What is the underlying rhythm? See reply for the answer @amalmattu @MasriAhmadMD @MusaSharkawi @jelevenson @ @mbelshazly #FOAMed #EKG 
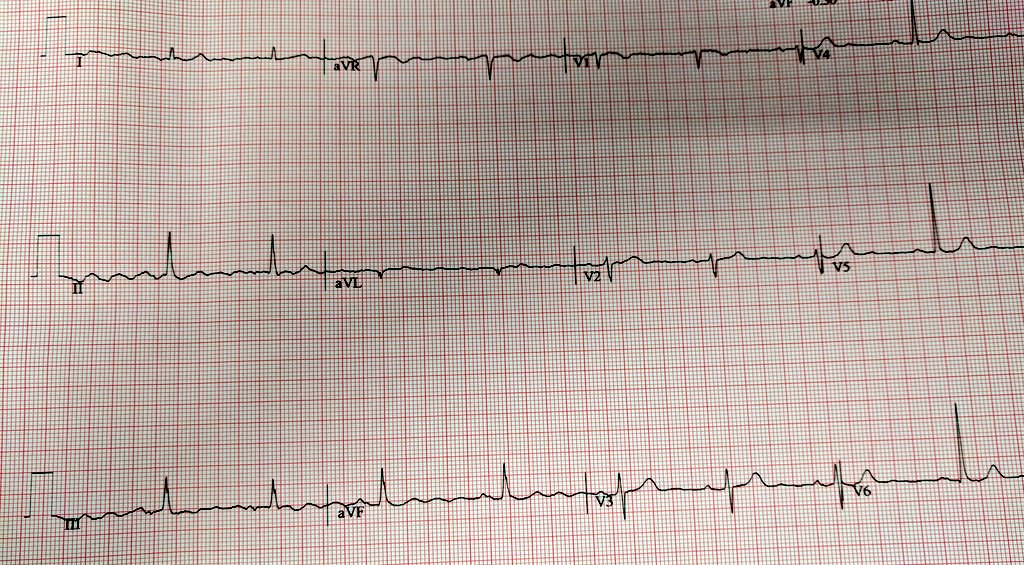
@amalmattu @MasriAhmadMD @MusaSharkawi @jelevenson @mbelshazly A cursory glance may fool one to think this is atrial flutter. On closer inspection clear preceding p-waves are seen. This gentleman has Parkinson's disease and the undulating baseline coincides with his resting tremor frequency.

• • •
Missing some Tweet in this thread? You can try to
force a refresh