Magnesium has the ability to shrink arterial plaques, demonstrated by some incredible clinical trials.
(🧵1/8)
(🧵1/8)
https://x.com/Outdoctrination/status/1977744364244812001

This first study came out in 2008.
They gave people magnesium citrate, just under 100 mg elemental magnesium per day.
This is a puny dose, magnesium RDA is 4X that and people often supplement even more than that.
These studies are all in hemodialysis patients, and that's mainly because these people develop heart disease at a much quicker rate due to toxin accumulation and altered mineral balance.
They gave people magnesium citrate, just under 100 mg elemental magnesium per day.
This is a puny dose, magnesium RDA is 4X that and people often supplement even more than that.
These studies are all in hemodialysis patients, and that's mainly because these people develop heart disease at a much quicker rate due to toxin accumulation and altered mineral balance.
Magnesium reduced plaque burden within 2 months.
Carotid intima median thickness (cIMT) is the literal thickness of the inner part of the arteries. It's a direct measurement of plaque buildup.
This was decreased on both the left and right sides, while plaque sizes tended to INCREASE without it.
Carotid intima median thickness (cIMT) is the literal thickness of the inner part of the arteries. It's a direct measurement of plaque buildup.
This was decreased on both the left and right sides, while plaque sizes tended to INCREASE without it.
There was also a decent correlation between serum magnesium levels and plaque size.
More magnesium = less plaque.
Serum magnesium is not the best overall measure, and it mainly becomes low in severe depletion.
More magnesium = less plaque.
Serum magnesium is not the best overall measure, and it mainly becomes low in severe depletion.

The second paper came out in 2013.
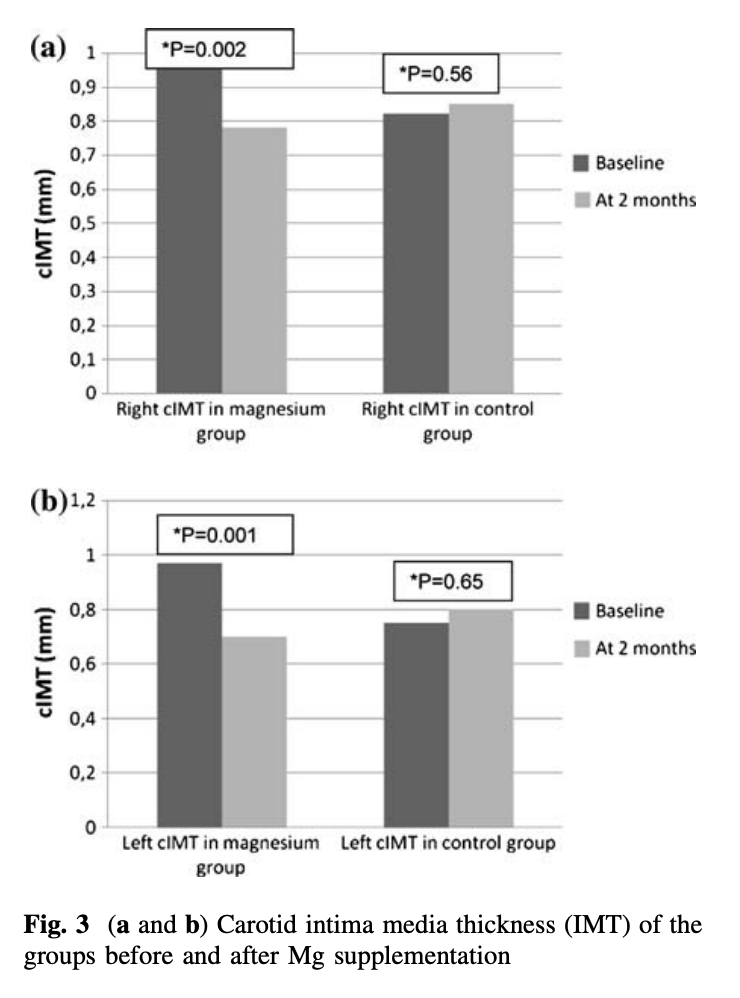
This time patients were given 440 mg of magnesium oxide 3x per week for 6 months.
Magnesium oxide is a terrible form of magnesium, with as little as 4% of it getting absorbed in the gut.
So really, this is a small, small amount of magnesium.
This time patients were given 440 mg of magnesium oxide 3x per week for 6 months.
Magnesium oxide is a terrible form of magnesium, with as little as 4% of it getting absorbed in the gut.
So really, this is a small, small amount of magnesium.

Even still, after 6 months, people taking the magnesium showed improvements in plaque thickness.
Both the left and right thicknesses were decreased, resulting in a total drop of plaque size.
Meanwhile, the placebo group saw plaques grow once again.
Both the left and right thicknesses were decreased, resulting in a total drop of plaque size.
Meanwhile, the placebo group saw plaques grow once again.

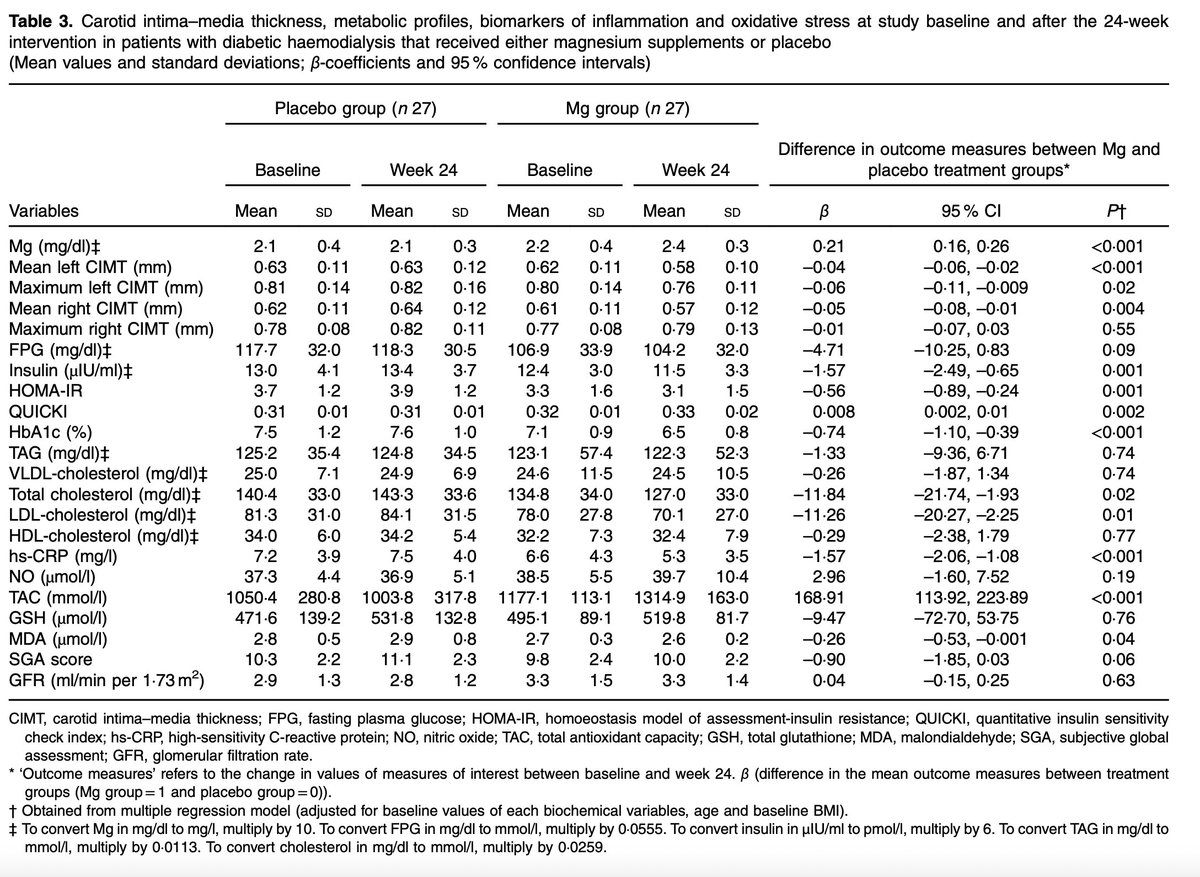
Another study published in 2019 showed even better effects.
Again, the poorly absorbed magnesium oxide, at just 150 mg of elemental magnesium per day, showed beneficial effects across the board.
Vascular:
↓ Mean left CIMT
↓ Maximum left CIMT
↓ Mean right CIMT
Glycemic / Insulin sensitivity:
↓ Insulin
↓ HOMA-IR
↑ QUICKI (insulin sensitivity)
↓ HbA1c
Lipids:
↓ Total cholesterol
↓ LDL cholesterol
Inflammation & oxidative stress:
↓ hs-CRP
↑ Total antioxidant capacity (TAC)
↓ MDA (lipid peroxidation marker)
Again, the poorly absorbed magnesium oxide, at just 150 mg of elemental magnesium per day, showed beneficial effects across the board.
Vascular:
↓ Mean left CIMT
↓ Maximum left CIMT
↓ Mean right CIMT
Glycemic / Insulin sensitivity:
↓ Insulin
↓ HOMA-IR
↑ QUICKI (insulin sensitivity)
↓ HbA1c
Lipids:
↓ Total cholesterol
↓ LDL cholesterol
Inflammation & oxidative stress:
↓ hs-CRP
↑ Total antioxidant capacity (TAC)
↓ MDA (lipid peroxidation marker)
How is magnesium so effective for heart disease?
Countless reasons, really, but a few of the most important.
1. Anti-inflammatory properties. Magnesium has been shown to alleviate various inflammatory conditions, and heart disease is no exception. The entire plaque formation process is an active construction by the immune system, not just a passive building up of lipids.
2. Metabolism. Magnesium is probably the single most important nutrient for the mitochondria, being involved in countless reactions in energy metabolism and needed for ATP synthesis. Mitochondrial function is needed to stop the inflammatory process and facilitate the export of cholesterol from the arteries.
3. Antioxidant properties. The core initiating event in atherosclerosis is oxidative stress that damages lipoproteins. Magnesium is critical in maintaining antioxidant defenses.
4. NO synthesis / endothelial function. Magnesium is incredibly important for this layer of cells in the arteries. When endothelial cells do not function correctly, they become more permeable to cholesterol entering the arteries.
5. Lipid lowering. Magnesium also has shown the ability to directly lower cholesterol and other lipids, through various mechanisms. Without enough magnesium, cholesterol cannot be cleared from the blood, metabolized or have its synthesis shut off properly.
Countless reasons, really, but a few of the most important.
1. Anti-inflammatory properties. Magnesium has been shown to alleviate various inflammatory conditions, and heart disease is no exception. The entire plaque formation process is an active construction by the immune system, not just a passive building up of lipids.
2. Metabolism. Magnesium is probably the single most important nutrient for the mitochondria, being involved in countless reactions in energy metabolism and needed for ATP synthesis. Mitochondrial function is needed to stop the inflammatory process and facilitate the export of cholesterol from the arteries.
3. Antioxidant properties. The core initiating event in atherosclerosis is oxidative stress that damages lipoproteins. Magnesium is critical in maintaining antioxidant defenses.
4. NO synthesis / endothelial function. Magnesium is incredibly important for this layer of cells in the arteries. When endothelial cells do not function correctly, they become more permeable to cholesterol entering the arteries.
5. Lipid lowering. Magnesium also has shown the ability to directly lower cholesterol and other lipids, through various mechanisms. Without enough magnesium, cholesterol cannot be cleared from the blood, metabolized or have its synthesis shut off properly.

My preferred magnesium brand (affiliate) is here, two highly absorbable forms at much higher doses than what is used in these studies. analyzeandoptimize.io/shop#magnesium
• • •
Missing some Tweet in this thread? You can try to
force a refresh