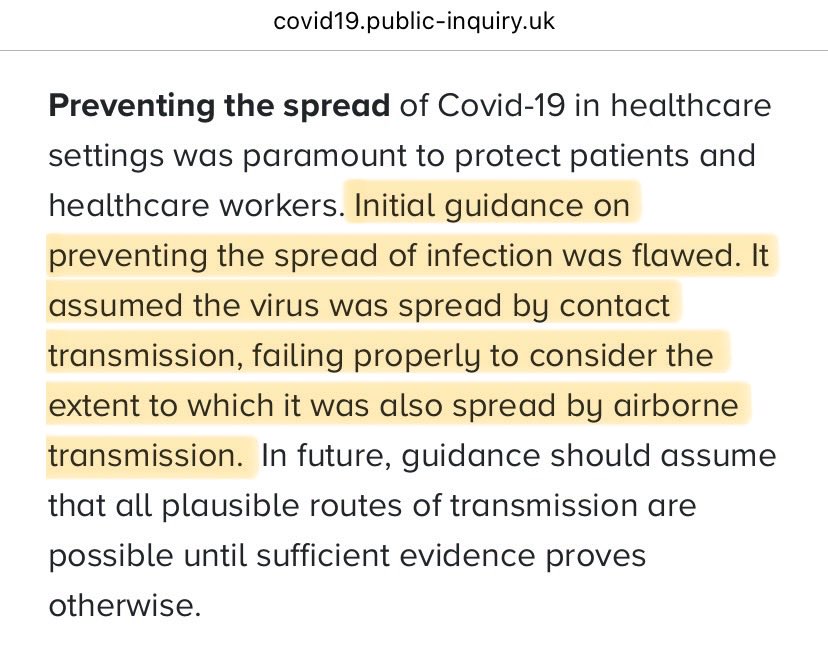
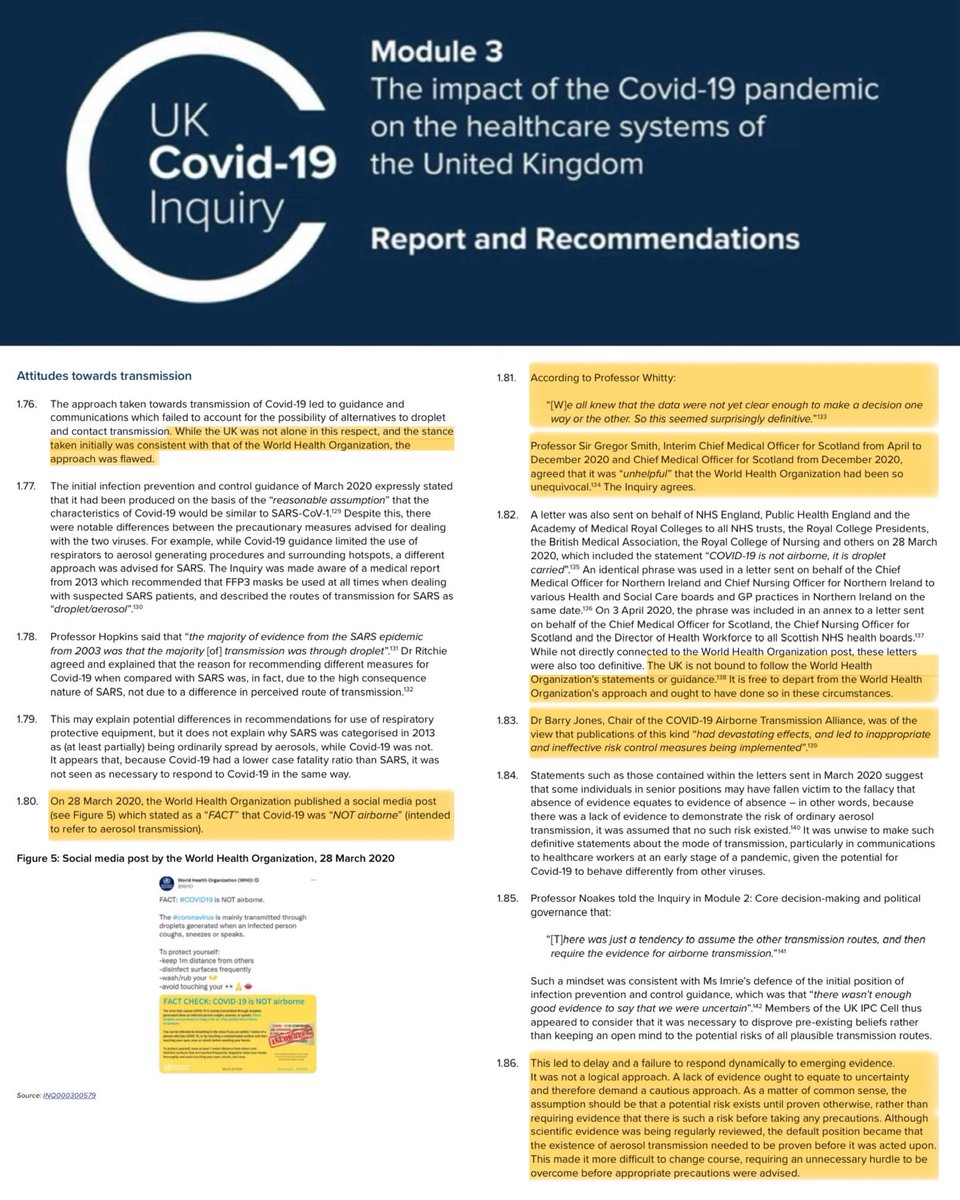
This feels suspiciously similar to March 2020 when, despite a lack of evidence, the WHO confidently stated that:
“COVID is NOT airborne”
The consequences of this flawed statement resulted in countless preventable deaths as countries failed to prioritise airborne mitigations.
“COVID is NOT airborne”
The consequences of this flawed statement resulted in countless preventable deaths as countries failed to prioritise airborne mitigations.
Interestingly, the ‘Superspreader’ study was mentioned during the WHO press conference.
They emphasised its similarities to the HV Hondius outbreak…
…but reassured that, since the 2018 outbreak only led to 34 cases, they “don’t anticipate a large epidemic” from this outbreak.
They emphasised its similarities to the HV Hondius outbreak…
…but reassured that, since the 2018 outbreak only led to 34 cases, they “don’t anticipate a large epidemic” from this outbreak.
However, the WHO neglected to mention that in 2018, Argentinian health authorities enforced quarantine measures for ALL high-risk contacts for at least 40 days, even if they had NO symptoms.
A total of 142 people were quarantined to prevent the spread.
gov.uk/guidance/andes…
A total of 142 people were quarantined to prevent the spread.
gov.uk/guidance/andes…

3/ ON-BOARD MITIGATIONS
Maria Van Kerkhove outlined the following precautions currently in place on the ship:
▪️disinfection of rooms
▪️confinement in cabins (including for eating meals)
▪️anyone leaving room to wear a medical (surgical) mask
However…
Maria Van Kerkhove outlined the following precautions currently in place on the ship:
▪️disinfection of rooms
▪️confinement in cabins (including for eating meals)
▪️anyone leaving room to wear a medical (surgical) mask
However…
…this list of precautions doesn’t tally with 1st-hand accounts from the ship.
Maria says passengers are eating meals in their cabins…
…but the NY Times suggests that:
“For meals, [passengers] are told to sit in every other chair in the dining room.”
nytimes.com/2026/05/06/wor…
Maria says passengers are eating meals in their cabins…
…but the NY Times suggests that:
“For meals, [passengers] are told to sit in every other chair in the dining room.”
nytimes.com/2026/05/06/wor…

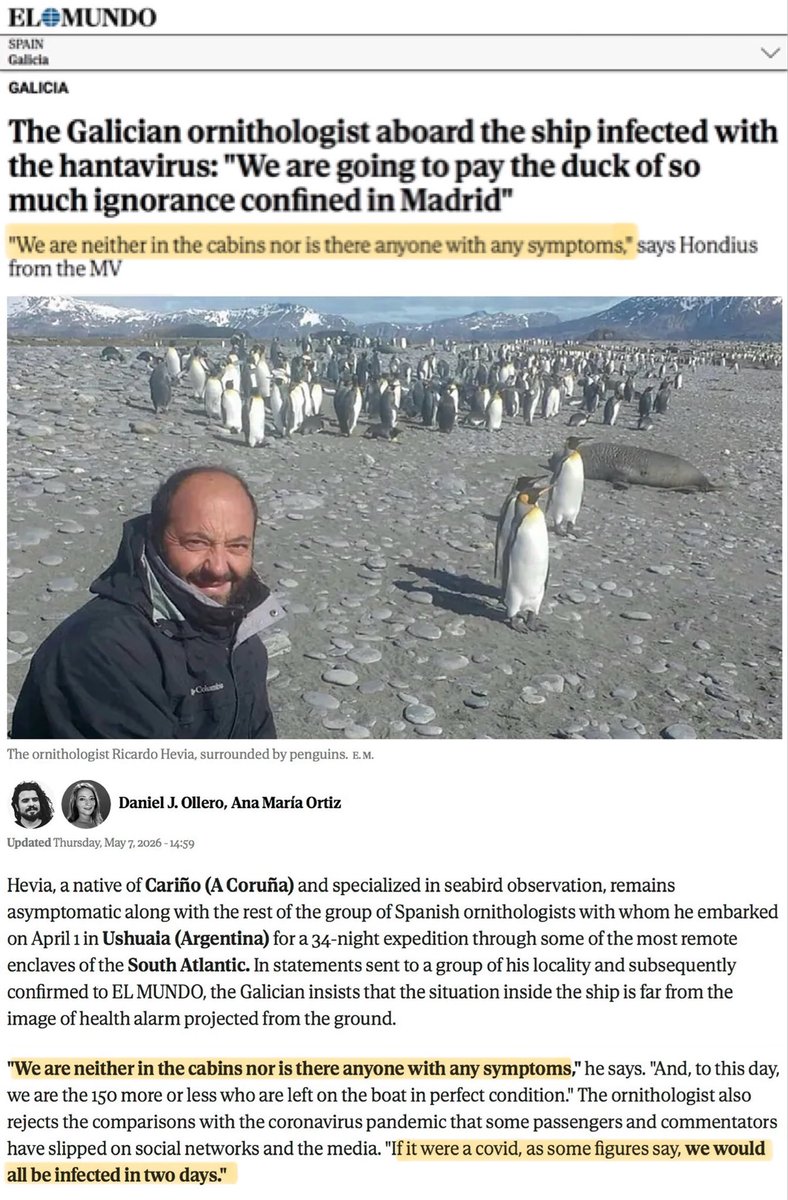
And this account, from an ornithologist on the ship, states:
“We are neither in the cabins nor is there anyone with symptoms.”
To further reinforce the laxness of measures, he goes on to say:
“If it were Covid […], we’d all be infected in two days.”
elmundo.es/galicia/2026/0…
“We are neither in the cabins nor is there anyone with symptoms.”
To further reinforce the laxness of measures, he goes on to say:
“If it were Covid […], we’d all be infected in two days.”
elmundo.es/galicia/2026/0…
But here’s the thing…
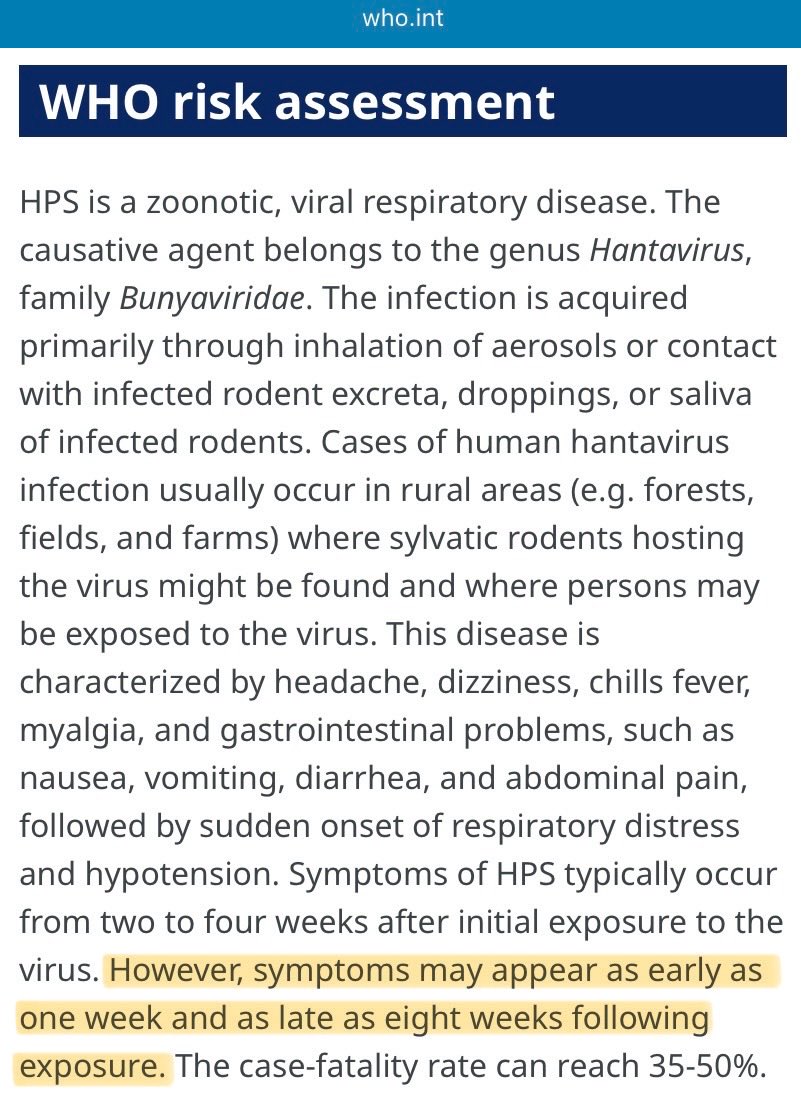
The Andes Virus has a LONG incubation period.
Symptoms can appear up to 8 WEEKS after exposure to an infectious case.
Initial symptoms are often mild & flu-like (prodromal stage) - and it’s MOST infectious during the early stage.
who.int/emergencies/di…
The Andes Virus has a LONG incubation period.
Symptoms can appear up to 8 WEEKS after exposure to an infectious case.
Initial symptoms are often mild & flu-like (prodromal stage) - and it’s MOST infectious during the early stage.
who.int/emergencies/di…
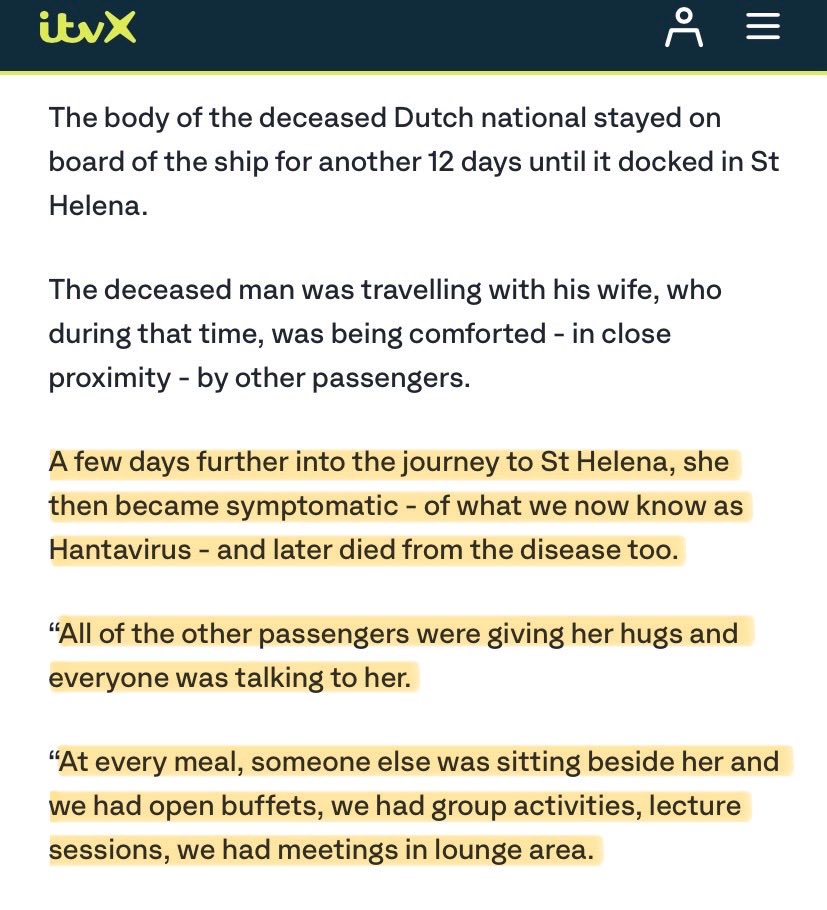
The infected Dutch woman was symptomatic & almost certainly infectious for several days before she disembarked from the ship on 24 April.
Anyone who came into contact with her may now be incubating the virus - BUT symptoms may not emerge until mid-JUNE!
itv.com/news/2026-05-0…
Anyone who came into contact with her may now be incubating the virus - BUT symptoms may not emerge until mid-JUNE!
itv.com/news/2026-05-0…
It’s also concerning that, despite the evidence that Andes Virus may be airborne (as per the ‘Superspreader’ paper mentioned earlier), the WHO have ONLY recommended use of medical (‘baggy blue’ surgical) masks, even when caring for symptomatic patients.
who.int/emergencies/di…
who.int/emergencies/di…
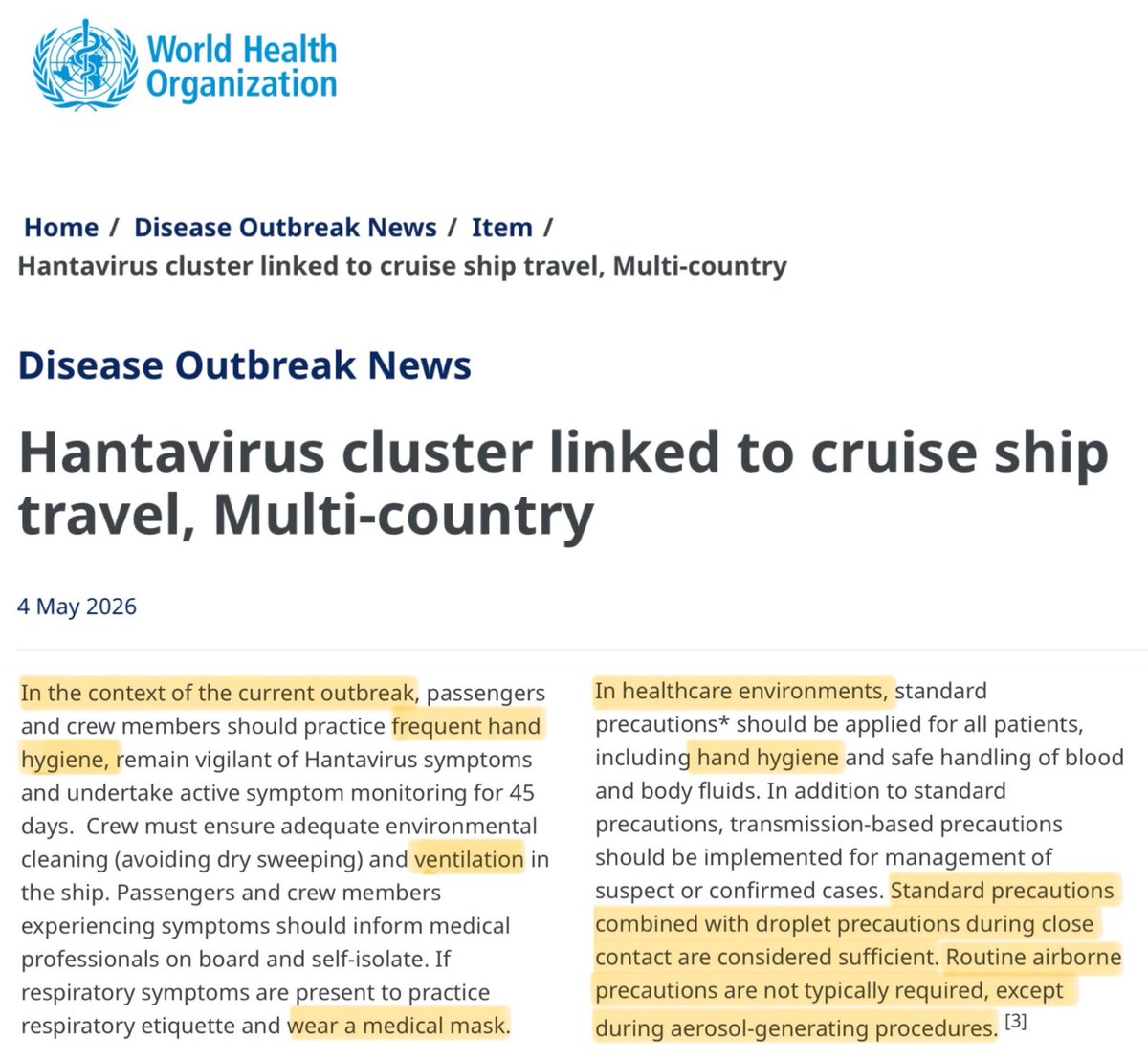
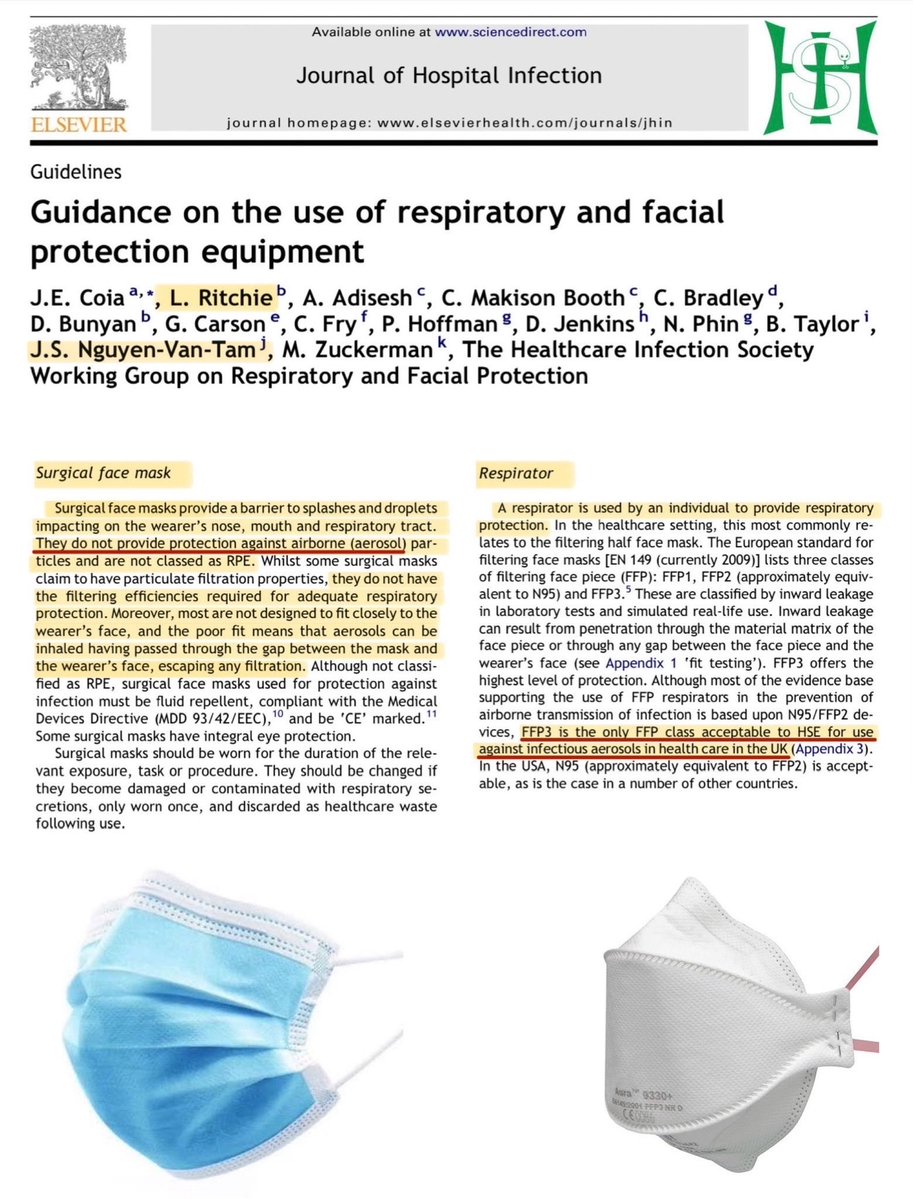
Surgical masks do NOT protect against airborne transmission.
Only respirator masks (N95/FFP3) provide adequate protection against airborne pathogens.
If there’s even a chance it could be airborne, surely the WHO should be recommending respirator masks?
journalofhospitalinfection.com/article/S0195-…
Only respirator masks (N95/FFP3) provide adequate protection against airborne pathogens.
If there’s even a chance it could be airborne, surely the WHO should be recommending respirator masks?
journalofhospitalinfection.com/article/S0195-…
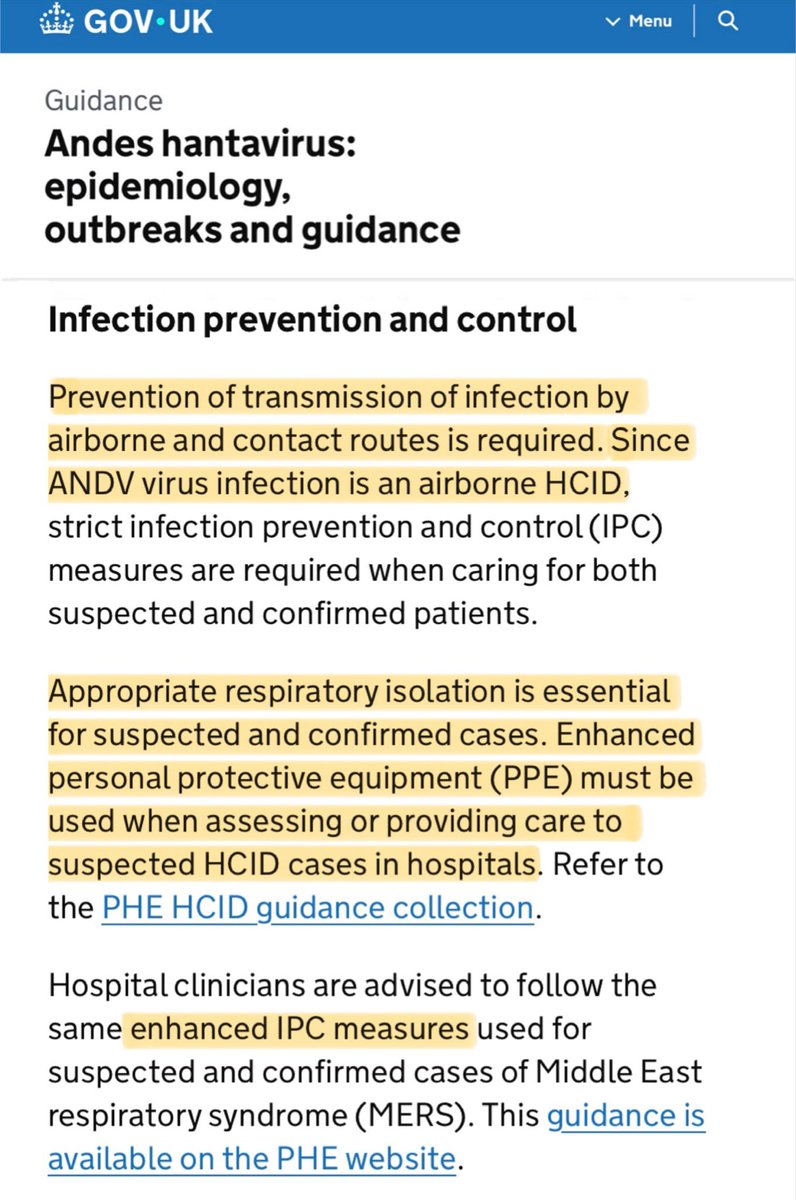
Here in the UK, infection control guidance when caring for patients with suspected or confirmed for Andes Virus requires:
▪️Prevention of transmission by AIRBORNE routes.
▪️Enhanced PPE (ie. FFP3 masks) when assessing or providing care in hospitals.
gov.uk/guidance/andes…
▪️Prevention of transmission by AIRBORNE routes.
▪️Enhanced PPE (ie. FFP3 masks) when assessing or providing care in hospitals.
gov.uk/guidance/andes…
4/ TESTING
The WHO confirmed that the hantavirus tests can only detect the viral RNA in a SYMPTOMATIC patient, from the first day of symptoms.
To clarify: this means someone infected will test NEGATIVE for the entire duration of the incubation period until onset of symptoms.
The WHO confirmed that the hantavirus tests can only detect the viral RNA in a SYMPTOMATIC patient, from the first day of symptoms.
To clarify: this means someone infected will test NEGATIVE for the entire duration of the incubation period until onset of symptoms.
This point is further reinforced by the statement issued yesterday from the International Hantavirus Society.
“A negative PCR result early after exposure should therefore NOT be interpreted as excluding later infection.”
Read full statement here:
zenodo.org/records/200752…
“A negative PCR result early after exposure should therefore NOT be interpreted as excluding later infection.”
Read full statement here:
zenodo.org/records/200752…
The CDC have also issued words of caution on the topic of testing, warning that:
“Early diagnosis of HPS can be difficult, especially within the first 72 hours of symptoms, before the virus can be accurately detected in body secretions & excretions.”
cdc.gov/han/php/notice…
“Early diagnosis of HPS can be difficult, especially within the first 72 hours of symptoms, before the virus can be accurately detected in body secretions & excretions.”
cdc.gov/han/php/notice…
A clear example of this issue of unreliable test results in the first few days of symptoms is the British man who is currently in hospital in Johannesburg:
▪️24 APR: Symptoms start
▪️27 APR: 1st test ➡️ NEGATIVE
▪️2 MAY: Repeat test ➡️ POSITIVE
edition.cnn.com/2026/05/08/hea…
▪️24 APR: Symptoms start
▪️27 APR: 1st test ➡️ NEGATIVE
▪️2 MAY: Repeat test ➡️ POSITIVE
edition.cnn.com/2026/05/08/hea…

With this in mind, I hope that suspected cases who test negative in the early stages of symptoms (when tests may be unreliable) continue to be isolated and undergo further testing.
This is the approach Singapore are taking ⬇️
reuters.com/business/healt…
This is the approach Singapore are taking ⬇️
reuters.com/business/healt…

5/ TRANSIT TO HOME COUNTRIES
One of the journalists specifically asked whether the cruise passengers would be allowed to take commercial flights home.
The answer seemed pretty vague & evasive.
Listen for yourself ⬇️
I suspect they can’t guarantee no commercial flights as yet.
One of the journalists specifically asked whether the cruise passengers would be allowed to take commercial flights home.
The answer seemed pretty vague & evasive.
Listen for yourself ⬇️
I suspect they can’t guarantee no commercial flights as yet.
New evidence has come to light this morning…
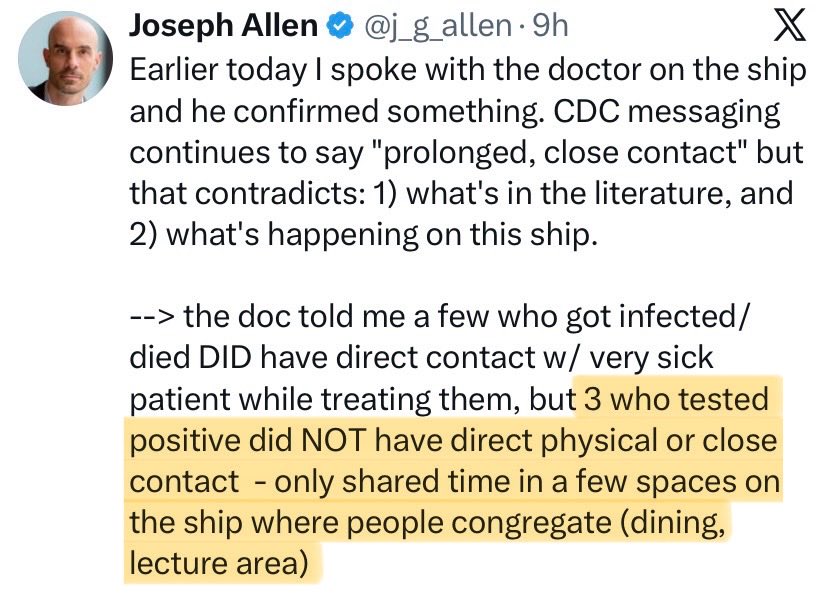
Prof Allen spoke to the ship’s current doctor (a passenger who stepped up after the original dr fell ill).
He confirmed that 3 people from the ship who tested positive did NOT have any physical or close contact with the index cases.
Prof Allen spoke to the ship’s current doctor (a passenger who stepped up after the original dr fell ill).
He confirmed that 3 people from the ship who tested positive did NOT have any physical or close contact with the index cases.
https://twitter.com/j_g_allen/status/2053224503245767144
CBC ‘Quirks & Quarks’ interviewed Gustavo Palacios, one of the world's few experts on the Andes virus, who was one of the authors of the Argentina ‘Superspreader’ study published in NEJM.
Here he summarises some of the key findings from that outbreak…
cbc.ca/listen/live-ra… x.com/sonyabuyting/s…
Here he summarises some of the key findings from that outbreak…
cbc.ca/listen/live-ra… x.com/sonyabuyting/s…
In that 2018 Argentina outbreak, one person was infected at the birthday party despite being seated on a table some distance away and only very briefly crossing paths with the infected person on the way to the restroom.
Transmission took place WITHOUT any close physical contact.
Transmission took place WITHOUT any close physical contact.
This is another crucial point from the 2018 Argentina outbreak which may have significant bearing on what unfolds in the coming days with the cruise ship outbreak…
“The window of infectiousness was 48 hours BEFORE the onset of symptoms and 48 hours AFTER the onset of symptoms.”
“The window of infectiousness was 48 hours BEFORE the onset of symptoms and 48 hours AFTER the onset of symptoms.”
Key lessons from 2018 Argentina outbreak:
🔎 probable AIRBORNE transmission
🔎 possibility of transmission from 48 hours BEFORE symptom onset
🔎 long incubation period, up to 8 weeks
🔎 containment strategy involved isolating ALL close contacts, regardless of symptoms.
🔎 probable AIRBORNE transmission
🔎 possibility of transmission from 48 hours BEFORE symptom onset
🔎 long incubation period, up to 8 weeks
🔎 containment strategy involved isolating ALL close contacts, regardless of symptoms.
The lesson from the Argentina outbreak is not panic but precaution.
Their containment strategy (rigorous contact-tracing, isolation of all possible contacts, & use of N95 masks) successfully reduced the estimated R0 from 2.1 to below 1 and brought the outbreak under control.
Their containment strategy (rigorous contact-tracing, isolation of all possible contacts, & use of N95 masks) successfully reduced the estimated R0 from 2.1 to below 1 and brought the outbreak under control.
What we need from health leaders is honesty not calm-mongering.
They must communicate clearly & truthfully about both the evidence & the unknowns.
This outbreak *should* be containable, but only if the guidance reflects the evidence rather than wishful thinking.
They must communicate clearly & truthfully about both the evidence & the unknowns.
This outbreak *should* be containable, but only if the guidance reflects the evidence rather than wishful thinking.
One last point: I suspect the wave of cases we’ve seen so far are from contact with case zero, the Dutch man who died on 11 Apr.
Given the incubation period is typically 2-6 weeks, we probably haven’t even seen the start of cases from those who came into contact with his wife…
Given the incubation period is typically 2-6 weeks, we probably haven’t even seen the start of cases from those who came into contact with his wife…
https://twitter.com/_catinthehat/status/2053079317156913642
Final final point…
This is a virus with a case fatality rate of 30-50% - ie. up to HALF of those who catch it will die…
…and there are NO vaccines or specific treatments.
If those leading the response get this wrong, the implications will be fatal.
ukhsa.blog.gov.uk/2026/05/05/wha…
This is a virus with a case fatality rate of 30-50% - ie. up to HALF of those who catch it will die…
…and there are NO vaccines or specific treatments.
If those leading the response get this wrong, the implications will be fatal.
ukhsa.blog.gov.uk/2026/05/05/wha…

🚨MAJOR UPDATE!
I’m delighted to say that the WHO have issued NEW guidance today in which every single concern I raised in this thread is addressed!
It’s brilliant that the WHO have listened to the international scientific community & changed course before it was too late… 👏🏻
I’m delighted to say that the WHO have issued NEW guidance today in which every single concern I raised in this thread is addressed!
It’s brilliant that the WHO have listened to the international scientific community & changed course before it was too late… 👏🏻
https://twitter.com/_catinthehat/status/2053566778664427671
• • •
Missing some Tweet in this thread? You can try to
force a refresh