
🔬Diving deep into #MECFS, #LongCOVID, #LongEBV & post-vaccine syndrome research. Dual role:Researcher and EBV ME/CFS patient. Seeking answers. #Antivirals #HLA
 ▪️ ME/CFS: the same model, but with other pathogens
▪️ ME/CFS: the same model, but with other pathogens 2/ This leads to the second major difference: the role of CD4 cells. In HIV/AIDS, the central problem is that CD4 cells are progressively lost. In Long COVID and ME/CFS, CD4 cells are not usually the compartment being massively destroyed as the main axis of the disease. On the contrary, in many patients they may continue contributing to the pathology, sustaining inflammation, helping autoreactive B cells, and favoring autoimmune responses. That is why, whereas HIV progresses toward immunodeficiency through depletion, Long COVID/ME/CFS fit much better with chronic immune activation + functional exhaustion + autoimmunity.
2/ This leads to the second major difference: the role of CD4 cells. In HIV/AIDS, the central problem is that CD4 cells are progressively lost. In Long COVID and ME/CFS, CD4 cells are not usually the compartment being massively destroyed as the main axis of the disease. On the contrary, in many patients they may continue contributing to the pathology, sustaining inflammation, helping autoreactive B cells, and favoring autoimmune responses. That is why, whereas HIV progresses toward immunodeficiency through depletion, Long COVID/ME/CFS fit much better with chronic immune activation + functional exhaustion + autoimmunity. 1️⃣ Cold changes how our immune system protects mucosal surfaces.
1️⃣ Cold changes how our immune system protects mucosal surfaces.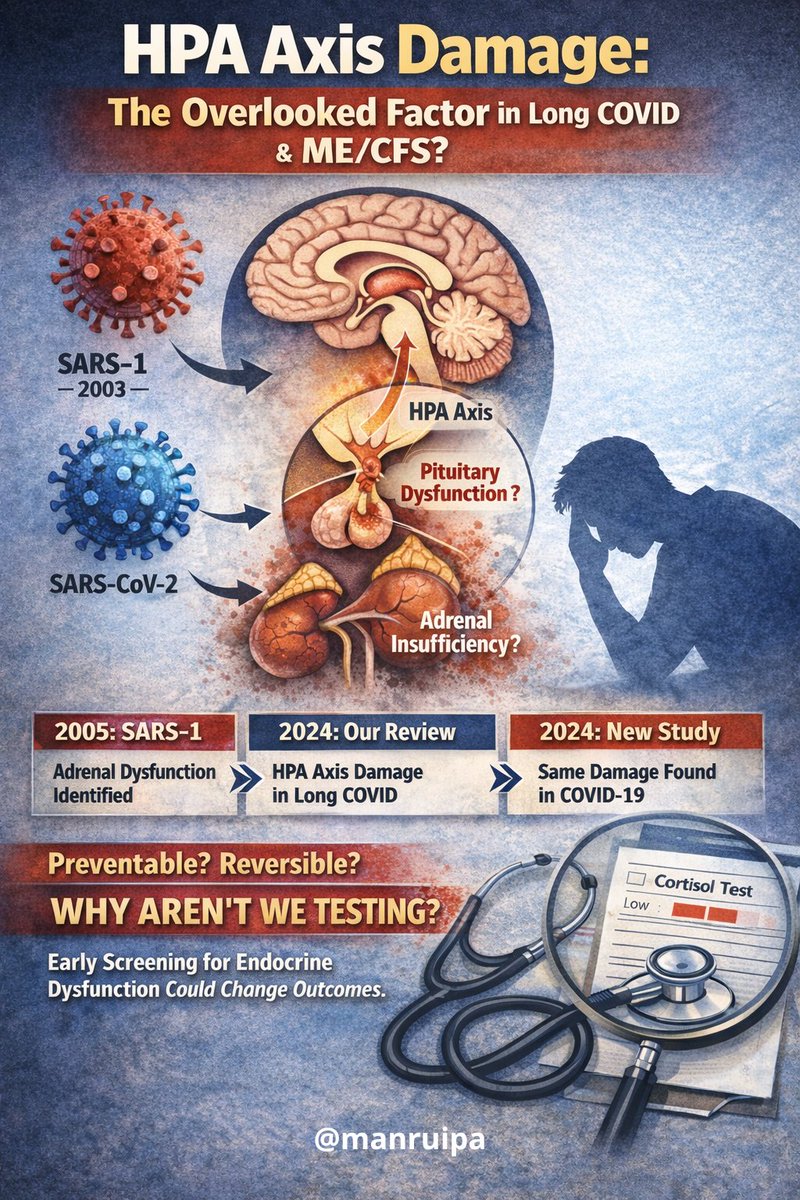 1️⃣ HPA axis damage in Long COVID and ME/CFS is not new. We’ve seen this before.
1️⃣ HPA axis damage in Long COVID and ME/CFS is not new. We’ve seen this before. 1) Why does anti-M3 matter?
1) Why does anti-M3 matter? 1)🔴 New evidence
1)🔴 New evidence 2️⃣ Don’t feel ashamed to:
2️⃣ Don’t feel ashamed to: 📢 𝐖𝐡𝐲 𝐕𝐚𝐜𝐜𝐢𝐧𝐞𝐬 𝐂𝐚𝐧 𝐃𝐞𝐯𝐞𝐥𝐨𝐩 𝐏𝐚𝐭𝐡𝐨𝐥𝐨𝐠𝐢𝐞𝐬 𝐒𝐢𝐦𝐢𝐥𝐚𝐫 𝐭𝐨 𝐏𝐞𝐫𝐬𝐢𝐬𝐭𝐞𝐧𝐭 𝐂𝐎𝐕𝐈𝐃 𝐚𝐧𝐝 𝐏𝐨𝐬𝐭-𝐈𝐧𝐟𝐞𝐜𝐭𝐢𝐨𝐮𝐬 𝐌𝐄/𝐂𝐅𝐒? 📢
📢 𝐖𝐡𝐲 𝐕𝐚𝐜𝐜𝐢𝐧𝐞𝐬 𝐂𝐚𝐧 𝐃𝐞𝐯𝐞𝐥𝐨𝐩 𝐏𝐚𝐭𝐡𝐨𝐥𝐨𝐠𝐢𝐞𝐬 𝐒𝐢𝐦𝐢𝐥𝐚𝐫 𝐭𝐨 𝐏𝐞𝐫𝐬𝐢𝐬𝐭𝐞𝐧𝐭 𝐂𝐎𝐕𝐈𝐃 𝐚𝐧𝐝 𝐏𝐨𝐬𝐭-𝐈𝐧𝐟𝐞𝐜𝐭𝐢𝐨𝐮𝐬 𝐌𝐄/𝐂𝐅𝐒? 📢
 1/La diversidad de microbiota varía entre personas, lo que hace imposible obtener resultados consistentes de los test de microbiota. No se sabe cuál es la microbiota normal. #Microbiota #SIBO #LongEBV #microE2324
1/La diversidad de microbiota varía entre personas, lo que hace imposible obtener resultados consistentes de los test de microbiota. No se sabe cuál es la microbiota normal. #Microbiota #SIBO #LongEBV #microE2324
 𝐃𝐨𝐞𝐬 𝐭𝐡𝐢𝐬 𝐦𝐨𝐝𝐞𝐥 𝐞𝐱𝐩𝐥𝐚𝐢𝐧 𝐭𝐡𝐞 𝐨𝐜𝐜𝐮𝐫𝐫𝐞𝐧𝐜𝐞 𝐨𝐟 𝐝𝐢𝐠𝐞𝐬𝐭𝐢𝐯𝐞 𝐩𝐫𝐨𝐛𝐥𝐞𝐦𝐬, 𝐟𝐨𝐨𝐝 𝐢𝐧𝐭𝐨𝐥𝐞𝐫𝐚𝐧𝐜𝐞𝐬 𝐚𝐧𝐝 𝐚𝐥𝐭𝐞𝐫𝐚𝐭𝐢𝐨𝐧𝐬 𝐢𝐧 𝐭𝐡𝐞 𝐦𝐢𝐜𝐫𝐨𝐛𝐢𝐨𝐭𝐚 𝐢𝐧 𝐭𝐡𝐞𝐬𝐞 𝐩𝐚𝐭𝐢𝐞𝐧𝐭𝐬?
𝐃𝐨𝐞𝐬 𝐭𝐡𝐢𝐬 𝐦𝐨𝐝𝐞𝐥 𝐞𝐱𝐩𝐥𝐚𝐢𝐧 𝐭𝐡𝐞 𝐨𝐜𝐜𝐮𝐫𝐫𝐞𝐧𝐜𝐞 𝐨𝐟 𝐝𝐢𝐠𝐞𝐬𝐭𝐢𝐯𝐞 𝐩𝐫𝐨𝐛𝐥𝐞𝐦𝐬, 𝐟𝐨𝐨𝐝 𝐢𝐧𝐭𝐨𝐥𝐞𝐫𝐚𝐧𝐜𝐞𝐬 𝐚𝐧𝐝 𝐚𝐥𝐭𝐞𝐫𝐚𝐭𝐢𝐨𝐧𝐬 𝐢𝐧 𝐭𝐡𝐞 𝐦𝐢𝐜𝐫𝐨𝐛𝐢𝐨𝐭𝐚 𝐢𝐧 𝐭𝐡𝐞𝐬𝐞 𝐩𝐚𝐭𝐢𝐞𝐧𝐭𝐬?
 Este modelo explica la aparición de problemas digestivos, intolerancias alimentarias y alteraciones en la microbiota en estos pacientes?
Este modelo explica la aparición de problemas digestivos, intolerancias alimentarias y alteraciones en la microbiota en estos pacientes?
 1/ 🤔 𝐈𝐧𝐭𝐫𝐨𝐝𝐮𝐜𝐭𝐢𝐨𝐧: ME/CFS and Long COVID are two pathologies that, although arising from different causes, present astonishing similarities in how they affect the body and their symptoms. #MyalgicEncephalomyelitis #COVIDSurvivors
1/ 🤔 𝐈𝐧𝐭𝐫𝐨𝐝𝐮𝐜𝐭𝐢𝐨𝐧: ME/CFS and Long COVID are two pathologies that, although arising from different causes, present astonishing similarities in how they affect the body and their symptoms. #MyalgicEncephalomyelitis #COVIDSurvivors
 …Myalgic Encephalomyelitis and Long COVID. But it is still unclear what pathways it uses.
…Myalgic Encephalomyelitis and Long COVID. But it is still unclear what pathways it uses.