Gastroenterologist & Hepatologist.
Disorders of the Gut Brain Axis.
Treating Long Covid, POTS, MCAS, hEDS.
Jun 27 • 33 tweets • 6 min read
POTS - Salt and water
Whenever I diagnose a pt with POTS, I explain how POTS affects their body (but in particular their gut). I then show how this leads to the development of symptoms. And how to treat.
For every disease we should always discuss treatments
And different options.
We should always start with the easiest, cheapest, lowest risk intervention first. Lifestyle factors should always be discussed.
Once I have discussed the different treatments, risks and benefits and likely success rates I then garner pt preference
May 23 • 19 tweets • 4 min read
The Corn 🌽 test
The most helpful, easiest, most readily available and cheapest test in functional GI medicine and the most underutilized.
So what is the Corn 🌽 test?
You eat a piece of corn on the cob and document how long it takes for you to see it appear in your stool
I call it the “poor man’s gut transit test “
It is a surrogate marker of whole gut transit time.
You should see the corn in your stool within 24 hours.
So who should perform the corn test?
A better question is who should not perform the corn test?
Anyone allergic to corn
May 6 • 26 tweets • 5 min read
The difficult patient # 4
Severe upper abdominal pain.
The 3 main causes of severe upper abdominal pain are all due to visceral hypersensitivity.
The visceral hypersensitivity makes the following pathologies present symptomatically.
In order of most common
1- Gastric visceral hypeersensitivty 2- MALS 3- SMA syndrome.
Let me explain in more detail.
1- gastric visceral hypersensitivity
This presents in 2 different ways
A - severe epigastric pain +/- loss of appetite, early satiety nausea and reflux
Apr 29 • 34 tweets • 6 min read
The difficult patient #3
Severe lower abdominal /pelvic pain.
Pts with POTS and MCAS are more likely to have
-Endometriosis
This can commonly mimic symptoms of”IBS” and need to be kept in mind
-vascular compression syndromes
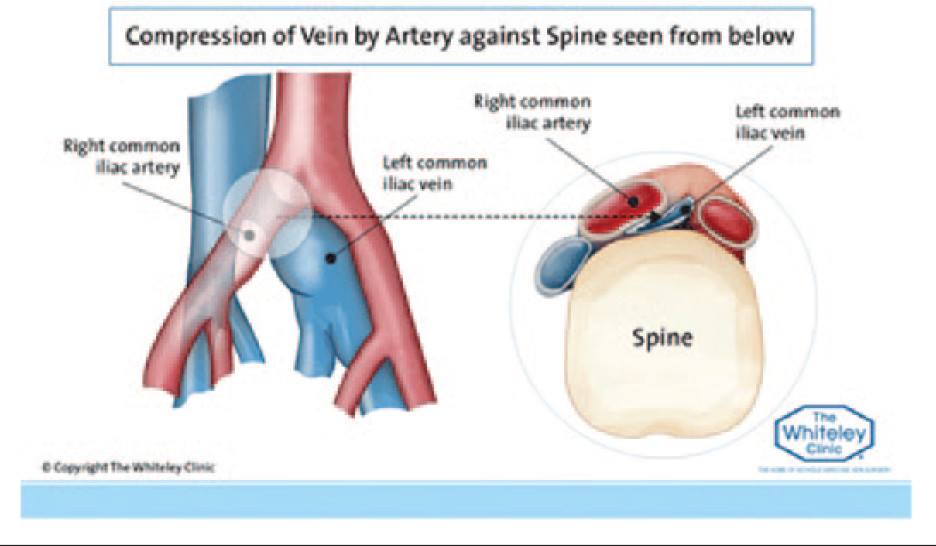
Pelvic congestion syndrome
This is usually due to a May Thorne (Left common iliac vein compression) or Left renal vein compression.
The pain of PCS is usually described as a deep pelvic pain or pressure.
It is usually worse on standing (inc the VCs and allows for blood pooling)
Apr 27 • 21 tweets • 4 min read
The difficult patient #2
Severe diarrhea not responding to usual treatments.
Keeping in mind that this post assumes a normal gastroscope, colonoscopy and biopsies.
Diarrhea in this situation is usually one of three options
1 - True diarrhoea
2 - Diarrhoea secondary to Faecal loading
3 - Diarrhoea due to severe obstructed defecation
Apr 26 • 15 tweets • 3 min read
The difficult patient presentation.
I thought I would do a series of posts on some of the most difficult to treat GI patients I see, and how I approach their management
Such as 1/ severe food Intolerances 2/ severe diarrhea 3/ severe abdominal pain
So let’s start
1- severe food intolerance
I see many patients who come to me only able to tolerate a small handful of foods. “I can only eat chicken breast, potato and lettuce- all other foods I react to”
Sometimes these food reactions cause disabling GI symptoms. Other times
Feb 28 • 10 tweets • 2 min read
Microdosing GLP1a/GIP agonists
Lots of interest in this topic. Particularly with @dysclinic publishing a case report showing improvement in POTS
I generally try to optimize my pts bowels and POTS before starting these drugs. I have seen improvement in POtS but
It’s always hard to know if the POtS is improving because the MCAS is (and the MCAS was driving the POTS)
Or the weight gain leads to better nutrition which helps autonomic function.
So is it a direct effect by improving the vagovagal reflex or via indirect mechanisms?
Feb 3 • 25 tweets • 4 min read
Why microdosing GLP1a/GIP agonist (Tirzepatide) helps POTS/MCAS/Long COVID/Functional GI symptoms.
#POTS #MCAS #LC #DGBI #microdosing
I had an epiphany a few months ago. One of those “why didn’t I realize this sooner” moments.
Why do microdosing GLP1a/GIP agonists help this cohort?
Before we delve further let’s look at how these drugs work. Whilst they are best known for their weight loss effects, they have lots of other beneficial actions
Dec 5, 2025 • 25 tweets • 4 min read
All things Gastric
Part 3 how to use GLP1a agonists.
GLP1a agonists work to reduce weight by the following mechanisms 1- they tell your brain you are not hungry 2- they slow down gastric emptying so you feel fuller for longer after eating, and therefore eat less
3- reduce inflammatory markers in particular IL-6, and TNF alpha 4- in some patients with MCAS they act like mast cell stabilizers
(Like all MCAS drugs they only work in some patients not all)
In normal patients (in whom calories in exceed calories out is driving weight)
Dec 4, 2025 • 17 tweets • 3 min read
All things Gastric
Part 2 Gastric Symptoms
The following symptoms can arise due to dysfunction in gastric function
Loss of appetite
Feeling full quickly when eating or for a long time after eating
Bloating
Belching
Pain
Nausea
Vomiting
Reflux acid or liquid
I find it easier to break symptoms down into 1/ those occurring with or after eating due to abnormal Digestive phase 2/ those occurring in the inter digestive phase
Let’s start with the second one as it is easier
Dec 4, 2025 • 15 tweets • 3 min read
All things Gastric
I thought I would do a series of posts on the stomach 1/ Normal Gastric Function 2/ Gastric symptoms including Gastroparesis 3/ How to use GLP1a in patients with Gastroc symptoms INCLUDING Gastroparesis.
#POTS #MCAS #hEDS
#Gastroparesis
1/ Normal Gastric Function
The stomach has 3 anatomical regions (fundus, body, antrum (and pylorus)
But from a functional point of view the stomach has 2 regions.
Upper stomach
Lower stomach
The Upper Stomach includes the Fundus and part of the Gastric Body
Sep 4, 2025 • 6 tweets • 1 min read
@GI_Pearls Once you truly understand the gut brain axis and DGBI u realise the DGBI are the gut manifestations of POTS and MCAS. I treat all my DGBI with antihistamines and mast cell stabilizers. Mast cells release mediators that cause visceral hypersensitivity.
@GI_Pearls The reason for the triad is that the ANS and mast cells are abundant in and control the integrity of the connective tissue. When dysfunctional they will cause an asymptomatic hEDS to become symptomatic.
And abnormal connective tissue will place abnormal shear stress
Aug 31, 2025 • 11 tweets • 2 min read
Abdominal pain in patients with FGID/DGBI/IBS
I see a lot of post where people complain of agonizing pain.
As well as lots of other symptoms.
So how do I approach abdominal pain?
Location and association with bowel motions.
Most cases of severe abdominal pain
Associated with the urge to defecate, or feel better or slightly better after using your bowels (or passing wind) is a colonic symptom. And it is due to faecal loading. But when I say this people say, “but I have diarrhoea” or “I go regularly “
Jun 6, 2025 • 10 tweets • 2 min read
Why do my bowels not work?
For those that suffer constipation or painful diarrhoea due to faecal loading treatment needs to focus on three key elements.
Unless you address them all you will not have success 1/ a rectum that senses the faeces and provides
The urge to defecate, teemed with a correct defecatory technique and adequate pelvic floor function.
Most of my pts have dyssynergia defecation. When the patient tries to push the faeces out, instead of relaxing the EAS
Jun 5, 2025 • 21 tweets • 4 min read
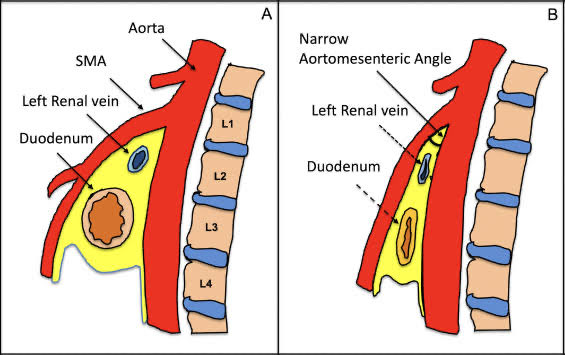
MALS and SMAS part 2
SMAS
Superior mesenteric artery compression of the third part of the duodenum.
This usually cooccurs with Left renal vein compression by the SMA, because they both “sit” under and between the SMA and the aorta.
If MALS is thought to be then SMAS is thought to be a unicorn.
The irony is it is more common than MALS but…
Whilst the compression alone (ie not causing symptoms so can’t be called a VCS) is more common,
Symptomatic SMAS is less common than symptomatic MALS.
Jun 5, 2025 • 19 tweets • 4 min read
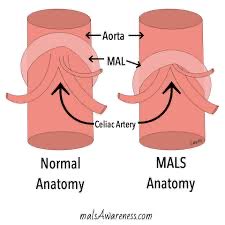
MALS and SMAS
I have previously posted on vascular compression syndromes in trifecta pts.
I left the best to last.
Going thru medicine and gastro training we were never taught about these two syndromes.
Occasionally in a radiology meeting someone would
Through out MALS or SMAS as a cause of chronic unexplained pain and all the registrars and residents would quickly google it.
So what are these conditions?
In my previous post on VCS (vascular compression syndromes) I spoke about how they are almost universal
May 8, 2025 • 12 tweets • 2 min read
Diagnostic criteria for MCAS
I had an interesting letter back the other day from an immunologist looking after my pt. I had started her on Famotidine (H2 blocker) for her gut symptoms and as an antihistamine and Prucalopride (stimulates gut motility)
I view IBS as the gut manifestation of POTS and MCAS and treat all pts as having both diseases
Whilst it is always ideal to stagger introducing new meds in MCAS pts as inc risk of drug reactions and want to know which drug it is, the pt started both together.
Mar 18, 2025 • 10 tweets • 2 min read
What a load of fucking bullshit.
1/100 cardiac arrhythmias. Bullshit
1/2000 bleeds requiring i patient admission. Bullshit
1/2000 req emergency surgery. Bullshit.
1/6000 splenic injury. Bullshit
1/1000 infections leading to sepsis. Bullshit
1 perforation
1 splenic rupture req splenectomy
Since cold snare polypectomy for large polyps and the use of clips my post polypectomy admission rate dropped from 1 every three years to 0 in last 3 years.
0 sepsis
Dec 29, 2024 • 23 tweets • 4 min read
Vascular Compression Syndromes (VCS) in POTS patients
In my experience, VCS are present in ALL patients with POTS, and are usually multiple. For the purposes of this thread this also applies to hEDS and trifecta patients as well.
So what is a VCS? A 🧵
A VCS is when a vascular structure (artery or vein) is either 1/ Being compressed by an adjacent structure or 2/ Is compressing an adj structure leading to the generation of symptoms
If the compression is asymptomatic we call it Vascular Compression Anatomy
Nov 4, 2024 • 5 tweets • 1 min read
Another commone medication mistake in POTS
If I am using Ivabradine (or if on beta blockers, - I never use beta blockers) these drugs are usu given twice a day.
But what does twice a day mean to you and the pt, and why is twice a day diff for POTS pt?
HR control is a symptomatic treatment, if you standing and walking around the house HR is under 100 you may not need the second dose,
Particularly as POTS is worse in the morning. SO by the afternoon, your HR may be better and you may not need the second dose.
Nov 4, 2024 • 20 tweets • 4 min read
DIVERTICULAR DISEASE
I think Diverticular disease, whilst very common, is very poorly understood.
Some definitions
Diverticulum - single
Diverticula - plural
Diverticular disease (DD) - presence of diverticula in the bowel
DD usually involves the sigmoid colon
It can occur in any part of the gut however.
It arises when a section of the bowel lining forms a little outpouching of the bowel wall.
It is thought to arise at sites of weakness in the bowel wall.
They are more likely to occur in the sigmoid colon