
Hospitalist @BIDMC_IM Teaching/Learning Dx @harvardmed❓, Co-host @Dx_Atypia 🦓 🐎, @CPSolvers Academy🕵🏽♂️, @YaleIMed @ColumbiaPS @UF 👨🏽🎓
 The key pivot of this schema emphasizes a search for exogenous culprits of life-threatening disease, as these culprits must either be treated or avoided in the future.
The key pivot of this schema emphasizes a search for exogenous culprits of life-threatening disease, as these culprits must either be treated or avoided in the future.
 Newcomer to the land of monoclonal gammopathies of clinical significance (MGCS)?
Newcomer to the land of monoclonal gammopathies of clinical significance (MGCS)? The "diagnostic arc" of HFrEF 🏔️
The "diagnostic arc" of HFrEF 🏔️
 🗻 The path to paraprotein evaluation may or may not begin with the observation of a "protein gap," meaning a (roughly) 4 g/dL difference between the serum Total protein & Albumin.
🗻 The path to paraprotein evaluation may or may not begin with the observation of a "protein gap," meaning a (roughly) 4 g/dL difference between the serum Total protein & Albumin. 
 Signature ✍️
Signature ✍️
 🥼 Below are the presenting labs (Baseline SCr = 2.0 mg/dL, Baseline NT-proBNP = 2000 pg/mL)
🥼 Below are the presenting labs (Baseline SCr = 2.0 mg/dL, Baseline NT-proBNP = 2000 pg/mL)

 First, recall BP is a product of Cardiac Output * Systemic Vascular Resistance.
First, recall BP is a product of Cardiac Output * Systemic Vascular Resistance.
 The pathophys of HFpEF first involves diastolic dysfunction.
The pathophys of HFpEF first involves diastolic dysfunction. 📚 Note 2: unless concurrent blood disorder, coags = normal!
📚 Note 2: unless concurrent blood disorder, coags = normal!
 Many thanks to @YaleIMed's Drs. Harriet Kluger & @PeterKahnMD for both their active involvement in this case & their support of this write-up.
Many thanks to @YaleIMed's Drs. Harriet Kluger & @PeterKahnMD for both their active involvement in this case & their support of this write-up. Pulmonary Infarction is the result of a simple series of events:
Pulmonary Infarction is the result of a simple series of events: B/c hydrostatic pressures are higher on the parietal pleura than on the visceral pleura & the oncotic pressures are equivalent, pleural fluid is primarily produced from the parietal pleura. The lymphatic vessels on the parietal pleura are responsible for pleural fluid resorption.
B/c hydrostatic pressures are higher on the parietal pleura than on the visceral pleura & the oncotic pressures are equivalent, pleural fluid is primarily produced from the parietal pleura. The lymphatic vessels on the parietal pleura are responsible for pleural fluid resorption. 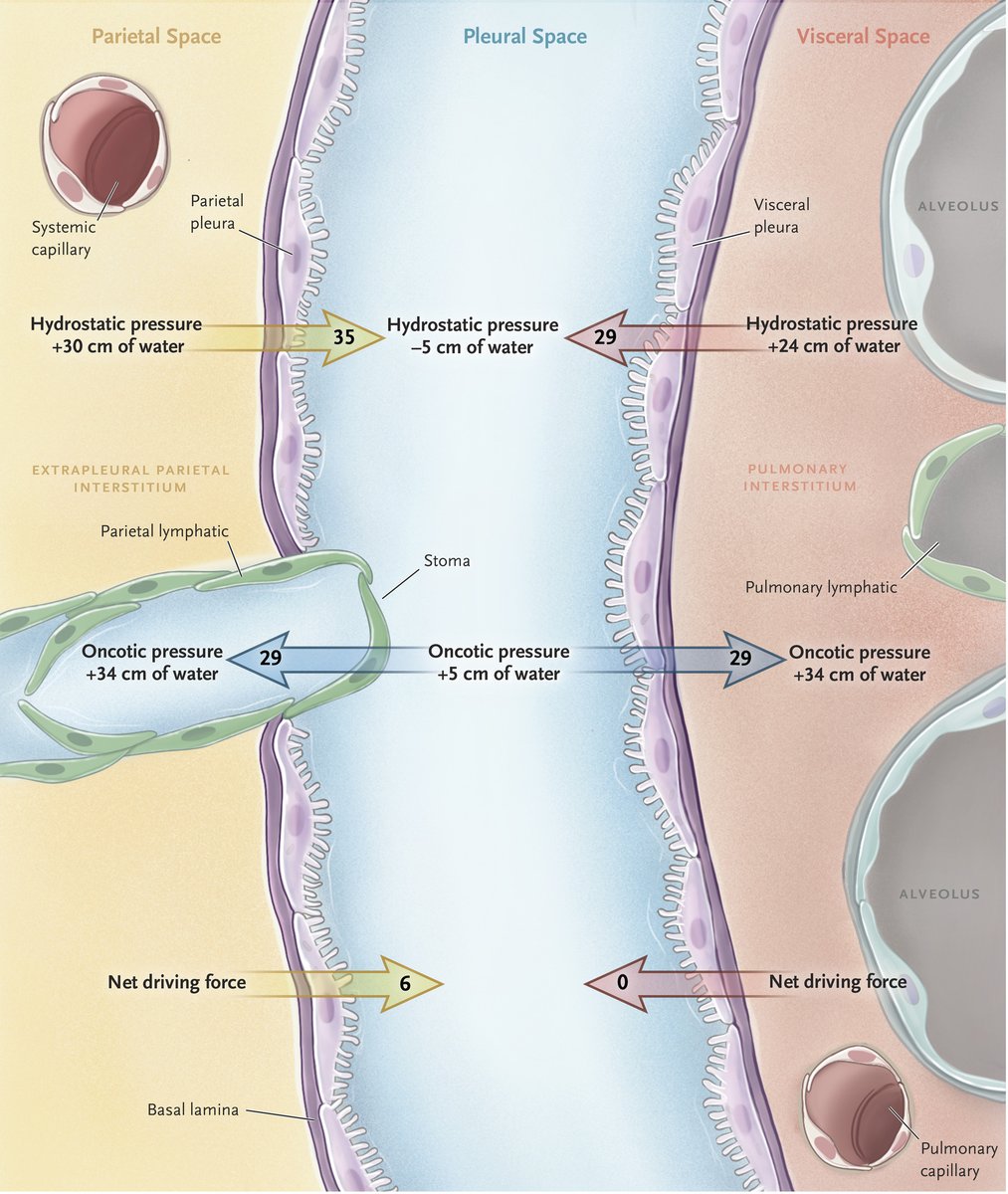
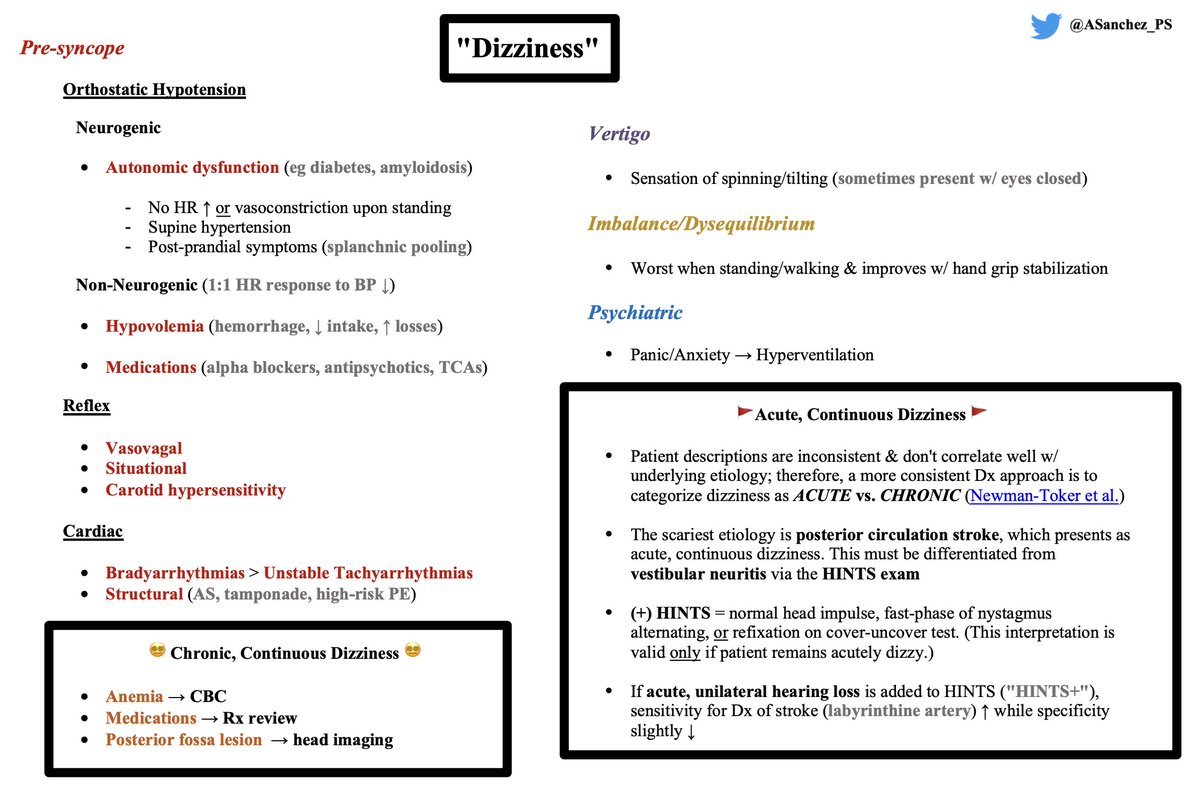 Dizziness 2/2 Pre-syncope:
Dizziness 2/2 Pre-syncope:
 Updated Lymphoma review:
Updated Lymphoma review:
 Acute hepatocellular injury = 3 P's.
Acute hepatocellular injury = 3 P's.
 Maddrey discriminant function calculator here: mdcalc.com/calc/56/maddre…
Maddrey discriminant function calculator here: mdcalc.com/calc/56/maddre…
 💭 Tips 💭:
💭 Tips 💭:


 🔬 Previously, a lymphoid neoplasm of the marrow/blood = leukemia, solid lymph node (LN) neoplasm = lymphoma
🔬 Previously, a lymphoid neoplasm of the marrow/blood = leukemia, solid lymph node (LN) neoplasm = lymphoma This framework inspired by:
This framework inspired by: First, some review. Where does monoclonal protein come from?
First, some review. Where does monoclonal protein come from?