
Infectious Disease Immunology physician specializing in complex chronic diseases. Views are my own; no medical advice given.
2 subscribers
 I believe this injury is reversible because I witness recovery - but it is profoundly unrecognized across medicine. Without recognition, patients are dismissed, under-investigated, and told they are fine while cognitive function and quality of life continue to decline.
I believe this injury is reversible because I witness recovery - but it is profoundly unrecognized across medicine. Without recognition, patients are dismissed, under-investigated, and told they are fine while cognitive function and quality of life continue to decline.
 The real questions are upstream:
The real questions are upstream: Throughput medicine rewards:
Throughput medicine rewards: Medical PTSD may show up as intense anxiety before appointments, avoidance of care, emotional numbing, or physiological distress during routine exams. Triggers can include specific language, environments, or clinician behavior.
Medical PTSD may show up as intense anxiety before appointments, avoidance of care, emotional numbing, or physiological distress during routine exams. Triggers can include specific language, environments, or clinician behavior.
 Memantine reduces glutamatergic excitotoxicity and dampens neuroinflammatory signaling. In ME/CFS and Long COVID, it improves cognitive steadiness, reduces sensory hypersensitivity, and increases threshold for mental exertion.
Memantine reduces glutamatergic excitotoxicity and dampens neuroinflammatory signaling. In ME/CFS and Long COVID, it improves cognitive steadiness, reduces sensory hypersensitivity, and increases threshold for mental exertion.
 These patients often present with severe orthostatic intolerance, paradoxical drug reactions, and hypersensitivities that limit even supportive interventions. Standard protocols frequently provoke deterioration and conventional care models are insufficient and risky.
These patients often present with severe orthostatic intolerance, paradoxical drug reactions, and hypersensitivities that limit even supportive interventions. Standard protocols frequently provoke deterioration and conventional care models are insufficient and risky.
 In ME/CFS and Long COVID, headaches may resemble migraine but can also reflect intracranial pressure disturbances, autonomic dysfunction, or cervical instability. History and exam must assess positional changes, visual symptoms, and response to previous migraine therapy.
In ME/CFS and Long COVID, headaches may resemble migraine but can also reflect intracranial pressure disturbances, autonomic dysfunction, or cervical instability. History and exam must assess positional changes, visual symptoms, and response to previous migraine therapy.
 Many post-COVID patients with fatigue, cognitive issues, GI symptoms, or multi-system complaints likely have an underlying connective tissue disorder.
Many post-COVID patients with fatigue, cognitive issues, GI symptoms, or multi-system complaints likely have an underlying connective tissue disorder. This dysfunction may lead to HPA axis disruption, chronic sympathetic activation, and impaired homeostatic recovery. Clinically, this may present as fatigue, orthostatic intolerance, cognitive dysfunction, and post-exertional malaise.
This dysfunction may lead to HPA axis disruption, chronic sympathetic activation, and impaired homeostatic recovery. Clinically, this may present as fatigue, orthostatic intolerance, cognitive dysfunction, and post-exertional malaise.
 For neuroinflammation and perfusion - pressure, cognitive lag, sensory overload - pentoxifylline (TNF-α, microvascular support) and PDE3 inhibitor cilostazol (cAMP modulation, antiplatelet effect). LDN - when it works - can enhance glial signaling; minocycline in short courses.
For neuroinflammation and perfusion - pressure, cognitive lag, sensory overload - pentoxifylline (TNF-α, microvascular support) and PDE3 inhibitor cilostazol (cAMP modulation, antiplatelet effect). LDN - when it works - can enhance glial signaling; minocycline in short courses.
 Phosphatidylcholine supports cellular membrane integrity and mitochondrial repair, aiding in cognitive function and energy metabolism disrupted in ME/CFS and Long COVID as well as mast cell degranulation in MCAS.
Phosphatidylcholine supports cellular membrane integrity and mitochondrial repair, aiding in cognitive function and energy metabolism disrupted in ME/CFS and Long COVID as well as mast cell degranulation in MCAS.
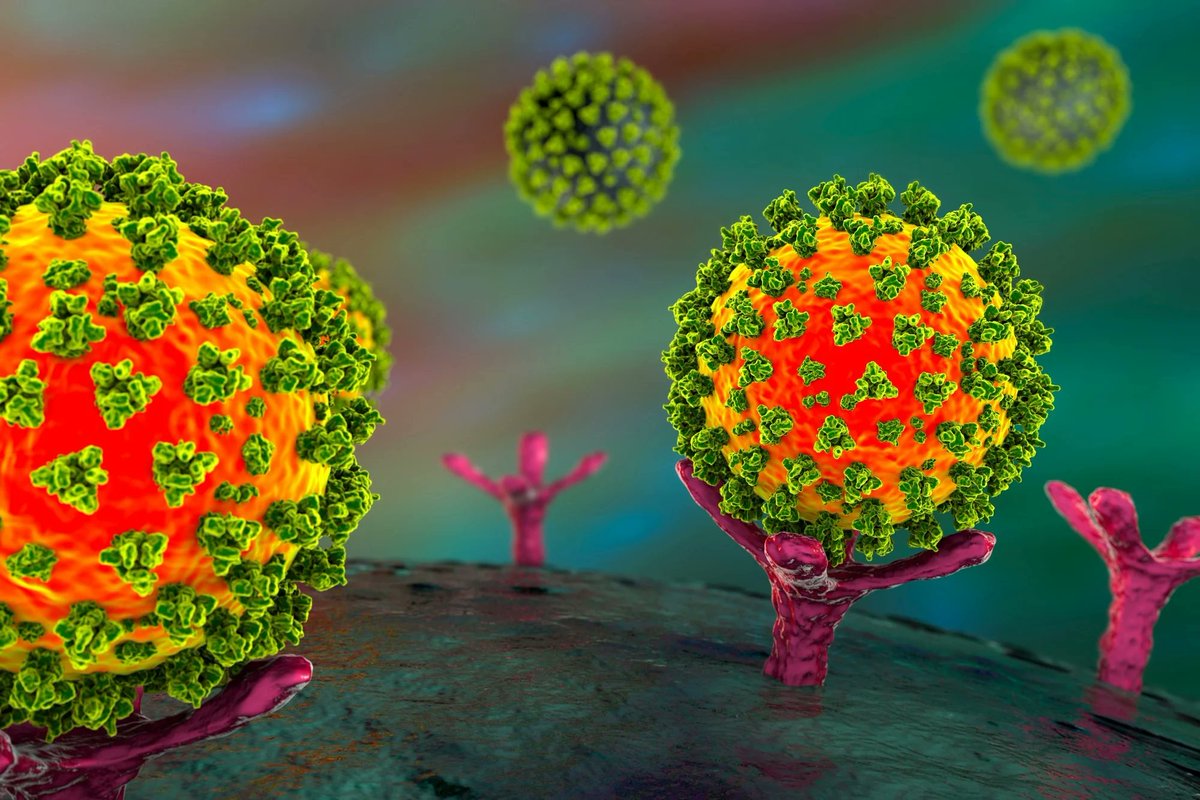 1. The ACE2 receptor, expressed in multiple organs, may harbor viral persistence, triggering inflammatory and immune responses.
1. The ACE2 receptor, expressed in multiple organs, may harbor viral persistence, triggering inflammatory and immune responses. Possible mechanisms of disease include:
Possible mechanisms of disease include: Clinical manifestations include however are not limited to:
Clinical manifestations include however are not limited to: Patients commonly describe edema, darkening, hyperemia and/or mottling of the extremities - most commonly the legs - amidst a setting of orthostatic intolerance, fatigue and weakness. Actions such as meal preparation or showering may seem insurmountable due to orthostasis.
Patients commonly describe edema, darkening, hyperemia and/or mottling of the extremities - most commonly the legs - amidst a setting of orthostatic intolerance, fatigue and weakness. Actions such as meal preparation or showering may seem insurmountable due to orthostasis.
 Patients often describe the internal tremor as a sensation of vibration or buzzing occurring internally as opposed to external. Patients have additionally described an internal "shuddering" or "wobbling" sensation most pronounced in the chest, abdomen, or extremities.
Patients often describe the internal tremor as a sensation of vibration or buzzing occurring internally as opposed to external. Patients have additionally described an internal "shuddering" or "wobbling" sensation most pronounced in the chest, abdomen, or extremities.
 Livedo reticularis - net-like pattern of discoloration that can appear as purplish or bluish patches
Livedo reticularis - net-like pattern of discoloration that can appear as purplish or bluish patches 
 Common triggers for MCAS include (feel free to contribute your unique triggers if not included below)
Common triggers for MCAS include (feel free to contribute your unique triggers if not included below)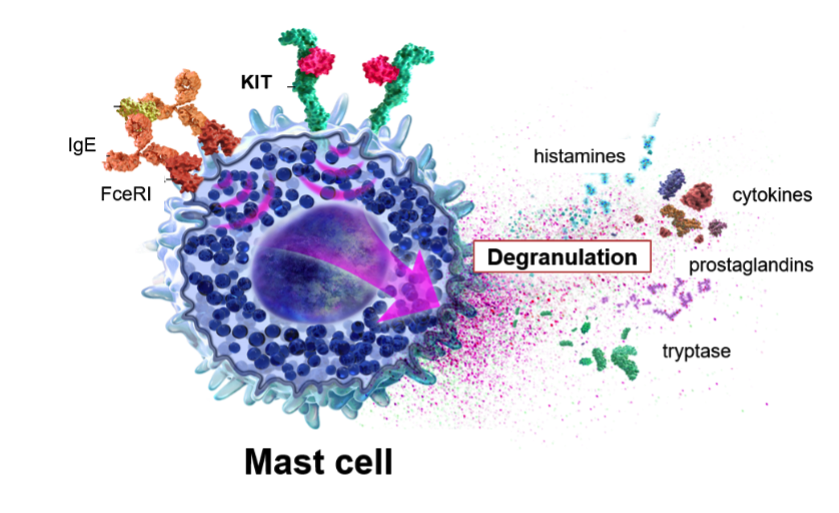 Genetic factors in MCAS
Genetic factors in MCAS Nasal-ocular - congestion and eye watering and itching
Nasal-ocular - congestion and eye watering and itching  Mitochondrial dysfunction deleteriously affecting cellular energy production may lead to reduced delivery of oxygen and nutrients to the brain resulting in cognitive impairment.
Mitochondrial dysfunction deleteriously affecting cellular energy production may lead to reduced delivery of oxygen and nutrients to the brain resulting in cognitive impairment.