I got a message last month from a 29 year old athlete.
He had been clinically dead in an ambulance 4 weeks earlier. Full cardiac arrest. 100% blocked LAD. The widow maker.
Resuscitated. Stented. Survived.
His cholesterol was low. His Lp(a) was 10. Every marker the system trusts said he was perfectly healthy.
This thread is about what actually caused his heart attack. And 5 hidden killers in young, fit people that your doctor will never test for.
He had been clinically dead in an ambulance 4 weeks earlier. Full cardiac arrest. 100% blocked LAD. The widow maker.
Resuscitated. Stented. Survived.
His cholesterol was low. His Lp(a) was 10. Every marker the system trusts said he was perfectly healthy.
This thread is about what actually caused his heart attack. And 5 hidden killers in young, fit people that your doctor will never test for.

He eats wild caught fish he catches himself. Seasonal game he hunts. Grows his own food.
No alcohol. No drugs. No supplements. No processed food.
If he cannot hunt it or grow it, he does not eat it.
Look at him and you would never suspect a cardiac event was possible. His doctor would never suspect it either.
That is the problem.
No alcohol. No drugs. No supplements. No processed food.
If he cannot hunt it or grow it, he does not eat it.
Look at him and you would never suspect a cardiac event was possible. His doctor would never suspect it either.
That is the problem.

His fasted lipid panel after the event.
Triglycerides: 47.
HDL: 101.
LDL: 118.
Lp(a): 10.
Trig to HDL ratio: 0.47.
Anything below 1.0 is world class metabolic health. He is at 0.47.
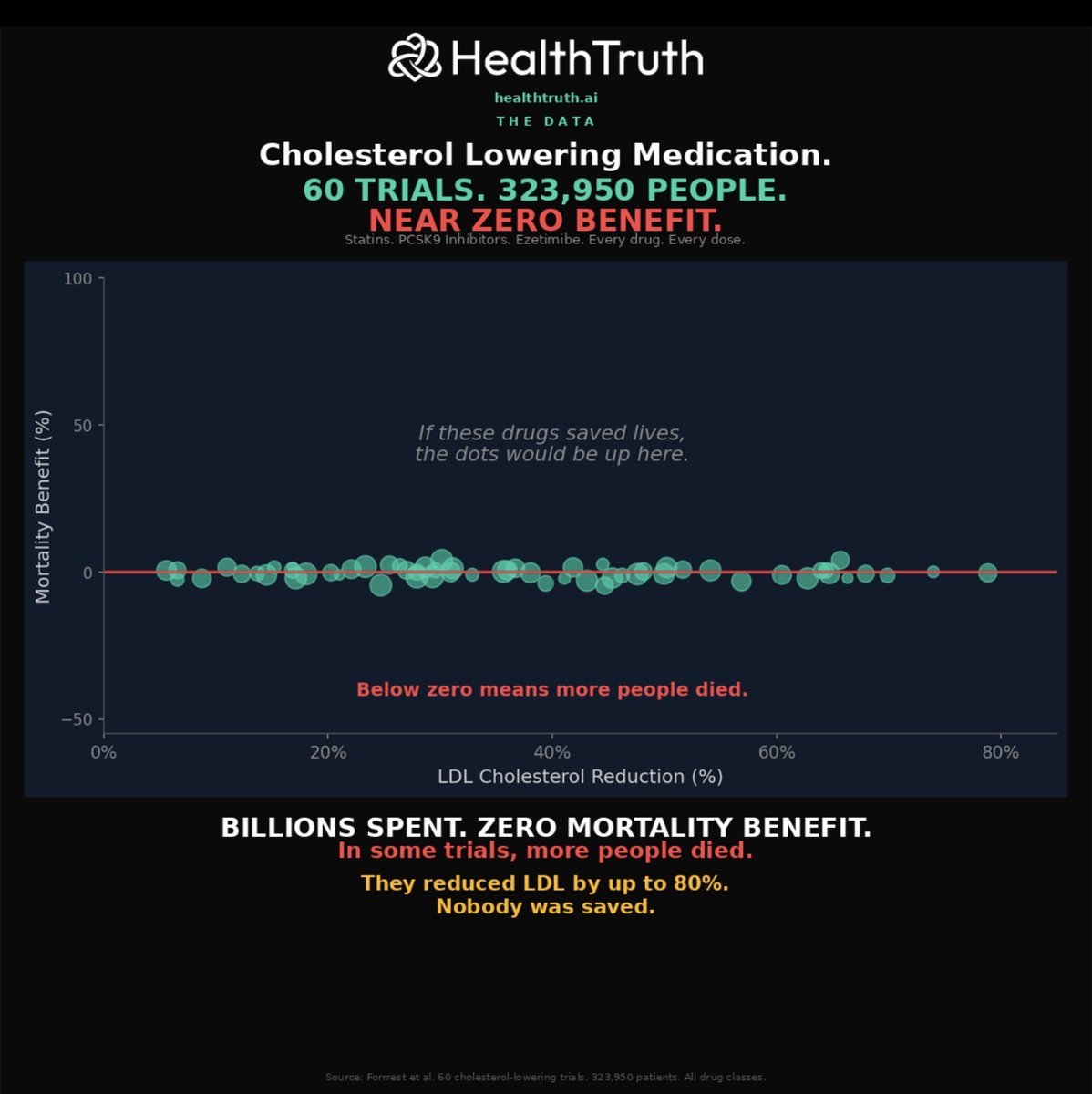
His doctor saw total cholesterol at 233 and reached for a statin.
The cholesterol paradigm had zero predictive power. Zero.
Triglycerides: 47.
HDL: 101.
LDL: 118.
Lp(a): 10.
Trig to HDL ratio: 0.47.
Anything below 1.0 is world class metabolic health. He is at 0.47.
His doctor saw total cholesterol at 233 and reached for a statin.
The cholesterol paradigm had zero predictive power. Zero.
So he ran the tests his doctors never ordered.
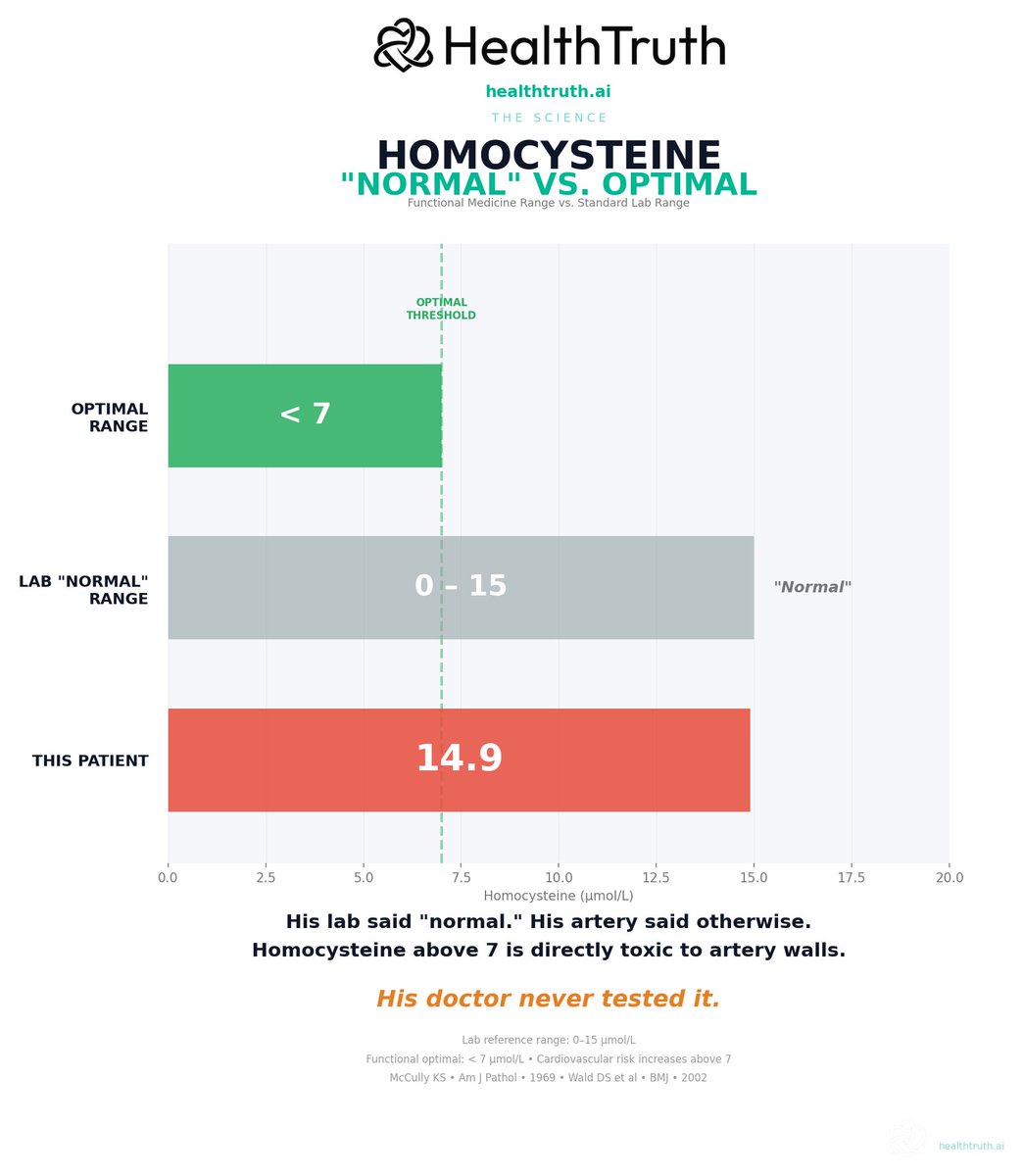
Homocysteine: 14.9.
The lab range goes up to 15 so his doctor would call it "normal." He scraped in by 0.1.
Functional optimal is below 7. He was double that.
Homocysteine is not a bystander marker. It is directly toxic to the lining of arteries. It damages the artery wall silently, without raising CRP, without triggering any alarm the system monitors.
His artery wall was being chemically destroyed for years. His cholesterol sat there doing nothing.
Homocysteine: 14.9.
The lab range goes up to 15 so his doctor would call it "normal." He scraped in by 0.1.
Functional optimal is below 7. He was double that.
Homocysteine is not a bystander marker. It is directly toxic to the lining of arteries. It damages the artery wall silently, without raising CRP, without triggering any alarm the system monitors.
His artery wall was being chemically destroyed for years. His cholesterol sat there doing nothing.
Factor VIII activity: 143.3. Normal range tops out at 150.
But here is the tell. His hs-CRP was already back to 0.2. The inflammatory spike from the heart attack had fully resolved.
Factor VIII had not come down with it.
If it was elevated because of the MI, it should have dropped alongside CRP. It did not. That means 143 is likely his baseline. His blood has been hypercoagulable his entire life. Nobody tested it. Nobody knew.
A minor plaque crack that would self-heal in most people became a total artery occlusion in minutes. Two causes stacking. One damaged the wall. The other sealed it shut.
But here is the tell. His hs-CRP was already back to 0.2. The inflammatory spike from the heart attack had fully resolved.
Factor VIII had not come down with it.
If it was elevated because of the MI, it should have dropped alongside CRP. It did not. That means 143 is likely his baseline. His blood has been hypercoagulable his entire life. Nobody tested it. Nobody knew.
A minor plaque crack that would self-heal in most people became a total artery occlusion in minutes. Two causes stacking. One damaged the wall. The other sealed it shut.

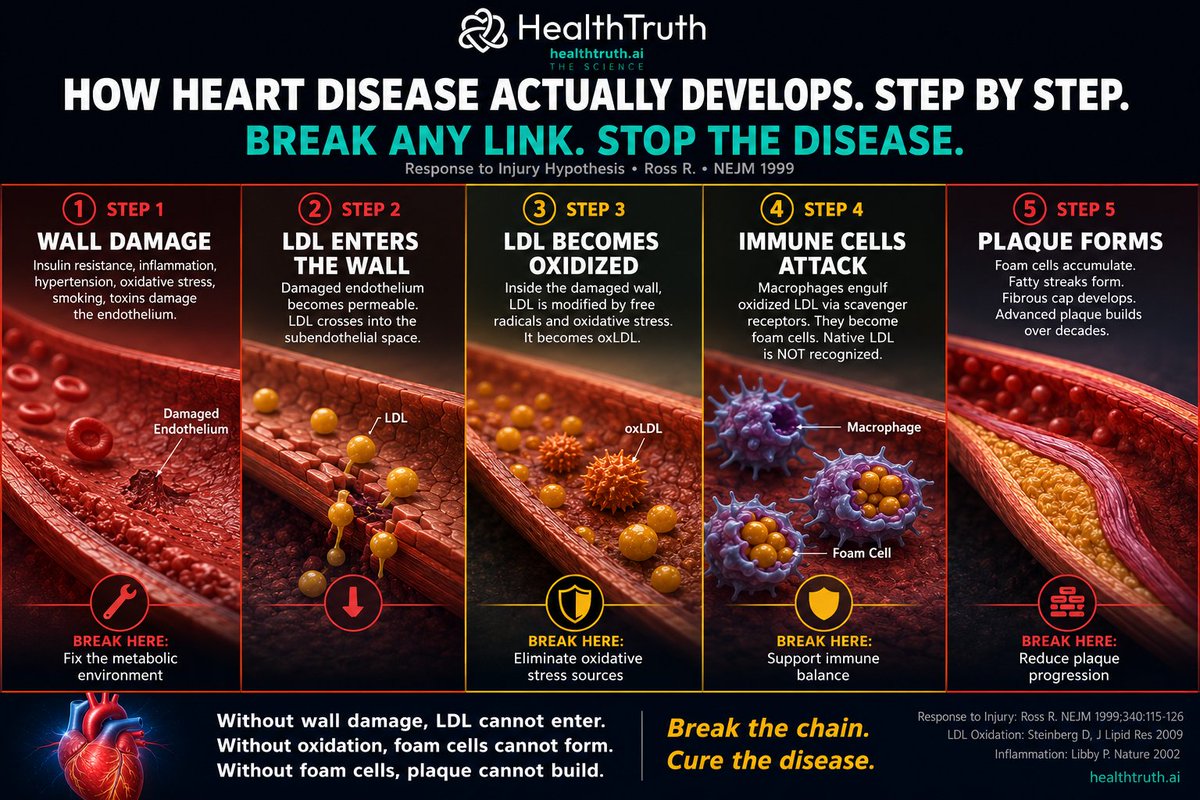
Hidden Killer #1: MTHFR.
Roughly 40 to 60 percent of all humans carry at least one copy of this gene variant. It reduces the body's ability to convert folate into its active form, methylfolate.
Without enough methylfolate, homocysteine cannot be cleared from the blood. It accumulates. It poisons the artery wall year after year.
No CRP signal. No cholesterol spike. No warning.
His ancestors carried this same gene for 10,000 years and never had heart attacks at 29.
The gene did not change. The environment changed.
Roughly 40 to 60 percent of all humans carry at least one copy of this gene variant. It reduces the body's ability to convert folate into its active form, methylfolate.
Without enough methylfolate, homocysteine cannot be cleared from the blood. It accumulates. It poisons the artery wall year after year.
No CRP signal. No cholesterol spike. No warning.
His ancestors carried this same gene for 10,000 years and never had heart attacks at 29.
The gene did not change. The environment changed.
His ancestors ate nose to tail. Liver, kidney, heart, brain. The richest sources of bioavailable folate on earth.
They ate whole fish. Head, liver, roe. They fermented their food. They lived in a clean environment with low toxin exposure.
The MTHFR enzyme running at half capacity did not matter because the folate input was massive. Enough methylfolate got through.
Modern life flipped every variable. Muscle meat only. Fish fillets only. Mercury in the water. Chemicals demanding more methylation than ever.
Same gene. Opposite environment. Different outcome.
You cannot out-eat a methylation defect with a modern diet. Even the cleanest one on earth.
They ate whole fish. Head, liver, roe. They fermented their food. They lived in a clean environment with low toxin exposure.
The MTHFR enzyme running at half capacity did not matter because the folate input was massive. Enough methylfolate got through.
Modern life flipped every variable. Muscle meat only. Fish fillets only. Mercury in the water. Chemicals demanding more methylation than ever.
Same gene. Opposite environment. Different outcome.
You cannot out-eat a methylation defect with a modern diet. Even the cleanest one on earth.
Hidden Killer #2: Your "healthy" diet may be poisoning you.
He eats wild caught fish as his primary protein year round. That is supposed to be one of the healthiest diets a human can eat.
But modern fish carry mercury. Mercury is directly toxic to the endothelial lining of arteries. It depletes selenium, which the body needs both to protect itself from mercury AND to convert thyroid hormone from T4 to T3.
His T3 was below range. His body was showing signs of being quietly poisoned by the very food that was supposed to save him.
Nobody tested his mercury. Nobody tested his selenium. They tested his cholesterol.
He eats wild caught fish as his primary protein year round. That is supposed to be one of the healthiest diets a human can eat.
But modern fish carry mercury. Mercury is directly toxic to the endothelial lining of arteries. It depletes selenium, which the body needs both to protect itself from mercury AND to convert thyroid hormone from T4 to T3.
His T3 was below range. His body was showing signs of being quietly poisoned by the very food that was supposed to save him.
Nobody tested his mercury. Nobody tested his selenium. They tested his cholesterol.
Hidden Killer #3: Clotting disorders.
Factor V Leiden. Prothrombin mutation. Antiphospholipid syndrome. Elevated Factor VIII.
These are inherited conditions that make your blood clot too aggressively. Millions of people carry them and will never know.
A minor plaque crack that your body would normally patch and move on from becomes a total blockage. A small tear becomes a fatal event.
The standard cardiac workup does not include a clotting panel. It includes a cholesterol panel.
Factor V Leiden. Prothrombin mutation. Antiphospholipid syndrome. Elevated Factor VIII.
These are inherited conditions that make your blood clot too aggressively. Millions of people carry them and will never know.
A minor plaque crack that your body would normally patch and move on from becomes a total blockage. A small tear becomes a fatal event.
The standard cardiac workup does not include a clotting panel. It includes a cholesterol panel.
Hidden Killer #4: SCAD.
Spontaneous coronary artery dissection. The inner wall of the artery tears on its own. Blood forces between the layers and squeezes the channel shut from the inside.
No plaque. No buildup. No cholesterol involved.
It is the most common cause of heart attacks in young women and fit people under 50 with clean lipids. Often triggered by extreme exertion.
Cholesterol testing cannot catch it. Because cholesterol was never the problem. The wall was.
Spontaneous coronary artery dissection. The inner wall of the artery tears on its own. Blood forces between the layers and squeezes the channel shut from the inside.
No plaque. No buildup. No cholesterol involved.
It is the most common cause of heart attacks in young women and fit people under 50 with clean lipids. Often triggered by extreme exertion.
Cholesterol testing cannot catch it. Because cholesterol was never the problem. The wall was.
Hidden Killer #5: The gene-environment mismatch you do not know you have.
You can eat clean, train hard, sleep well, avoid alcohol, avoid processed food, and still carry a genetic vulnerability that your environment is not supporting.
MTHFR needs methylfolate your modern diet does not provide.
Clotting genes need monitoring your doctor does not order.
Mercury needs selenium your body is not getting.
Artery walls need nutrients your "healthy" diet may be missing.
Your genes evolved in one world. You live in another. The gap between them is where disease hides.
You can eat clean, train hard, sleep well, avoid alcohol, avoid processed food, and still carry a genetic vulnerability that your environment is not supporting.
MTHFR needs methylfolate your modern diet does not provide.
Clotting genes need monitoring your doctor does not order.
Mercury needs selenium your body is not getting.
Artery walls need nutrients your "healthy" diet may be missing.
Your genes evolved in one world. You live in another. The gap between them is where disease hides.
There is one more thing. He had been under significant stress for years.
This matters more than most people realize. Chronic stress does not just feel bad. It changes your biology.
Sustained cortisol increases clotting tendency. It raises blood pressure, which increases shear stress on artery walls. The proximal LAD takes more hemodynamic force than any other coronary artery. It is always ground zero.
Cortisol also drives homocysteine production by increasing methylation demand. The same methylation cycle that was already compromised by his MTHFR mutation was being pushed even harder by chronic stress.
Homocysteine was damaging the wall. Factor VIII was making his blood hypercoagulable. Stress was accelerating both.
The plaque did not rupture randomly. It ruptured because every system was loaded. Genetics set the trap. Stress pulled the trigger.
This matters more than most people realize. Chronic stress does not just feel bad. It changes your biology.
Sustained cortisol increases clotting tendency. It raises blood pressure, which increases shear stress on artery walls. The proximal LAD takes more hemodynamic force than any other coronary artery. It is always ground zero.
Cortisol also drives homocysteine production by increasing methylation demand. The same methylation cycle that was already compromised by his MTHFR mutation was being pushed even harder by chronic stress.
Homocysteine was damaging the wall. Factor VIII was making his blood hypercoagulable. Stress was accelerating both.
The plaque did not rupture randomly. It ruptured because every system was loaded. Genetics set the trap. Stress pulled the trigger.
This is why genetics is not optional. It is foundational.
A 29 year old athlete with perfect lipids nearly died because nobody matched his genetics to his environment. Nobody screened the high risk markers that would have caught this years before the event.
Not cholesterol. Homocysteine. Clotting factors. Methylation. Thyroid conversion. Toxic load. Nutrient status.
This is exactly why I built Neo. To screen every one of these markers. To catch the patterns that the standard system was never designed to find.
If we had seen this young man's bloodwork two years ago, we would have flagged the homocysteine. We would have flagged the Factor VIII. We would have tested MTHFR. We would have connected his fish-heavy diet to mercury and selenium.
He would never have been in that ambulance.
That is what prevention looks like. Not a statin for a number that was never broken. A complete picture of your genetics, your environment, and the gap between them.
A 29 year old athlete with perfect lipids nearly died because nobody matched his genetics to his environment. Nobody screened the high risk markers that would have caught this years before the event.
Not cholesterol. Homocysteine. Clotting factors. Methylation. Thyroid conversion. Toxic load. Nutrient status.
This is exactly why I built Neo. To screen every one of these markers. To catch the patterns that the standard system was never designed to find.
If we had seen this young man's bloodwork two years ago, we would have flagged the homocysteine. We would have flagged the Factor VIII. We would have tested MTHFR. We would have connected his fish-heavy diet to mercury and selenium.
He would never have been in that ambulance.
That is what prevention looks like. Not a statin for a number that was never broken. A complete picture of your genetics, your environment, and the gap between them.
A 29 year old athlete is alive today because an ambulance reached him in time.
Not because the system caught his risk. Not because his doctor tested the right things. Not because his cholesterol was monitored.
He survived by luck. Then he survived by asking better questions.
The system gave him a clean bill of health and a statin prescription. The root cause investigation gave him answers.
Same patient. Same genes. Different questions. Different outcome.
If you are young, fit, and doing everything right, do not assume you are safe. Ask for the tests on this list. The ones that saved him are the ones his doctor never ordered.
Not because the system caught his risk. Not because his doctor tested the right things. Not because his cholesterol was monitored.
He survived by luck. Then he survived by asking better questions.
The system gave him a clean bill of health and a statin prescription. The root cause investigation gave him answers.
Same patient. Same genes. Different questions. Different outcome.
If you are young, fit, and doing everything right, do not assume you are safe. Ask for the tests on this list. The ones that saved him are the ones his doctor never ordered.

Mark Kaplan
Founder, HealthTruth
Heart attack survivor. Zero drugs. Healthier at 58 than 40.
Co-founders of Neo | HealthTruth
Dr. Philip Ovadia, Cardiac Surgeon @ifixhearts
Dr. Aseem Malhotra, Cardiologist @DrAseemMalhotra
Dr. Robert Cywes, Metabolic Surgeon @carbaddictiondr
Prof. Tim Noakes, Head of Science @ProfTimNoakes
The truth heals
Founder, HealthTruth
Heart attack survivor. Zero drugs. Healthier at 58 than 40.
Co-founders of Neo | HealthTruth
Dr. Philip Ovadia, Cardiac Surgeon @ifixhearts
Dr. Aseem Malhotra, Cardiologist @DrAseemMalhotra
Dr. Robert Cywes, Metabolic Surgeon @carbaddictiondr
Prof. Tim Noakes, Head of Science @ProfTimNoakes
The truth heals
• • •
Missing some Tweet in this thread? You can try to
force a refresh