Tucker Carlson admitted he used to make fun of people who believe vaccines cause autism.
He now describes his behavior as “unthinking, stupid, and reactionary.”
Tucker says people are noticing what Robert De Niro noticed about vaccines before he suddenly abandoned the issue: “There’s something there that people aren’t addressing” with vaccines and autism.
De Niro declared this on “The Today Show” back in 2016. Let the clip roll, and you’ll see it.
Fast forward to today, and it’s hard to believe De Niro actually said what he did on mainstream television.
What’s even harder to believe is just how most of the vaccines used today got approved in the first place.
“Placebo” doesn’t mean what most people think it means when it comes to vaccines.
Once you understand what a vaccine “placebo” is, the way evidence gets buried starts making a lot more sense. 🧵
He now describes his behavior as “unthinking, stupid, and reactionary.”
Tucker says people are noticing what Robert De Niro noticed about vaccines before he suddenly abandoned the issue: “There’s something there that people aren’t addressing” with vaccines and autism.
De Niro declared this on “The Today Show” back in 2016. Let the clip roll, and you’ll see it.
Fast forward to today, and it’s hard to believe De Niro actually said what he did on mainstream television.
What’s even harder to believe is just how most of the vaccines used today got approved in the first place.
“Placebo” doesn’t mean what most people think it means when it comes to vaccines.
Once you understand what a vaccine “placebo” is, the way evidence gets buried starts making a lot more sense. 🧵
Something strange happens when people first start looking seriously at vaccine safety data.
They do the research. They find the studies. They bring the evidence carefully into a conversation that feels safe and possible.
But nothing moves.
The other person doesn’t adjust. Doesn’t even get curious. They just double down harder.
Nothing about it feels like a normal disagreement. It feels like something else entirely.
Because it is.
And there’s actually a specific reason for that. A reason that goes much deeper than tribalism.
They do the research. They find the studies. They bring the evidence carefully into a conversation that feels safe and possible.
But nothing moves.
The other person doesn’t adjust. Doesn’t even get curious. They just double down harder.
Nothing about it feels like a normal disagreement. It feels like something else entirely.
Because it is.
And there’s actually a specific reason for that. A reason that goes much deeper than tribalism.

The reason vaccine orthodoxy functions differently from almost every other medical debate isn’t random.
It’s structural. It was designed and built this way.
To understand why the evidence lands differently here—why the same standards of proof that apply literally everywhere else somehow don’t apply to vaccines—you have to understand what vaccines actually represent in Western medicine.
And it’s probably not what you think.
It’s structural. It was designed and built this way.
To understand why the evidence lands differently here—why the same standards of proof that apply literally everywhere else somehow don’t apply to vaccines—you have to understand what vaccines actually represent in Western medicine.
And it’s probably not what you think.

This information comes from the work of medical researcher @MidwesternDoc. For all the sources and details, read the full report here:
midwesterndoctor.com/p/dissecting-t…
midwesterndoctor.com/p/dissecting-t…
In 1979, a physician named Robert Mendelsohn published “Confessions of a Medical Heretic.”
His central argument was this: modern medicine isn’t an art or a science—it’s a religion.
Doctors replaced priests. White coats replaced priest robes. Hospitals became temples. Drugs became communion wafers.
And vaccines became the holy water—the ritual that baptizes you into the faith.
Mendelsohn made numerous television appearances on vaccine dangers in the early 1980s—debates that were broadcast to millions. Those segments could never air today. The exact same arguments he made back then were validated in nearly every detail throughout COVID-19.
That framing—medicine as religion, vaccines as holy water—isn’t just a metaphor. It explains exactly what you’re up against when you try to have a factual conversation about vaccine safety.
His central argument was this: modern medicine isn’t an art or a science—it’s a religion.
Doctors replaced priests. White coats replaced priest robes. Hospitals became temples. Drugs became communion wafers.
And vaccines became the holy water—the ritual that baptizes you into the faith.
Mendelsohn made numerous television appearances on vaccine dangers in the early 1980s—debates that were broadcast to millions. Those segments could never air today. The exact same arguments he made back then were validated in nearly every detail throughout COVID-19.
That framing—medicine as religion, vaccines as holy water—isn’t just a metaphor. It explains exactly what you’re up against when you try to have a factual conversation about vaccine safety.
Three forces converged to create this.
The first is structural: medicine’s entire claim to social prestige rests on a mythology—that it rescued humanity from the dark ages of infectious disease. Vaccines are the centerpiece of that mythology.
But there’s a problem. The actual data shows that only 3.5% of the decline in overall death rates can be attributed to all medical interventions combined. The rest was sanitation, nutrition, and improved living conditions.
Medicine falsely claimed credit for a transition it mostly watched happen. And vaccines are the flag planted on top of that false claim.
If vaccines fall, the mythology falls. Which means those who built careers on it are, psychologically speaking, unable to reconsider.
The first is structural: medicine’s entire claim to social prestige rests on a mythology—that it rescued humanity from the dark ages of infectious disease. Vaccines are the centerpiece of that mythology.
But there’s a problem. The actual data shows that only 3.5% of the decline in overall death rates can be attributed to all medical interventions combined. The rest was sanitation, nutrition, and improved living conditions.
Medicine falsely claimed credit for a transition it mostly watched happen. And vaccines are the flag planted on top of that false claim.
If vaccines fall, the mythology falls. Which means those who built careers on it are, psychologically speaking, unable to reconsider.
The second force is cognitive. Medical training relies on shortcuts—if A then B—without necessarily verifying why. When those assumptions are challenged, the trained response is to double down, not investigate. That tendency gets reinforced by the fact that admitting vaccine harm means admitting you harmed patients you personally treated.
The third force is societal. When traditional religion was displaced in Western culture, the need for shared faith didn’t disappear—it got redirected.
Science filled the gap. But science-as-institution gradually morphed into scientism: a framework claiming objectivity while functioning like doctrine. You can hear it in the language. “I believe in science.” “I believe in vaccines.” “Anyone who questions this must be silenced.”
That’s not the language of evidence. That’s the language of heresy.
The third force is societal. When traditional religion was displaced in Western culture, the need for shared faith didn’t disappear—it got redirected.
Science filled the gap. But science-as-institution gradually morphed into scientism: a framework claiming objectivity while functioning like doctrine. You can hear it in the language. “I believe in science.” “I believe in vaccines.” “Anyone who questions this must be silenced.”
That’s not the language of evidence. That’s the language of heresy.

The vaccine-as-holy-water metaphor isn’t just philosophical.
Medical students and healthcare workers are required to be fully vaccinated—which filters out anyone not aligned with the doctrine before they can enter the profession. Those who comply are then expected to administer the sacrament to patients.
During COVID-19, segments of the public began formally excommunicating the unvaccinated—excluded from employment, restaurants, social life.
The ritual function was visible in real time. This wasn’t public health policy. It was enforcement of a faith boundary.
Medical students and healthcare workers are required to be fully vaccinated—which filters out anyone not aligned with the doctrine before they can enter the profession. Those who comply are then expected to administer the sacrament to patients.
During COVID-19, segments of the public began formally excommunicating the unvaccinated—excluded from employment, restaurants, social life.
The ritual function was visible in real time. This wasn’t public health policy. It was enforcement of a faith boundary.
@MidwesternDoc The full article from @MidwesternDoc lays out exactly how vaccine orthodoxy became untouchable—and how the research system was deliberately built to make harm nearly impossible to prove. It’s worth the read.
midwesterndoctor.com/p/dissecting-t…
midwesterndoctor.com/p/dissecting-t…
Here’s the mechanism that protects the entire system from evidence.
Placebo-controlled trials—the gold standard of medical proof—are declared “unethical” for vaccines because they would deny children a “life-saving” intervention. So large retrospective studies comparing vaccinated and unvaccinated children become the best available evidence.
But when those studies show harm, they’re dismissed as “non-controlled.” Demands go up for the controlled trials that were just declared unethical.
The trap closes. Evidence of harm can never satisfy the evidentiary standard, because the evidentiary standard requires the study design that’s been banned.
The Institute of Medicine—cited for decades as the definitive authority on vaccine safety—published major reports in 1994 and 2012. What those reports actually said was that insufficient evidence existed to definitively support or disprove a link between vaccines and serious injury, and that this research should be urgently conducted.
But it never was.
Placebo-controlled trials—the gold standard of medical proof—are declared “unethical” for vaccines because they would deny children a “life-saving” intervention. So large retrospective studies comparing vaccinated and unvaccinated children become the best available evidence.
But when those studies show harm, they’re dismissed as “non-controlled.” Demands go up for the controlled trials that were just declared unethical.
The trap closes. Evidence of harm can never satisfy the evidentiary standard, because the evidentiary standard requires the study design that’s been banned.
The Institute of Medicine—cited for decades as the definitive authority on vaccine safety—published major reports in 1994 and 2012. What those reports actually said was that insufficient evidence existed to definitively support or disprove a link between vaccines and serious injury, and that this research should be urgently conducted.
But it never was.
Meanwhile, retrospective data supporting vaccine safety is widely published and cited without scrutiny. The same data type showing harm gets dismissed as inadequate. Same methodology. Different outcome based on the direction of the finding.
That asymmetry wasn’t accidental.
Leaked records obtained through litigation show that IOM committee members were told at the outset that their final report—the one cited as definitive proof of vaccine safety—could not provide evidence suggesting vaccines cause harm.
The conclusion was set before the review began.
That asymmetry wasn’t accidental.
Leaked records obtained through litigation show that IOM committee members were told at the outset that their final report—the one cited as definitive proof of vaccine safety—could not provide evidence suggesting vaccines cause harm.
The conclusion was set before the review began.
@MidwesternDoc There’s a phrase for treating absence of evidence as evidence of absence.
It’s a category error. A logical fallacy covered in any introduction to philosophy course.
In vaccine science, it became official regulatory policy.
It’s a category error. A logical fallacy covered in any introduction to philosophy course.
In vaccine science, it became official regulatory policy.
The structural manipulation inside vaccine trials goes further.
Trials are monitored for extraordinarily short follow-up periods. The clinical studies for the hepatitis B vaccine—given to every newborn in the United States—tracked side effects for only four to five days post-vaccination.
Most of the chronic conditions associated with vaccines—autoimmune disorders, neurological injuries, developmental changes—take weeks, months, or years to become apparent.
A four-day window doesn’t miss those outcomes by accident. A four-day window is specifically sized to miss them.
Trials are monitored for extraordinarily short follow-up periods. The clinical studies for the hepatitis B vaccine—given to every newborn in the United States—tracked side effects for only four to five days post-vaccination.
Most of the chronic conditions associated with vaccines—autoimmune disorders, neurological injuries, developmental changes—take weeks, months, or years to become apparent.
A four-day window doesn’t miss those outcomes by accident. A four-day window is specifically sized to miss them.

But the most structurally dishonest feature of vaccine trial design is what gets used as the “placebo.”
Real placebos are inert. Saline. Something that does nothing, so any adverse event difference between groups is visible.
Shockingly, most vaccine trials use another vaccine as the control—often for a completely different disease. That means the “placebo” group is also experiencing vaccine-induced biological effects. When adverse event rates look similar between groups, the vaccine is declared safe.
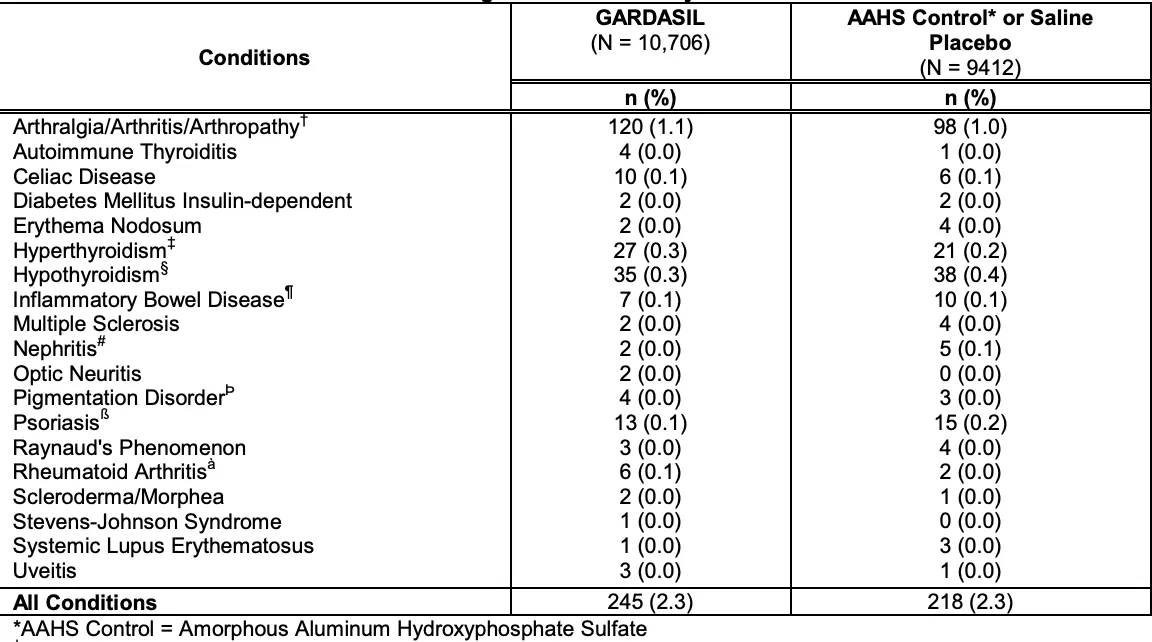
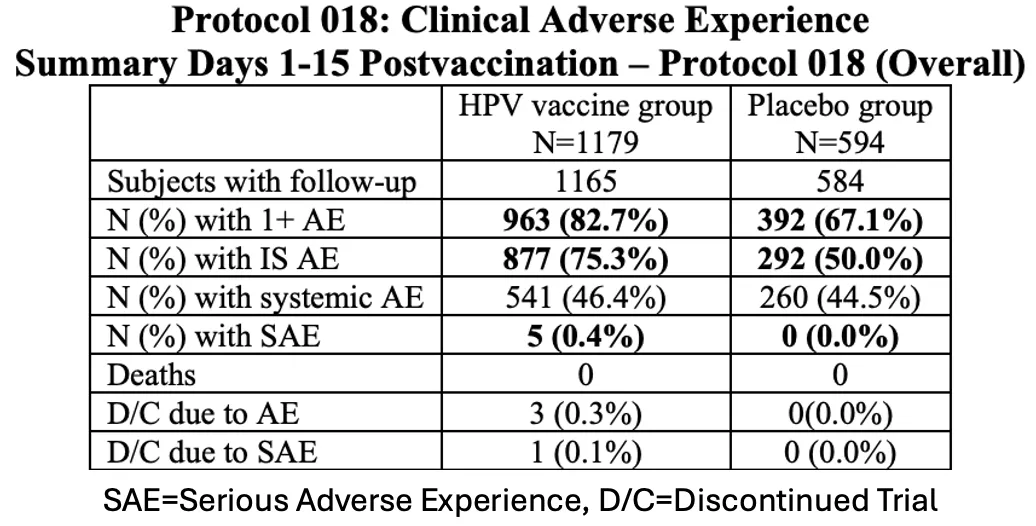
In the HPV vaccine trials, the control substance used as a “placebo” was an aluminum adjuvant—a compound with its own documented inflammatory properties. In those trials, 2.3% of participants in both the vaccine and “placebo” groups developed life-altering autoimmune conditions.
The placebo was also causing autoimmune conditions. That’s not a clean comparison. That’s a mechanism specifically designed to make the signal disappear.
And if you trace any vaccine trial chain back far enough, the very first vaccine in the sequence was simply never tested against an inert placebo at all. It was assumed safe. Every trial after it built its “safety” comparison on top of that untested assumption.
Real placebos are inert. Saline. Something that does nothing, so any adverse event difference between groups is visible.
Shockingly, most vaccine trials use another vaccine as the control—often for a completely different disease. That means the “placebo” group is also experiencing vaccine-induced biological effects. When adverse event rates look similar between groups, the vaccine is declared safe.
In the HPV vaccine trials, the control substance used as a “placebo” was an aluminum adjuvant—a compound with its own documented inflammatory properties. In those trials, 2.3% of participants in both the vaccine and “placebo” groups developed life-altering autoimmune conditions.
The placebo was also causing autoimmune conditions. That’s not a clean comparison. That’s a mechanism specifically designed to make the signal disappear.
And if you trace any vaccine trial chain back far enough, the very first vaccine in the sequence was simply never tested against an inert placebo at all. It was assumed safe. Every trial after it built its “safety” comparison on top of that untested assumption.
In the initial Gardasil trials covering over 21,000 subjects, the death rate in the vaccine group was 8.5 per 10,000. The “placebo” group’s death rate was 7.2 per 10,000.
The expected background death rate for girls and young women of the same age: 4.37 per 10,000.
Both the vaccine group and the control group were dying at nearly double the baseline. The FDA’s determination: no concern, because the rates matched each other.
But they matched each other on purpose. Young women and girls died by design.
A system designed to detect safety signals failed to notice that both groups were dying at an anomalous rate. Because matching an also-anomalous control means the trial, by design, cannot see its own signal.
The expected background death rate for girls and young women of the same age: 4.37 per 10,000.
Both the vaccine group and the control group were dying at nearly double the baseline. The FDA’s determination: no concern, because the rates matched each other.
But they matched each other on purpose. Young women and girls died by design.
A system designed to detect safety signals failed to notice that both groups were dying at an anomalous rate. Because matching an also-anomalous control means the trial, by design, cannot see its own signal.
@MidwesternDoc The full piece from @MidwesternDoc goes deeper into this—including the complete HPV adverse event table, the mechanics of injury reclassification, and additional trial data that never reached the public.
midwesterndoctor.com/p/dissecting-t…
midwesterndoctor.com/p/dissecting-t…
One of the most striking aspects of this story involves a physician who agreed to conduct a vaccinated vs. unvaccinated comparison study—promising in advance to publish the results regardless of what they showed.
The data came back showing vaccines were dangerous—immensely.
The physician refused to publish.
Later, when caught speaking about it on a hidden camera, he admitted he withheld the findings to protect himself.
The footage can be seen in the film “An Inconvenient Study.”
The data came back showing vaccines were dangerous—immensely.
The physician refused to publish.
Later, when caught speaking about it on a hidden camera, he admitted he withheld the findings to protect himself.
The footage can be seen in the film “An Inconvenient Study.”

When the record becomes inconvenient, the record gets deleted.
The CDC itself maintained a large population dataset—one that could have ethically compared vaccinated and unvaccinated children at scale. It’s the exact dataset safety advocates had been requesting for years.
But when Secretary Kennedy prepared to access it, the CDC deleted it.
The CDC itself maintained a large population dataset—one that could have ethically compared vaccinated and unvaccinated children at scale. It’s the exact dataset safety advocates had been requesting for years.
But when Secretary Kennedy prepared to access it, the CDC deleted it.

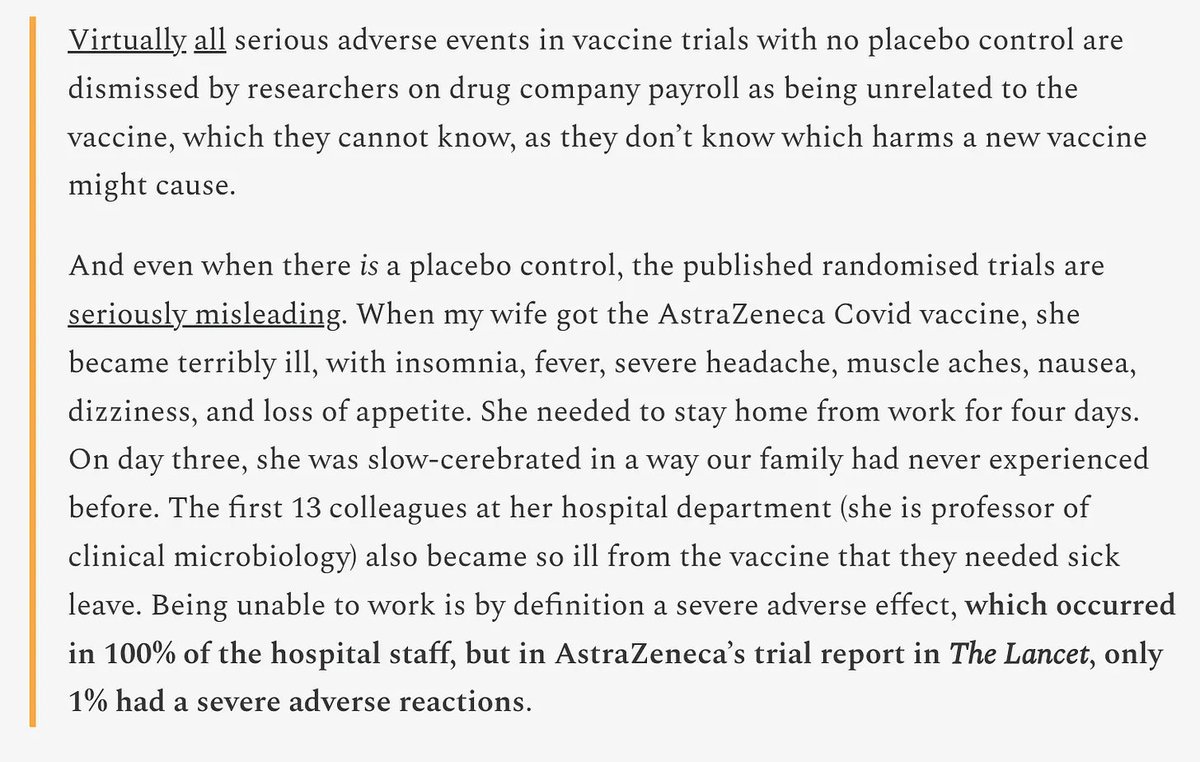
Peter Gøtzsche is one of the world’s foremost experts on pharmaceutical research fraud. What he documented about the AstraZeneca COVID vaccine trial is worth considering.
After his own wife received the vaccine, she experienced severe insomnia, fever, intense headache, muscle aches, nausea, and dizziness—missing four days of work. On the third day, family members described her as cognitively altered in a way they’d never seen.
The first 13 colleagues in her hospital department became similarly debilitated. Every one of them needed sick leave.
But in AstraZeneca’s published trial report in The Lancet: 1% of participants had severe adverse reactions.
100% vs 1%
After his own wife received the vaccine, she experienced severe insomnia, fever, intense headache, muscle aches, nausea, and dizziness—missing four days of work. On the third day, family members described her as cognitively altered in a way they’d never seen.
The first 13 colleagues in her hospital department became similarly debilitated. Every one of them needed sick leave.
But in AstraZeneca’s published trial report in The Lancet: 1% of participants had severe adverse reactions.
100% vs 1%
That gap—100% real-world, 1% published—has a documented mechanism.
Trial investigators have the authority to determine whether an adverse event was caused by the vaccine. They consistently conclude it was not. Because they can.
In COVID vaccine trials, participants testified that a severe cancer was reclassified as enlarged lymph nodes. A permanent disability was reclassified as “functional abdominal pain.”
The injury didn’t disappear. The category changed.
It is shockingly easy to lie with data.
Trial investigators have the authority to determine whether an adverse event was caused by the vaccine. They consistently conclude it was not. Because they can.
In COVID vaccine trials, participants testified that a severe cancer was reclassified as enlarged lymph nodes. A permanent disability was reclassified as “functional abdominal pain.”
The injury didn’t disappear. The category changed.
It is shockingly easy to lie with data.

This pattern isn’t unique to vaccines.
When SSRIs first came to market, the FDA was flooded with reports linking them to suicide, homicide, and mass violence. The agency convened a formal hearing on the subject in September 1991. The industry knew the risk. The data existed.
None of it reached the public until victim lawsuits forced the documents out through discovery decades later.
The same architecture—capture the regulator, suppress the signal, wait for litigation—has operated across every major pharmaceutical category. Vaccines are the most protected version of a system that has never worked the way it claims to.
When SSRIs first came to market, the FDA was flooded with reports linking them to suicide, homicide, and mass violence. The agency convened a formal hearing on the subject in September 1991. The industry knew the risk. The data existed.
None of it reached the public until victim lawsuits forced the documents out through discovery decades later.
The same architecture—capture the regulator, suppress the signal, wait for litigation—has operated across every major pharmaceutical category. Vaccines are the most protected version of a system that has never worked the way it claims to.
The agencies meant to catch this have a structural reason not to.
FOIA’d emails revealed that the CDC’s Immunization Safety Office head was in routine communication with the pharmaceutical industry to set national vaccine policy—while simultaneously blocking citizen groups that were advocating for vaccine safety research. This wasn’t a rogue actor. This was standard operating procedure documented in internal correspondence.
When the CDC and FDA fought to suppress a surge of severe injury reports following the HPV vaccine, the CDC director overseeing that effort subsequently became a Merck executive. Her compensation from Merck exceeded thirty million dollars.
Thirty. Million. Dollars.
Peter Marks—the FDA director who worked consistently to conceal COVID vaccine injury signals and fast-track authorization toward mandates—left the agency and became an executive at Eli Lilly. Trump’s former FDA commissioner joined Pfizer’s board.
This is the incentive structure that governs the regulatory apparatus. Not a conspiracy. A system of rewards so reliable it doesn’t require coordination.
FOIA’d emails revealed that the CDC’s Immunization Safety Office head was in routine communication with the pharmaceutical industry to set national vaccine policy—while simultaneously blocking citizen groups that were advocating for vaccine safety research. This wasn’t a rogue actor. This was standard operating procedure documented in internal correspondence.
When the CDC and FDA fought to suppress a surge of severe injury reports following the HPV vaccine, the CDC director overseeing that effort subsequently became a Merck executive. Her compensation from Merck exceeded thirty million dollars.
Thirty. Million. Dollars.
Peter Marks—the FDA director who worked consistently to conceal COVID vaccine injury signals and fast-track authorization toward mandates—left the agency and became an executive at Eli Lilly. Trump’s former FDA commissioner joined Pfizer’s board.
This is the incentive structure that governs the regulatory apparatus. Not a conspiracy. A system of rewards so reliable it doesn’t require coordination.

There’s a financial reason the federal government cannot afford to find vaccines harmful.
The government pays out vaccine injury claims directly. If even one in five autism cases were linked to vaccines, estimated liability would reach approximately $1.3 trillion.
For context: the entire federal budget in 2017 was $3.3 trillion.
That’s not an abstraction. That number easily explains why the research doesn’t get done. Why the databases get deleted. Why the IOM committee was told what its conclusion needed to be before the members sat down.
The science was never designed to find harm. It was designed to disarm the question.
The government pays out vaccine injury claims directly. If even one in five autism cases were linked to vaccines, estimated liability would reach approximately $1.3 trillion.
For context: the entire federal budget in 2017 was $3.3 trillion.
That’s not an abstraction. That number easily explains why the research doesn’t get done. Why the databases get deleted. Why the IOM committee was told what its conclusion needed to be before the members sat down.
The science was never designed to find harm. It was designed to disarm the question.

@MidwesternDoc The full article from @MidwesternDoc goes so much deeper. It also points to a companion piece reviewing over a dozen suppressed studies showing vaccinated children developed chronic illness at dramatically higher rates.
midwesterndoctor.com/p/dissecting-t…
midwesterndoctor.com/p/dissecting-t…
COVID-19 significantly changed the calculation.
Vaccines were mandated despite failing to stop transmission. Millions were injured. The resulting polling data started coming in and has stayed there ever since.
Surveys consistently conducted since 2022 find roughly a third of recipients experienced side effects, with about one in ten describing those effects as severe. In the most recent survey, 46% of Americans said they believe the COVID vaccine likely caused a significant number of unexplained deaths—with 25% saying this is very likely.
Those aren’t fringe numbers. That’s half the country expressing mainstream population-level doubt that years of official messaging has failed to suppress.
Vaccines were mandated despite failing to stop transmission. Millions were injured. The resulting polling data started coming in and has stayed there ever since.
Surveys consistently conducted since 2022 find roughly a third of recipients experienced side effects, with about one in ten describing those effects as severe. In the most recent survey, 46% of Americans said they believe the COVID vaccine likely caused a significant number of unexplained deaths—with 25% saying this is very likely.
Those aren’t fringe numbers. That’s half the country expressing mainstream population-level doubt that years of official messaging has failed to suppress.

The vaccine brand was used to sell COVID gene therapies. And when that brand corroded, it opened a door.
People who’d been injured by other vaccines—flu shots, childhood immunizations, HPV vaccines—began speaking publicly in numbers impossible to dismiss.
Tucker Carlson told millions of viewers his son developed Guillain-Barré syndrome from a flu shot.
The old wall isn’t holding anymore.
And it’s long overdue.
People who’d been injured by other vaccines—flu shots, childhood immunizations, HPV vaccines—began speaking publicly in numbers impossible to dismiss.
Tucker Carlson told millions of viewers his son developed Guillain-Barré syndrome from a flu shot.
The old wall isn’t holding anymore.
And it’s long overdue.
Lawmakers are starting to name it now.
For decades, the system’s protection required that debate never really begin—because the moment debate starts, the contradictions become immediately visible.
No placebos because unethical.
No non-placebo evidence because uncontrolled.
No data because deleted.
No liability because legally shielded.
Anyone who looks at all four of those things together stops being confused and starts being angry.
For decades, the system’s protection required that debate never really begin—because the moment debate starts, the contradictions become immediately visible.
No placebos because unethical.
No non-placebo evidence because uncontrolled.
No data because deleted.
No liability because legally shielded.
Anyone who looks at all four of those things together stops being confused and starts being angry.

What’s actually happening here is larger than any single injection.
For decades, the same pattern repeated: data buried, trials manipulated, databases deleted, researchers silenced, regulators captured. Not because of a conspiracy in the traditional sense—but because of something more ordinary and more durable.
A system of incentives that rewards conformity, punishes dissent, and grows its legitimacy on a single premise it can never afford to question.
When a society hands a scientific institution the authority of religion—when criticism becomes heresy, when questioning becomes threat, when conclusions must be set before data is collected—it hasn’t elevated science. It’s replaced it with something that wears science’s clothing.
The faith is fracturing now. What gets built in its place—whether it’s something genuinely more honest or simply a new set of untouchable orthodoxies—is a question everyone paying attention is going to have to answer. Before we lose the opportunity.
For decades, the same pattern repeated: data buried, trials manipulated, databases deleted, researchers silenced, regulators captured. Not because of a conspiracy in the traditional sense—but because of something more ordinary and more durable.
A system of incentives that rewards conformity, punishes dissent, and grows its legitimacy on a single premise it can never afford to question.
When a society hands a scientific institution the authority of religion—when criticism becomes heresy, when questioning becomes threat, when conclusions must be set before data is collected—it hasn’t elevated science. It’s replaced it with something that wears science’s clothing.
The faith is fracturing now. What gets built in its place—whether it’s something genuinely more honest or simply a new set of untouchable orthodoxies—is a question everyone paying attention is going to have to answer. Before we lose the opportunity.
@MidwesternDoc Thanks for reading! This information was based on a report originally published by @MidwesternDoc. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
midwesterndoctor.com/p/dissecting-t…
midwesterndoctor.com/p/dissecting-t…
@MidwesternDoc For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by @MidwesternDoc:
What They Don’t Tell Us About Anxiety and Benzodiazepine Dangers
midwesterndoctor.com/p/what-they-do…
What They Don’t Tell Us About Anxiety and Benzodiazepine Dangers
midwesterndoctor.com/p/what-they-do…
@MidwesternDoc The Hidden Dangers of Hospital Births & How to Protect Your Family
midwesterndoctor.com/p/the-hidden-d…
midwesterndoctor.com/p/the-hidden-d…
@MidwesternDoc While you’re at it, give @MidwesternDoc a follow.
No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed.
This is easily one of the most valuable accounts you’ll ever follow.
--> @MidwesternDoc
No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed.
This is easily one of the most valuable accounts you’ll ever follow.
--> @MidwesternDoc

• • •
Missing some Tweet in this thread? You can try to
force a refresh