The drug may start the addiction.
But over time, the cue can begin to drive it.
A place. A person. A smell. A mood. A time of day.
This is how the brain learns to seek the drug before the drug is even present. 🧵👇
But over time, the cue can begin to drive it.
A place. A person. A smell. A mood. A time of day.
This is how the brain learns to seek the drug before the drug is even present. 🧵👇
To understand why, start with what repeated drug use teaches the brain.
The substance is not experienced in isolation.
It happens in a context:
* where the person is
* who they are with
* what they feel
* what they expect
* what their body has learned to anticipate
The substance is not experienced in isolation.
It happens in a context:
* where the person is
* who they are with
* what they feel
* what they expect
* what their body has learned to anticipate
That context can become a cue.
The brain learns that certain signals predict drug availability.
Over time, the cue stops being background.
It becomes a trigger for craving, attention, motivation, and drug-seeking behaviour.
The brain learns that certain signals predict drug availability.
Over time, the cue stops being background.
It becomes a trigger for craving, attention, motivation, and drug-seeking behaviour.
This is why relapse may not begin at the moment of use.
It may begin earlier.
A cue appears.
Prediction starts.
Attention narrows.
Motivation rises.
Drug-seeking begins.
By the time use occurs, the relapse process may already be underway.
It may begin earlier.
A cue appears.
Prediction starts.
Attention narrows.
Motivation rises.
Drug-seeking begins.
By the time use occurs, the relapse process may already be underway.
The mechanism is conditioning.
The brain pairs substance use with the signals around it:
* the bar
* the contact
* the argument
* the loneliness
* the payday
* the withdrawal state
The brain learns:
“When this appears, the drug may be near.”
The brain pairs substance use with the signals around it:
* the bar
* the contact
* the argument
* the loneliness
* the payday
* the withdrawal state
The brain learns:
“When this appears, the drug may be near.”
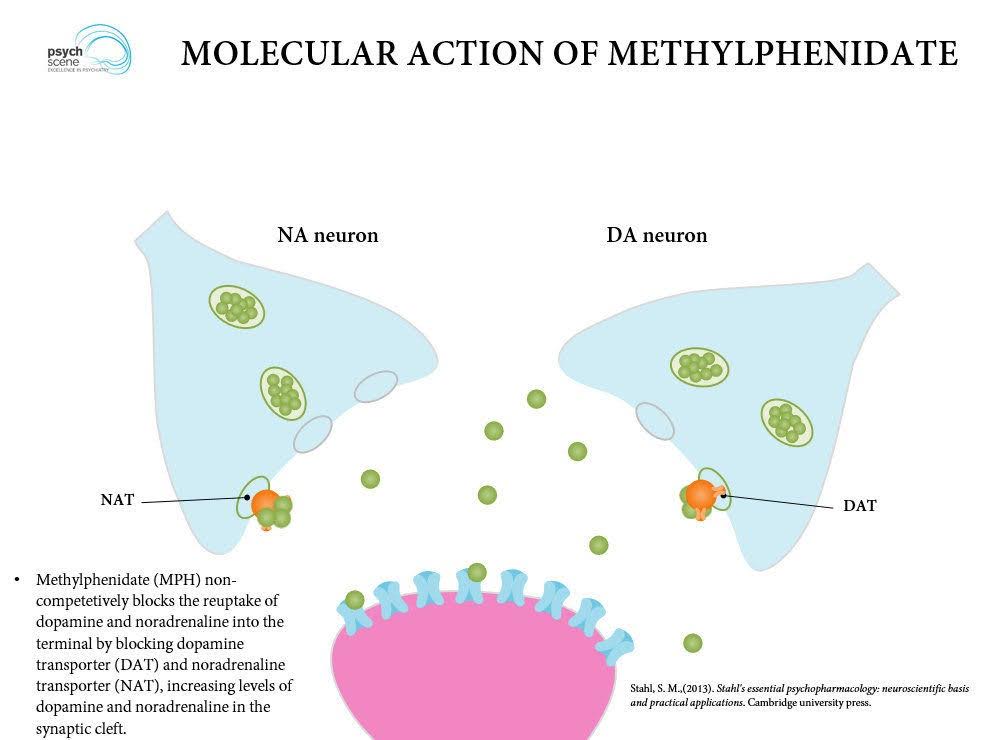
Dopamine helps encode that prediction.
At first, the drug may carry the strongest reward signal.
But with repeated use, dopamine firing can shift earlier.
From the drug itself…
to the cue that predicts it.
At first, the drug may carry the strongest reward signal.
But with repeated use, dopamine firing can shift earlier.
From the drug itself…
to the cue that predicts it.
That shift is clinically important.
The cue begins to organise:
* attention
* craving
* motivation
* preparation
* drug-seeking behaviour
The patient is not only remembering use.
The brain is preparing for it.
The cue begins to organise:
* attention
* craving
* motivation
* preparation
* drug-seeking behaviour
The patient is not only remembering use.
The brain is preparing for it.

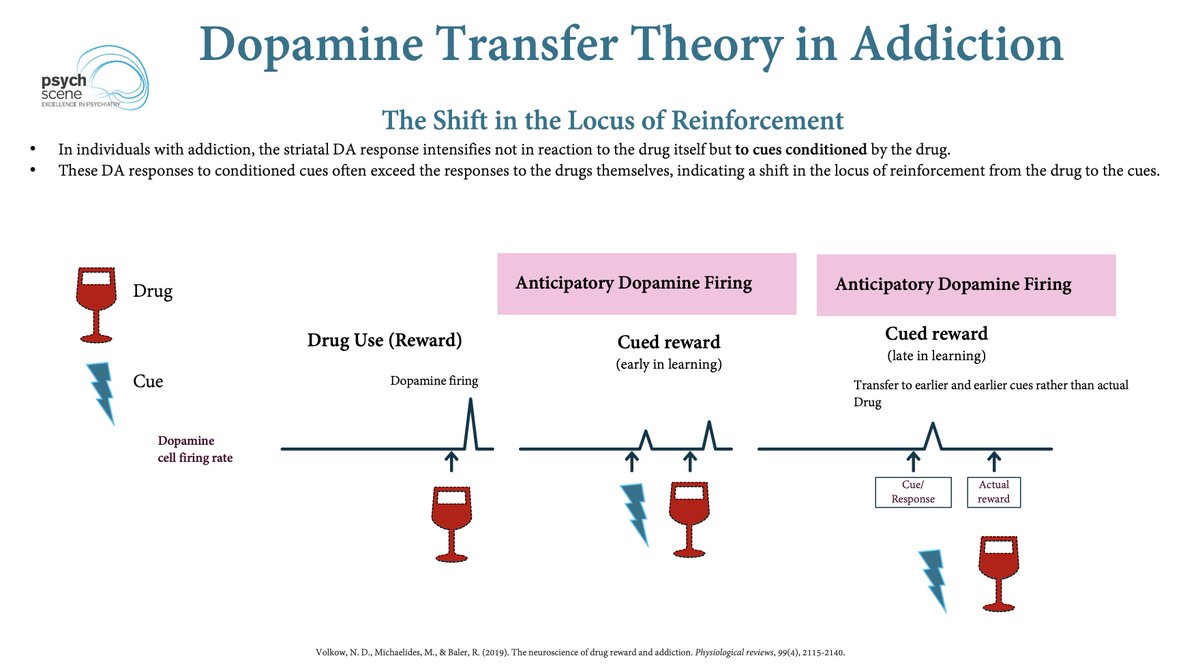
In addiction, conditioned cues can produce strong striatal dopamine responses.
In some cases, the dopamine response to the cue may exceed the response to the drug itself.
The signal has shifted.
The cue has become biologically powerful.
In some cases, the dopamine response to the cue may exceed the response to the drug itself.
The signal has shifted.
The cue has become biologically powerful.
This is why “just don’t use” is often too shallow.
The patient may be trying to resist the final step.
But the sequence may have started earlier:
with the cue that activated the seeking system.
Relapse prevention has to move upstream.
The patient may be trying to resist the final step.
But the sequence may have started earlier:
with the cue that activated the seeking system.
Relapse prevention has to move upstream.
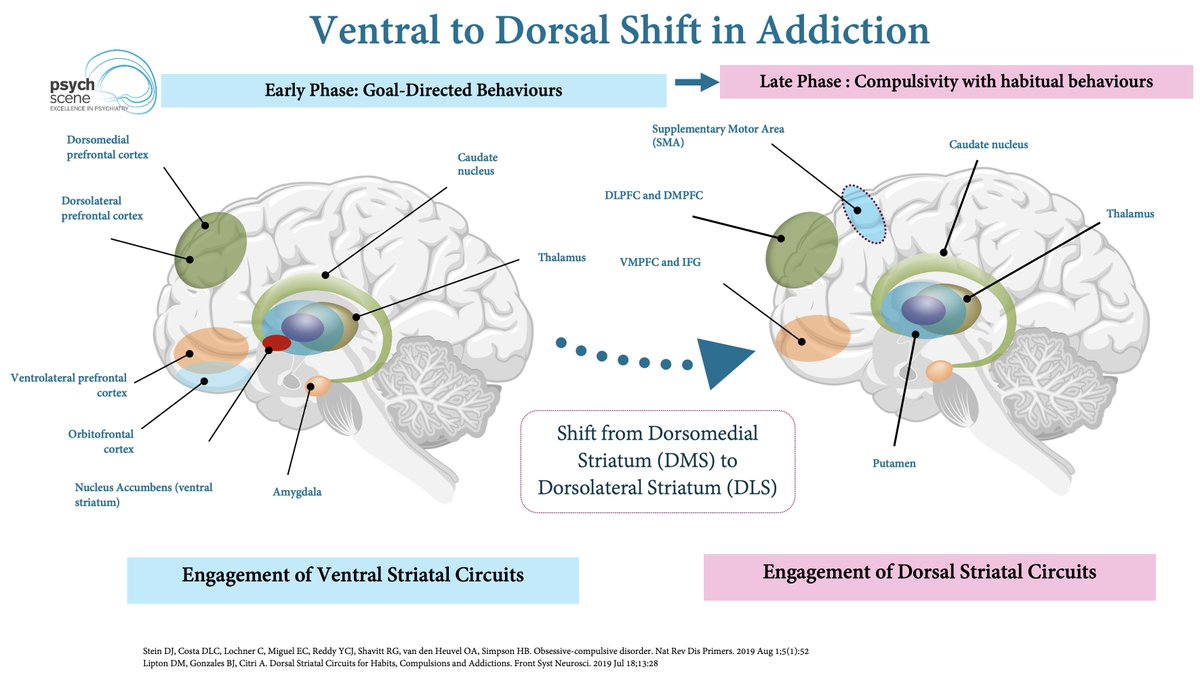
Now add habit learning.
Repeated cue-drug pairings can shift behaviour from flexible, goal-directed choice toward more automatic responding.
The question becomes less:
“Do I want this?”
and more:
“This cue means act.”
Repeated cue-drug pairings can shift behaviour from flexible, goal-directed choice toward more automatic responding.
The question becomes less:
“Do I want this?”
and more:
“This cue means act.”
This is where the striatum becomes important.
Addiction can involve a shift from ventral striatal reward processing toward dorsal striatal habit circuitry.
In practical terms:
drug-seeking becomes less sensitive to consequences…
and more driven by stimulus-response patterns.
Addiction can involve a shift from ventral striatal reward processing toward dorsal striatal habit circuitry.
In practical terms:
drug-seeking becomes less sensitive to consequences…
and more driven by stimulus-response patterns.
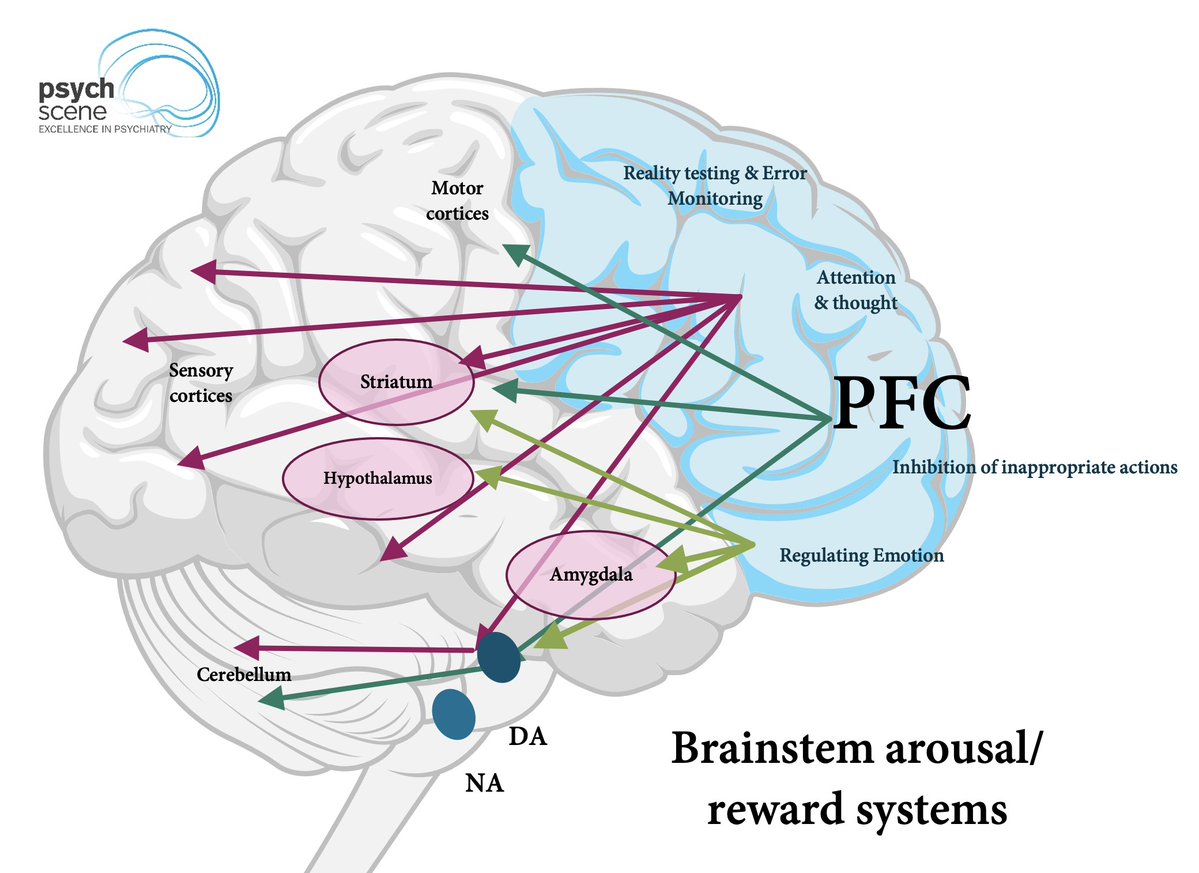
The prefrontal cortex also matters.
It supports:
* inhibitory control
* decision-making
* emotion regulation
* delayed gratification
But during cue-driven craving, top-down control may struggle against conditioned motivation.
The patient may know the consequence and still feel pulled toward use.
It supports:
* inhibitory control
* decision-making
* emotion regulation
* delayed gratification
But during cue-driven craving, top-down control may struggle against conditioned motivation.
The patient may know the consequence and still feel pulled toward use.
The insula adds another layer.
Cues are not only external.
They can be internal:
* tension
* craving
* stress
* withdrawal sensations
* bodily discomfort
The body state itself can become part of the cue network.
Cues are not only external.
They can be internal:
* tension
* craving
* stress
* withdrawal sensations
* bodily discomfort
The body state itself can become part of the cue network.
So clinically, cue mapping matters.
Ask:
What happens before craving?
Where are they?
Who are they with?
What are they feeling?
What body state appears?
What routine predicts use?
The relapse sequence usually starts before the relapse.
Ask:
What happens before craving?
Where are they?
Who are they with?
What are they feeling?
What body state appears?
What routine predicts use?
The relapse sequence usually starts before the relapse.
Putting it together:
drug exposure → cue learning → dopamine prediction → craving → narrowed attention → habit circuitry → drug-seeking → relapse risk
The drug may start the learning.
But the cue can later run the sequence.
drug exposure → cue learning → dopamine prediction → craving → narrowed attention → habit circuitry → drug-seeking → relapse risk
The drug may start the learning.
But the cue can later run the sequence.
Relapse prevention cannot start only at the moment of use.
It has to move upstream:
To the cues, predictions, body states, and habits that start the seeking sequence.
To learn more about the neuroscience of addiction and how it translates into clinical practice, click the link below and check out the full course inside The Academy:
psychscene.co/42Yw9hu
It has to move upstream:
To the cues, predictions, body states, and habits that start the seeking sequence.
To learn more about the neuroscience of addiction and how it translates into clinical practice, click the link below and check out the full course inside The Academy:
psychscene.co/42Yw9hu
• • •
Missing some Tweet in this thread? You can try to
force a refresh