Filtering the air may help prevent your own infection from becoming more severe
If everyone in a household becomes infected with the same virus, does it help to isolate from each other and can you be a danger to yourself? Read on to find out...🧵1/
#AirQuality #IAQ #Ventilation
If everyone in a household becomes infected with the same virus, does it help to isolate from each other and can you be a danger to yourself? Read on to find out...🧵1/
#AirQuality #IAQ #Ventilation
An interesting hypothesis-generating study was published recently that asked if an infected person's condition can become even worse by re-inhaling their own virus particles ( ). 2/sciencedirect.com/science/articl…
Is a transition from a milder upper respiratory tract infection (runny nose, sore throat) to a more severe lower respiratory tract infection like pneumonia is significantly driven by the physical mechanism of inhaling virus containing aerosols deep into the lungs? 3/
While a person may first become infected by breathing in virus aerosols generated by another infected person, the newly the infected individual exhales high concentrations of aerosols during peak viral shedding. 4/
If they are located in a poorly ventilated space, the aerosols accumulate and the person re-inhales their own virus, driving them deep into their own uninfected lung tissues. 5/
Instead of seeing tissue become infected in a cellular "crawling" pattern from a point where the infection spreads, COVID chest CT scans show rapid scattered patches of lung damage across distant isolated areas. 6/
Inhaled aerosols would act more like the wind scattering dandelion seeds across a large area simultaneously and better explain these CT scan results. 7/
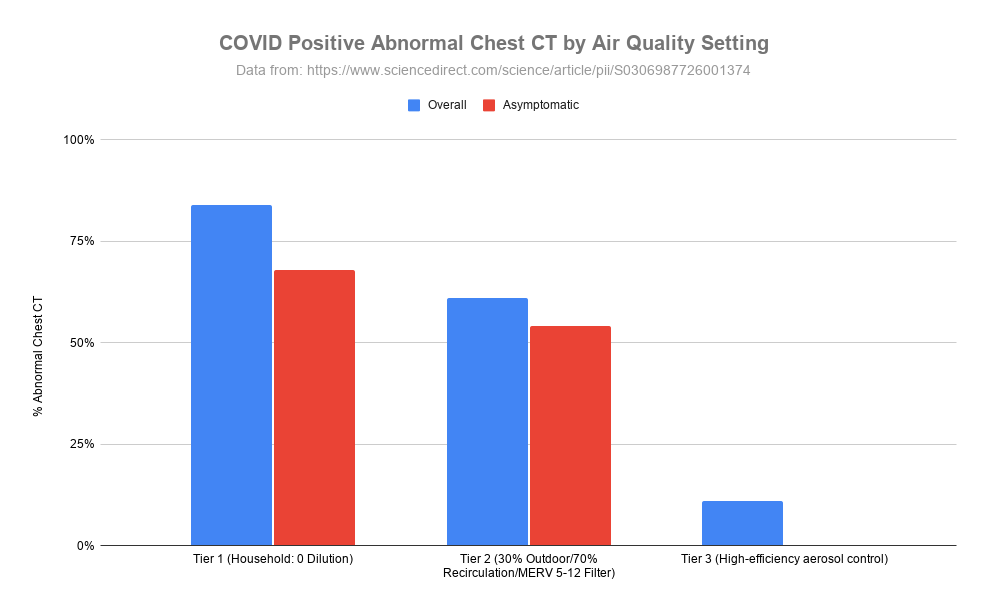
The researchers looked at chest CT scans from people that tested positive for COVID in three different tiers of ventilation quality. 8/
The first (Tier 1) were households and community areas with stagnant air, zero dilution and high accumulation. They found that 84% of the infected people who had chest CT scans overall and 68% of asymptomatic infections had abnormal CT scan results. 9/
In Tier 2 which had 30% fresh air, 70% re-circulated air and typical building filtration (MERV 5-12) the chest CT abnormality rate dropped to 61% overall and 54% for asymptomatic infections. 10/
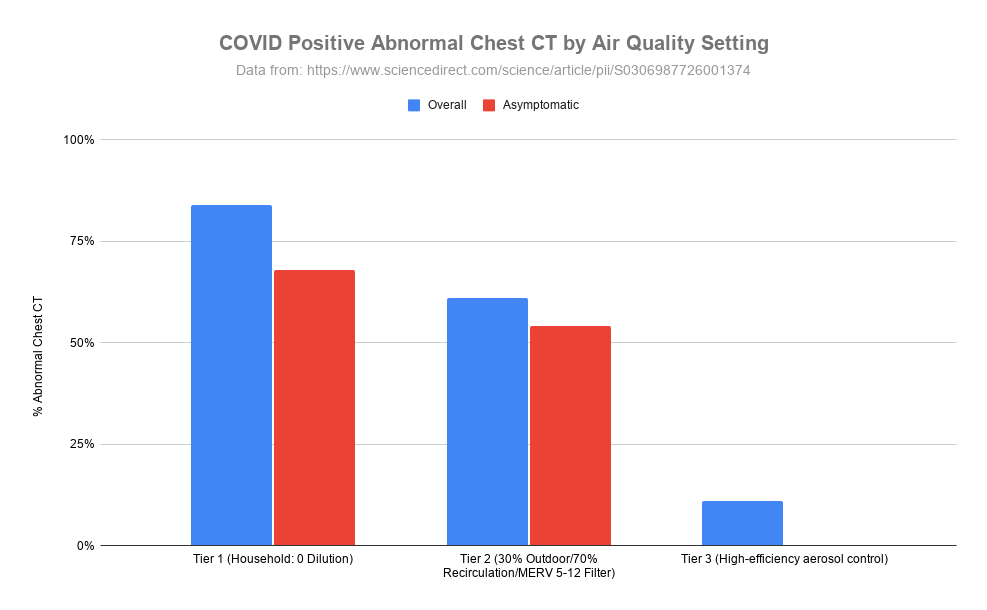
Finally, in Tier 3 where people were placed in individual negative-pressure rooms with rapid continuous air evacuation, only 11% of infected participants had chest CT abnormalities and those that did were tiny and very short lived. 11/
All participants in this high air quality group had very high viral loads in their throats and noses, but did not progress into lung damage. 12/
It is important to note that this study does not prove the hypothesis of an aerosol bridge linking upper respiratory infection to lung damage. Multiple convergent evidence is pointing more and more that this hypothesis is possible. 13/
In addition to human evidence, another study has shown with controlled COVID exposure in primates that inoculation via the intranasal route resulted in limited involvement in the lower respiratory tract... 14/
...whereas exposure to aerosols resulted in infection throughout the respiratory tract ( ). 15/academic.oup.com/jid/article/23…
If their hypothesis is true, improving air filtration and air quality not only protects others from catching your sickness but also helps protect you from your own sickness. 16/
Even without high end negative-pressure isolation rooms, it is possible to put an air filter close to our heads when sick to try and filter as much of what we are releasing in our own aerosols as possible to reduce the amount we are re-inhaling and others might be inhaling. 17/
Cleaning the air and improving ventilation could physically prevent mild cases from degrading into more severe illness including pneumonia. 18/
Since cleaning the air is a physical mechanism, it would be applicable to all pathogens that catch rides in aerosols including viruses and bacteria and not be impacted by pathogens mutating over time. 19/
The nice thing about this hypothesis is that even if we don't know definitively if true, cleaning the air has many benefits so worthwhile implementing whether this specific hypothesis is true or not. 20/
You can find out more about the importance of indoor air quality here ( pingthread.com/thread/1607379… ) more specifically about wildfire smoke and cooking here ( docs.google.com/document/d/1x0… ). 21/
A new webinar by Dr. Louise Hidinger, founder of Clean Indoor Air Toronto: Healthy Air at Home: What You Can Monitor, Filter, and Fix ( ) 22/
OSPE (Ontario Society of Professional Engineers) has a number of different indoor air quality reports here ( ). 23/ospe.on.ca/advocacy/gover…
UCDavid College of Engineering has a whole bunch of Indoor Air Quality videos here ( ). 24/iaq.ucdavis.edu/video-lessons/
Joey Fox has put together a collection of Indoor Air Quality educational pieces here ( ). 25/itsairborne.com/indoor-air-qua…
@threadreaderapp please unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh