
Ravi Gupta is Hong Kong Jockey Club Professor of Global Health, University of Cambridge. TIME100 Most Influential 2020; Clarivate Highly Cited Researcher




 We first measured baseline SARS-CoV-2 seroprevalence prior to vaccination using flow cytometry methods for binding antibodies to nucleocapsid (N), coupled with virus neutralisation approaches for protective neutralizing antibody responses to VOC (January 2021)
We first measured baseline SARS-CoV-2 seroprevalence prior to vaccination using flow cytometry methods for binding antibodies to nucleocapsid (N), coupled with virus neutralisation approaches for protective neutralizing antibody responses to VOC (January 2021)









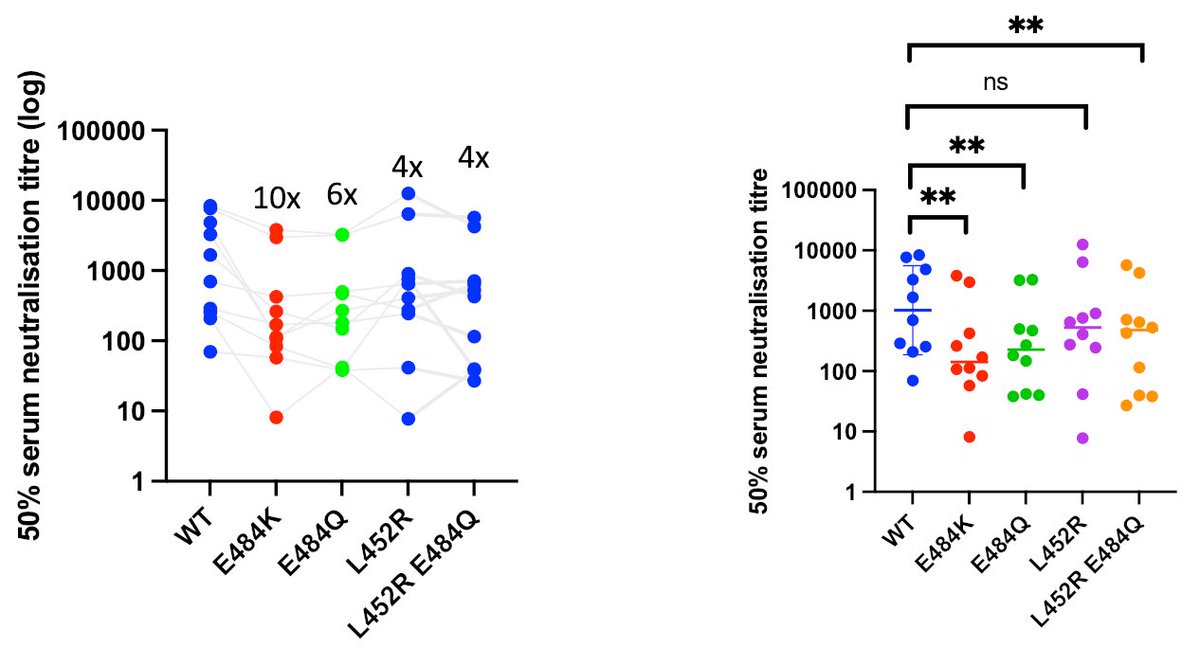

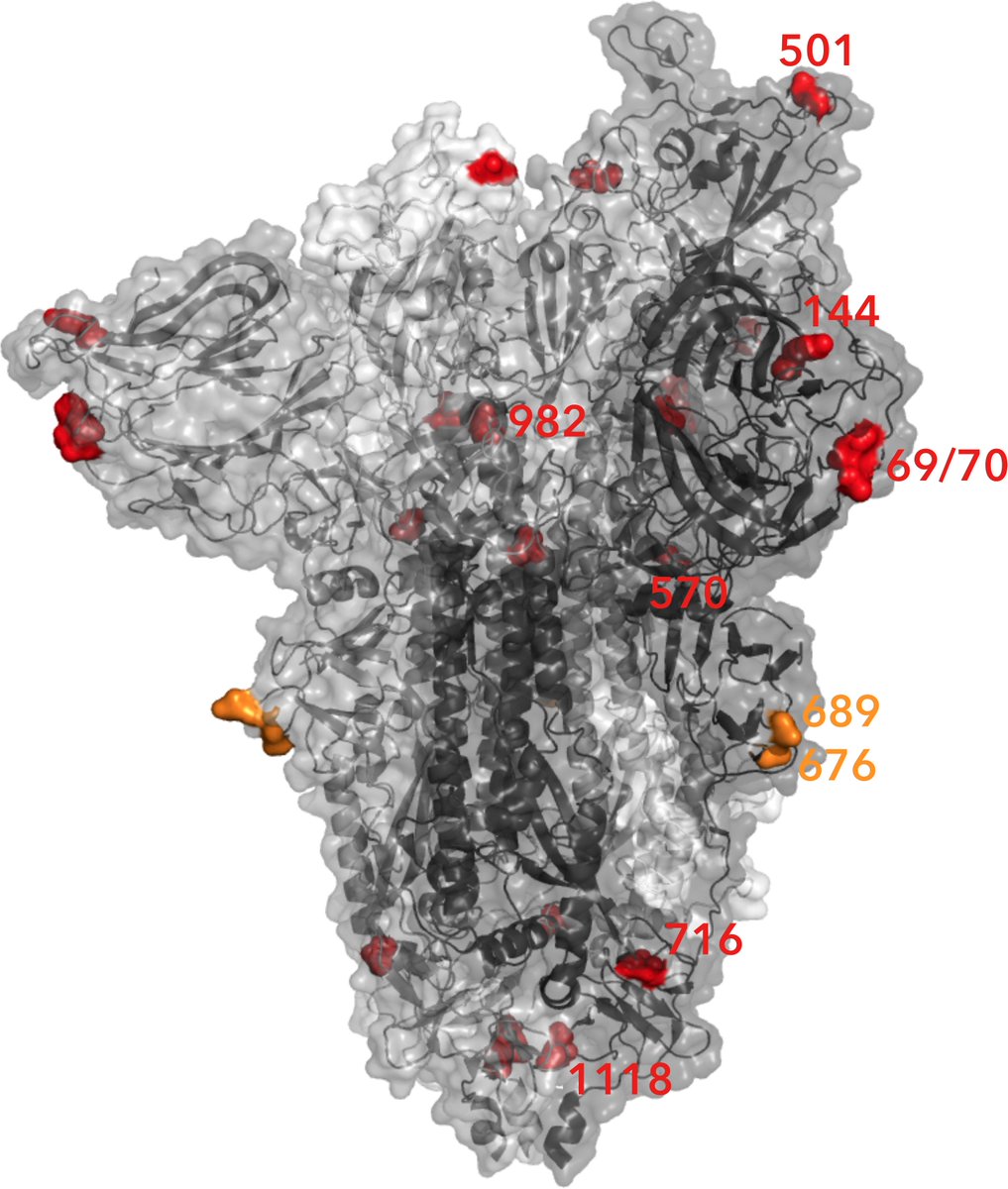 The numbers infected with B1.1.7 has been growing faster than other UK variants based on independent data sources. This variant of SARS-CoV-2 is therefore thought to be more transmissible by around 50%. Data suggest it does not lead to more severe illness however.
The numbers infected with B1.1.7 has been growing faster than other UK variants based on independent data sources. This variant of SARS-CoV-2 is therefore thought to be more transmissible by around 50%. Data suggest it does not lead to more severe illness however.
