
We provide psychiatry education for Psychiatrists, GPs & Mental Health Practitioners. • Join The Academy 👇
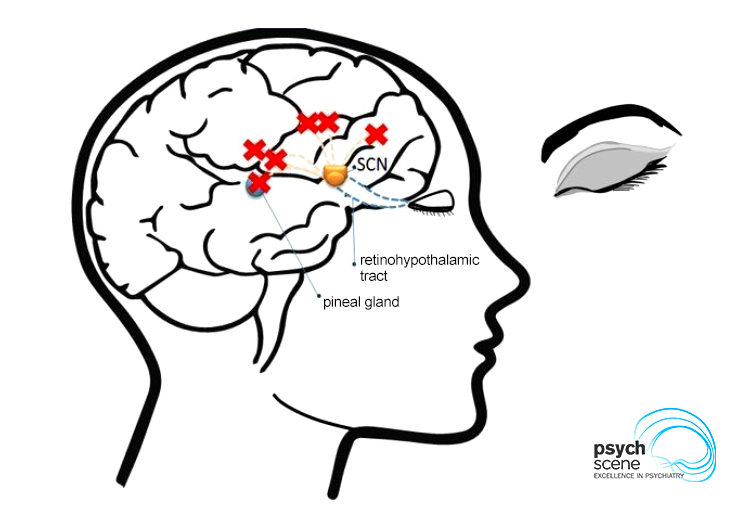 Agomelatine has two key receptor actions:
Agomelatine has two key receptor actions:
 1/ Affective-Interpersonal Pattern
1/ Affective-Interpersonal Pattern 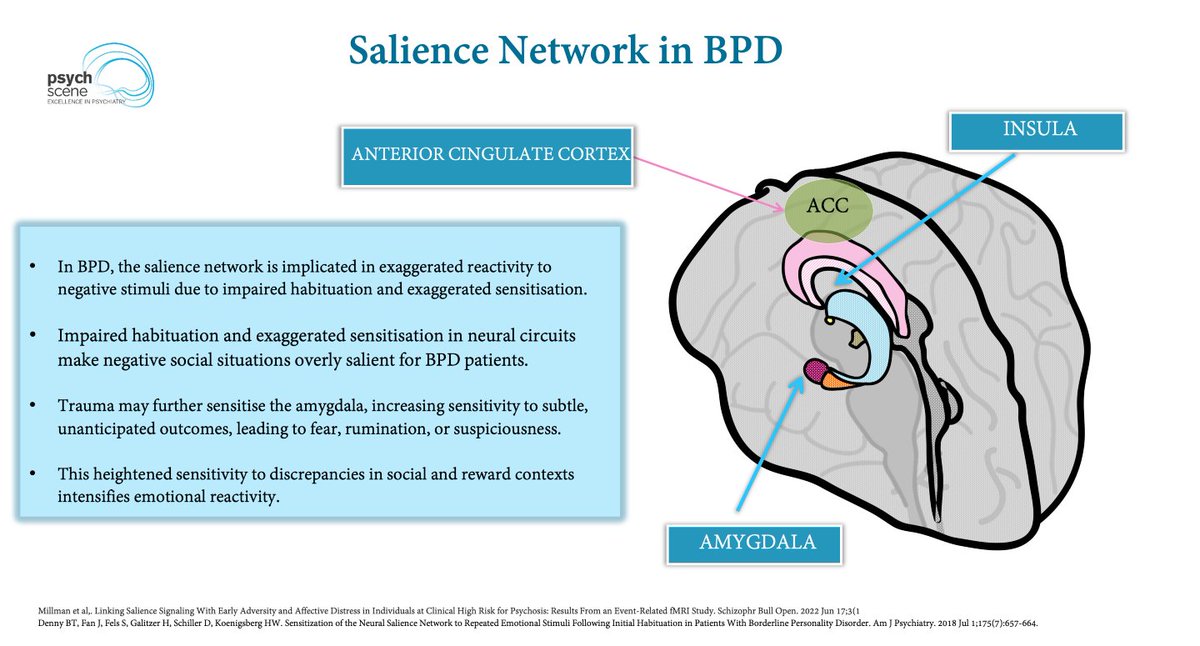 Prediction errors = expectation vs outcome
Prediction errors = expectation vs outcome The brain is predictive by nature.
The brain is predictive by nature. At ‘face value’, BPD can look a lot like cPTSD.
At ‘face value’, BPD can look a lot like cPTSD. Diagnostic labels separate ADHD and ASD.
Diagnostic labels separate ADHD and ASD. In schizophrenia, reward processing is not only about pleasure.
In schizophrenia, reward processing is not only about pleasure.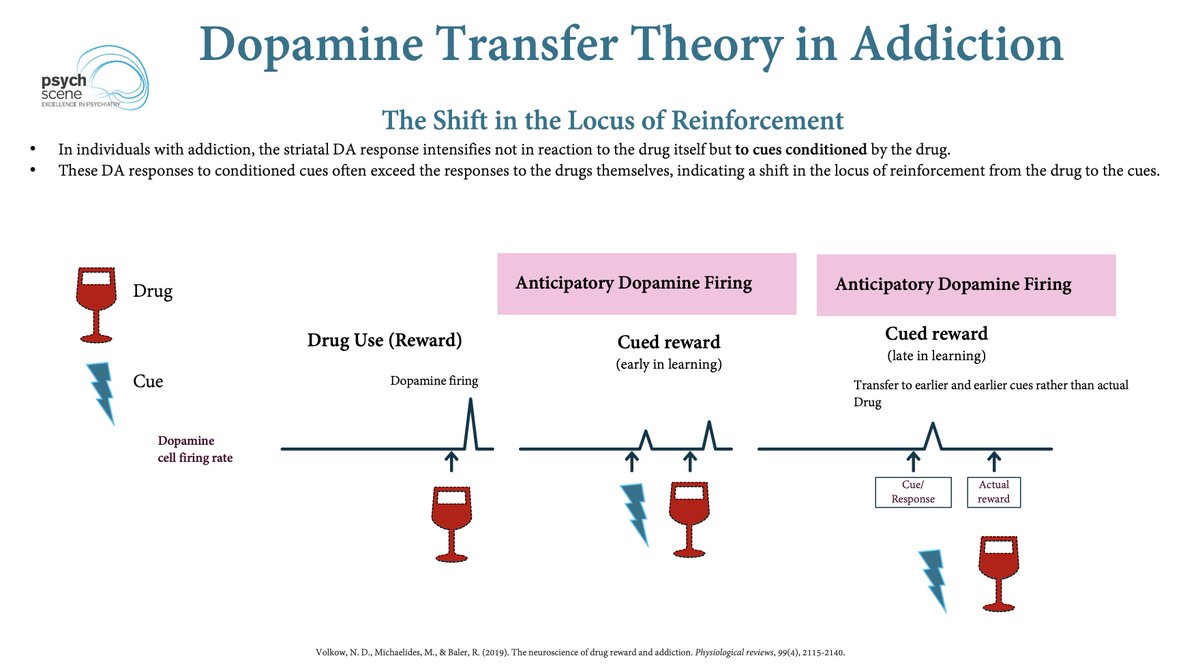 To understand why, start with what repeated drug use teaches the brain.
To understand why, start with what repeated drug use teaches the brain. 1/ Attachment
1/ Attachment
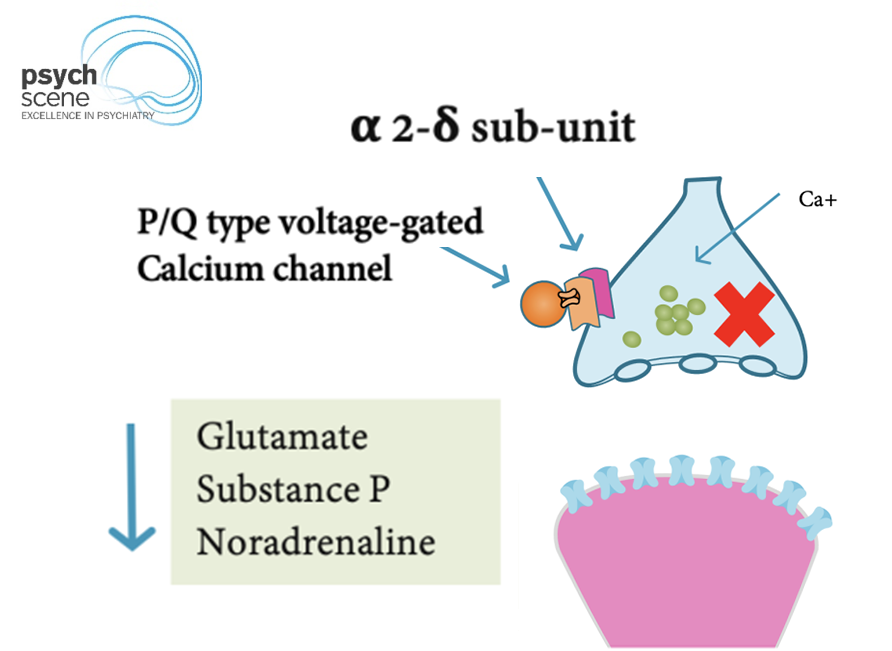 Despite their structural similarity to GABA, gabapentin and pregabalin do not bind to GABA-A or GABA-B receptors.
Despite their structural similarity to GABA, gabapentin and pregabalin do not bind to GABA-A or GABA-B receptors. Let’s start with the definition.
Let’s start with the definition.
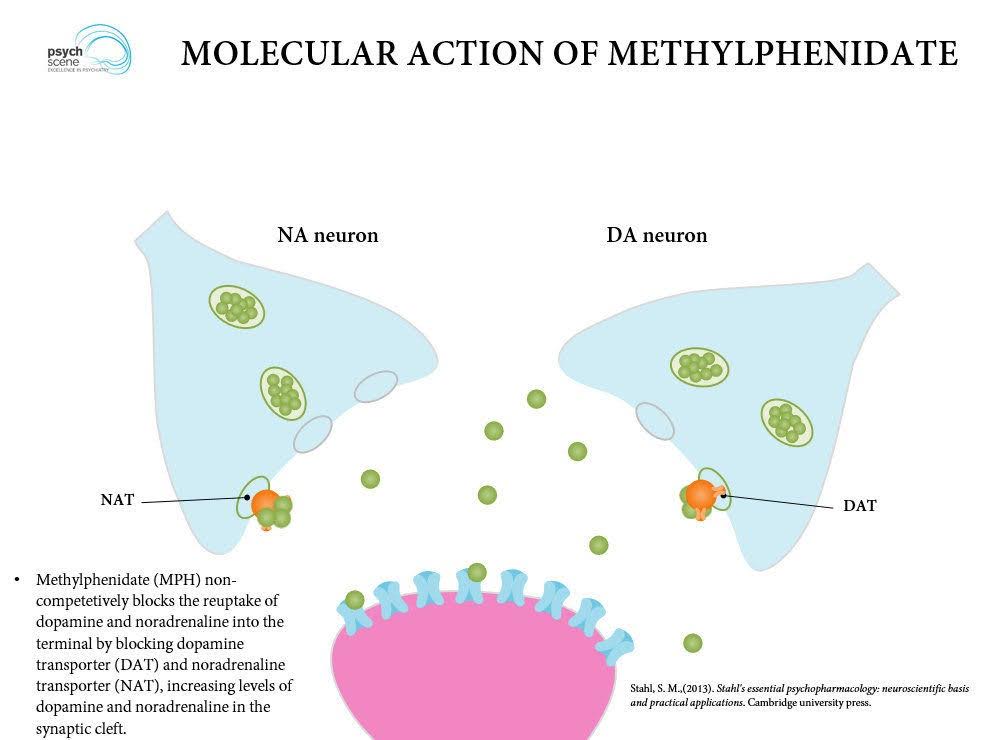 Methylphenidate blocks the reuptake of:
Methylphenidate blocks the reuptake of: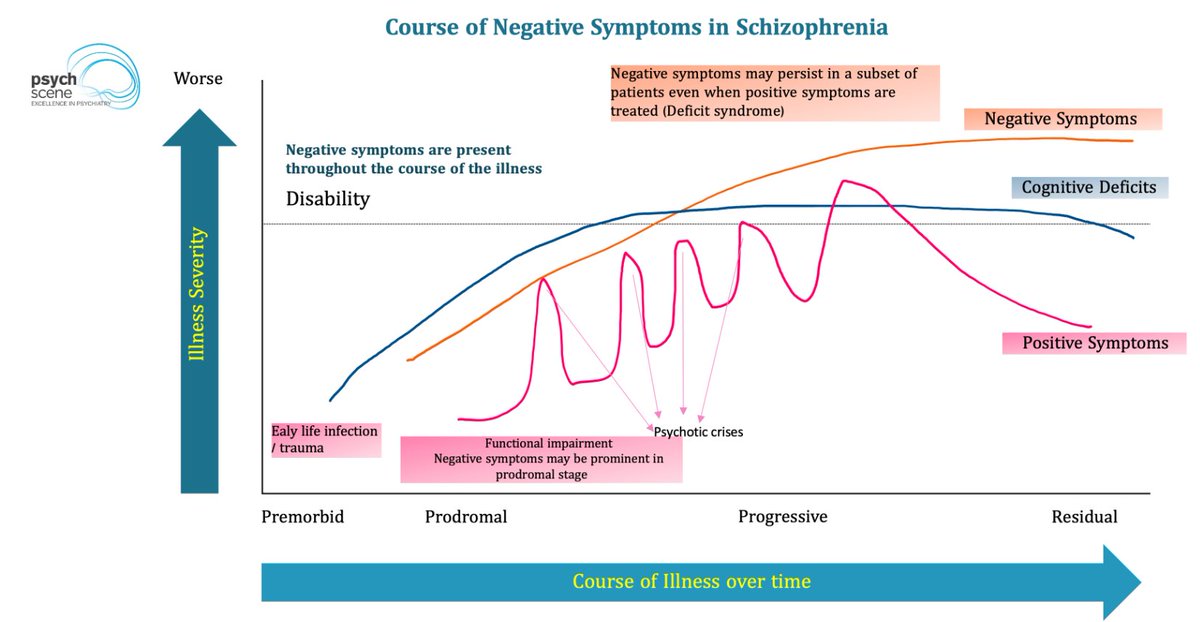 This is the recovery gap in schizophrenia.
This is the recovery gap in schizophrenia.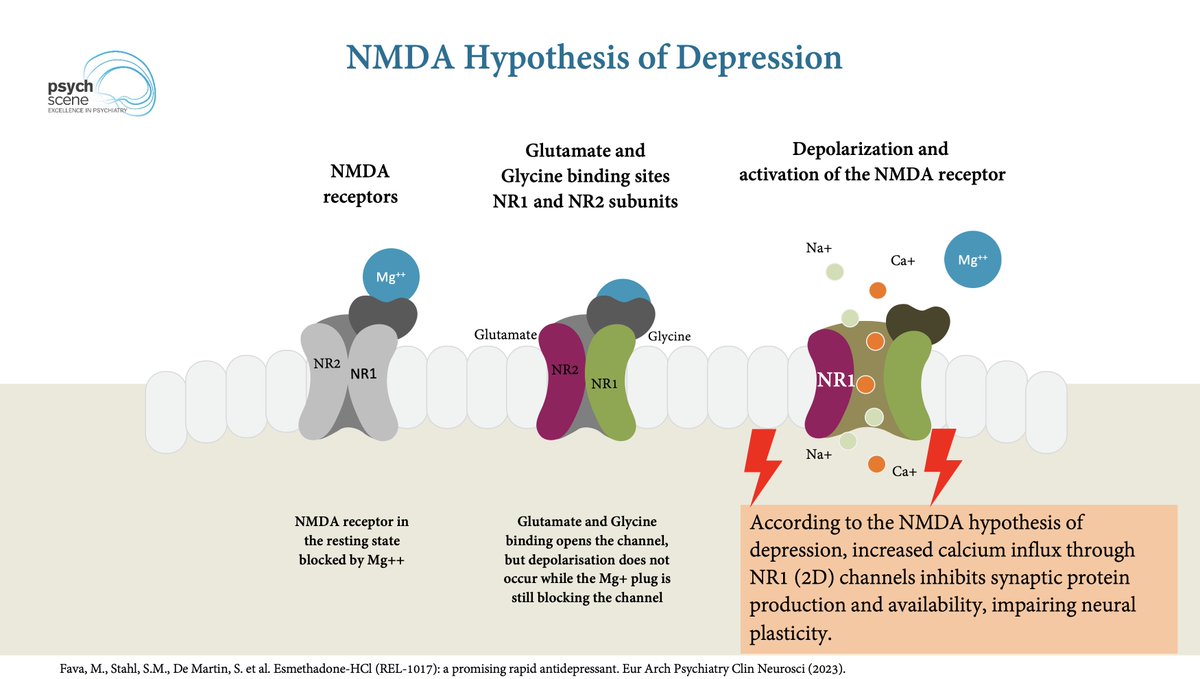 For decades, antidepressants have largely targeted monoamine systems:
For decades, antidepressants have largely targeted monoamine systems: Both medications can be useful in ADHD when stimulants are:
Both medications can be useful in ADHD when stimulants are: This is where the Tripartite Model of Fronto-Striato-Limbic Circuits becomes useful.
This is where the Tripartite Model of Fronto-Striato-Limbic Circuits becomes useful.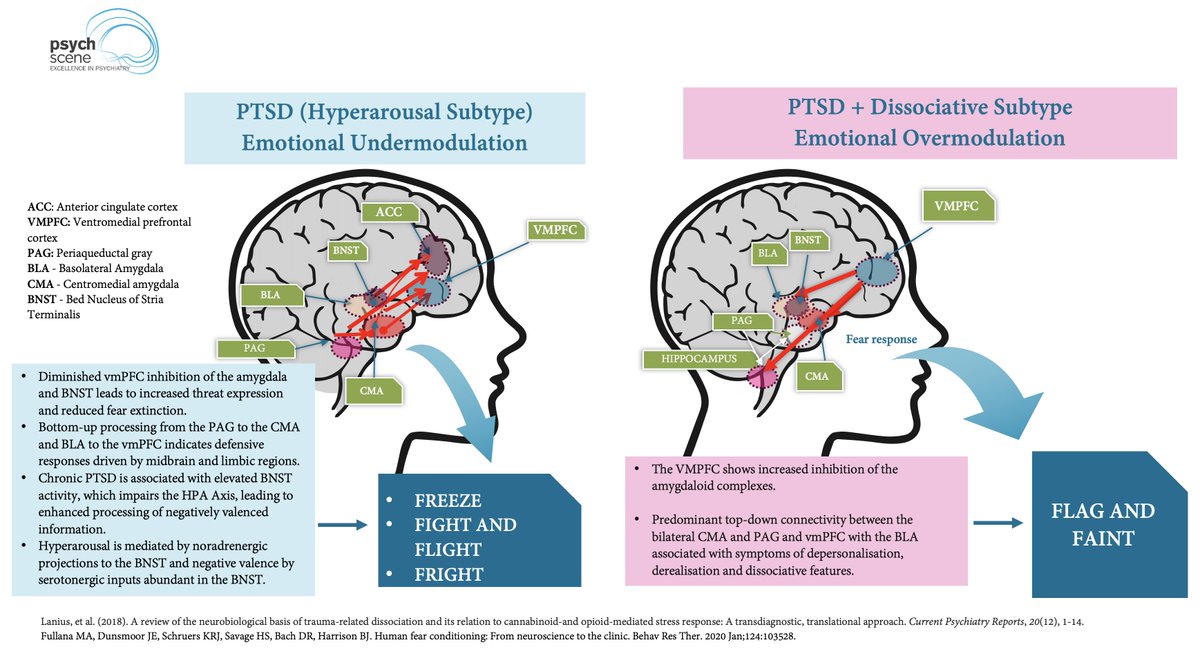 Around 13–30% of individuals with PTSD meet criteria for the dissociative subtype.
Around 13–30% of individuals with PTSD meet criteria for the dissociative subtype. The dorsal striatum is not just a motor structure.
The dorsal striatum is not just a motor structure.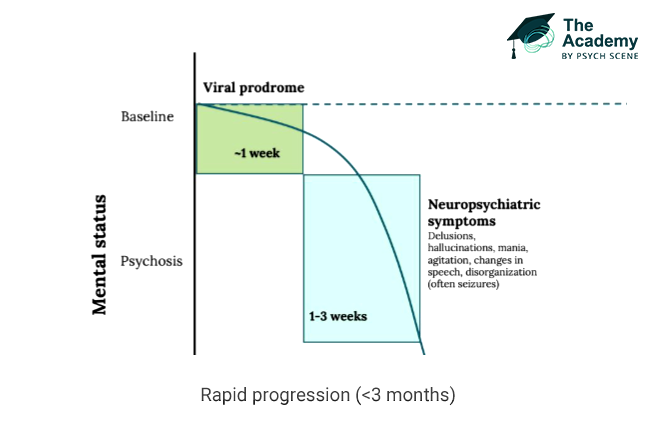 AE diagnosis can be considered when all three of the following criteria are met.
AE diagnosis can be considered when all three of the following criteria are met.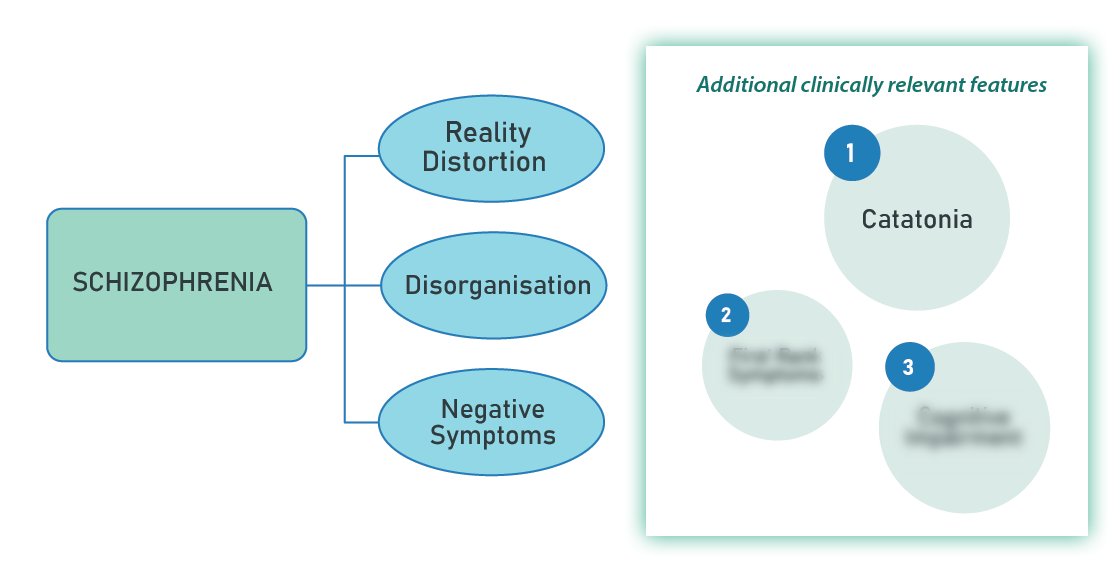 1/ Catatonia
1/ Catatonia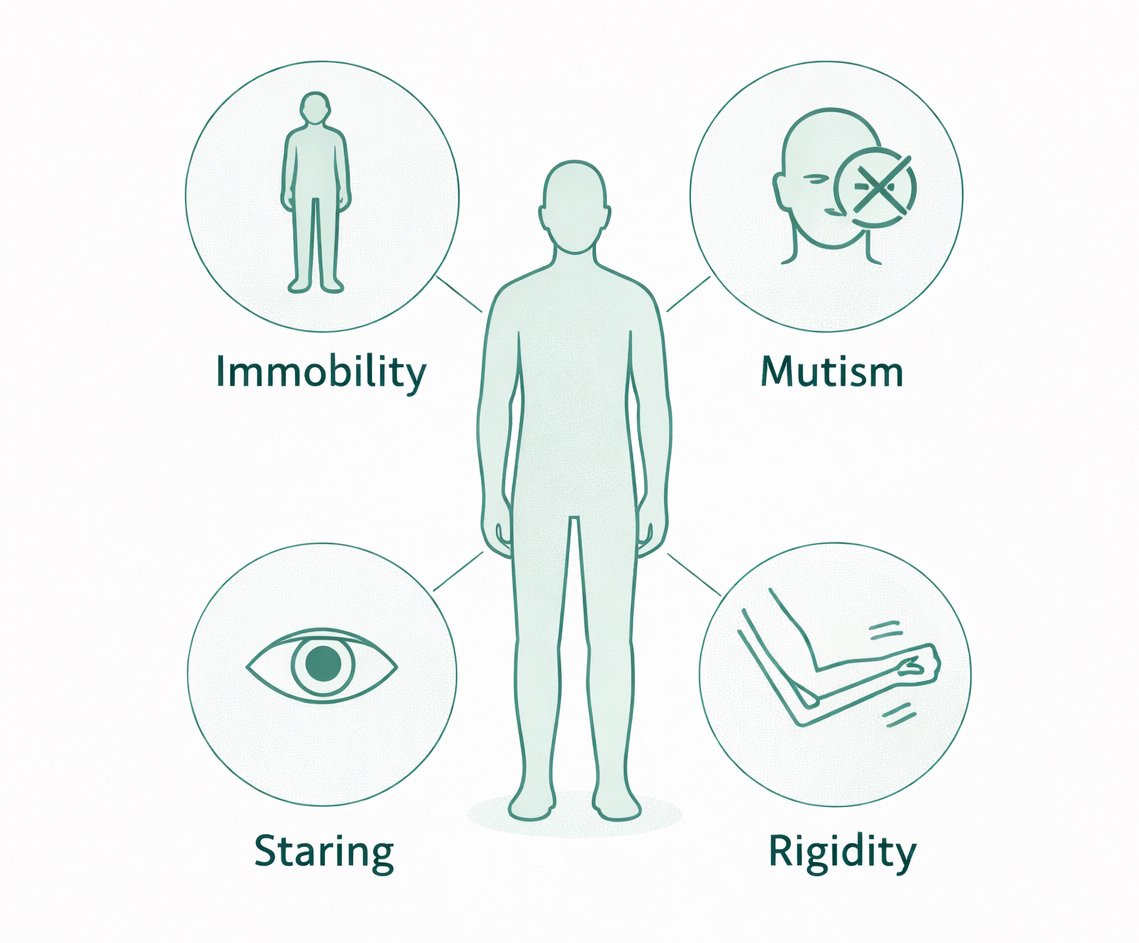
 1/ Avoid the Mind–Body Split
1/ Avoid the Mind–Body Split