⚠️‼️ I came across this news in Spain, and this discourse keeps doing enormous harm.
The post literally says:
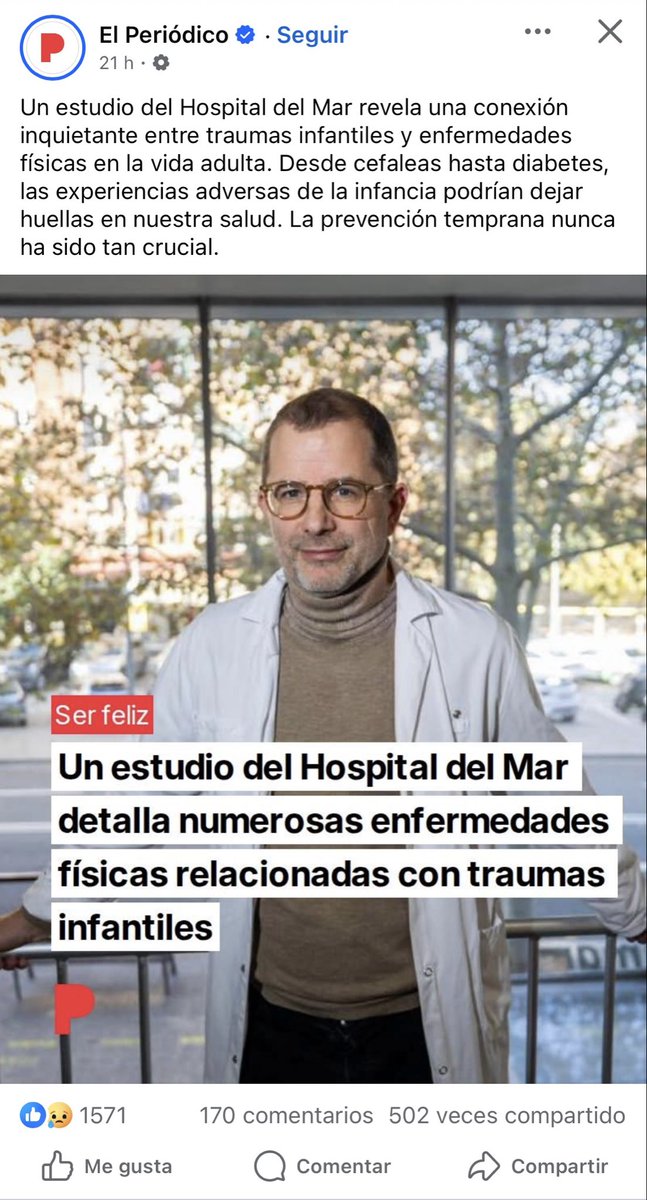
“A study from Hospital del Mar reveals a worrying connection between childhood trauma and physical diseases in adult life. From headaches to diabetes, adverse childhood experiences could leave marks on our health. Early prevention has never been so crucial.”
“A study from Hospital del Mar details numerous physical diseases linked to childhood trauma.”
Not because they literally said that most organic diseases are caused by childhood trauma, but because in practice, many of the diseases they attribute to or reduce to trauma end up being organic diseases whose biomarkers have not yet been discovered, or whose proper medical workup was never even done.
And that is the real problem.
For years, many patients are first filtered through the lens of trauma, psychosomatic illness, or somatization, when in reality what they have is an organic disease that has simply not yet been diagnosed. I would even go further and say that this also happens with diseases we now understand well: before reaching the right specialist and before the appropriate tests are performed, many patients are treated as if the origin of their symptoms were psychological or trauma-related, simply because nobody has investigated their case properly.
That is not precision medicine.
That is a way of covering diagnostic ignorance with a psychological narrative.
The history of medicine shows this again and again: many diseases that in their early stages were treated as “nervous,” “hysterical,” or “psychosomatic” later turned out to be well-defined organic diseases. This happened with multiple autoimmune, neurological, and inflammatory diseases. And it is still happening today.
That is why this discourse is so dangerous. Because it not only delays the real diagnosis, but also blames the patient, isolates them, sends them into the wrong clinical pathways, and steals years of serious medical investigation from them.
Most of these patients do not need their illness to be explained through trauma.
They need the right tests, the right specialist, and serious investigation of their real biology instead of convenient theories being projected onto them.
Enough of turning the absence of known biomarkers into a psychological explanation.
What some people today call trauma or somatization too often ends up tomorrow having a name, a mechanism, and a biological marker.
The post literally says:
“A study from Hospital del Mar reveals a worrying connection between childhood trauma and physical diseases in adult life. From headaches to diabetes, adverse childhood experiences could leave marks on our health. Early prevention has never been so crucial.”
“A study from Hospital del Mar details numerous physical diseases linked to childhood trauma.”
Not because they literally said that most organic diseases are caused by childhood trauma, but because in practice, many of the diseases they attribute to or reduce to trauma end up being organic diseases whose biomarkers have not yet been discovered, or whose proper medical workup was never even done.
And that is the real problem.
For years, many patients are first filtered through the lens of trauma, psychosomatic illness, or somatization, when in reality what they have is an organic disease that has simply not yet been diagnosed. I would even go further and say that this also happens with diseases we now understand well: before reaching the right specialist and before the appropriate tests are performed, many patients are treated as if the origin of their symptoms were psychological or trauma-related, simply because nobody has investigated their case properly.
That is not precision medicine.
That is a way of covering diagnostic ignorance with a psychological narrative.
The history of medicine shows this again and again: many diseases that in their early stages were treated as “nervous,” “hysterical,” or “psychosomatic” later turned out to be well-defined organic diseases. This happened with multiple autoimmune, neurological, and inflammatory diseases. And it is still happening today.
That is why this discourse is so dangerous. Because it not only delays the real diagnosis, but also blames the patient, isolates them, sends them into the wrong clinical pathways, and steals years of serious medical investigation from them.
Most of these patients do not need their illness to be explained through trauma.
They need the right tests, the right specialist, and serious investigation of their real biology instead of convenient theories being projected onto them.
Enough of turning the absence of known biomarkers into a psychological explanation.
What some people today call trauma or somatization too often ends up tomorrow having a name, a mechanism, and a biological marker.
• • •
Missing some Tweet in this thread? You can try to
force a refresh