Ultramarathoner, triathlete & #LongCovidAdvocate I never wanted to be / LC-dysautonomia & LC-MCAS
Jan 24 • 5 tweets • 1 min read
My MCAS=>HyperPOTS flare coincide with low C3 and normalize in between the flares
Together with ⬆️Factor VIII/VonWillenbrand in bad flares+low C3
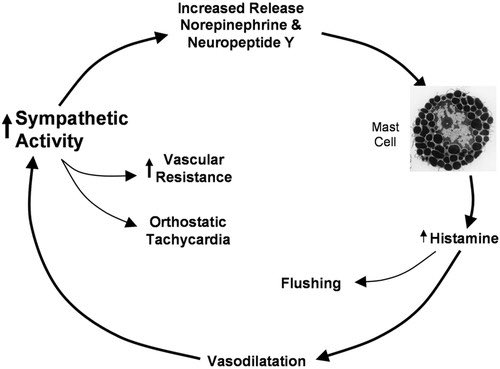
=> alternative complement pathway+mast cell activation leading to endothelial activation => autonomic instability/dysautonomia
Factor VIII is a non-specific marker of mast cell activation and would be elevated together w/VWF (carries FVIII), in flares both are ⬆️10-20% for me
FVIII+VWF+C3 normalize when not in MCAS flare
4wks ago (moderate flare) low C3/normal FVIII+VWF, 2 wks ago C3 back to normal
Mar 26, 2024 • 18 tweets • 6 min read
“Complete remission with histamine blocker in a patient with intractable hyperadrenergic postural orthostatic tachycardia syndrome secondary to long coronavirus disease syndrom” full text
1/journals.lww.com/jhypertension/…
This paper’s case study describes my #LongCovid 1/1, and how #MCAS and #HyperPOTS are inseparably connected in a vicous circle, or a “close-loop mechanism with positive feedback established after SARS-CoV-2 infection in a previously healthy young patient”
2/
Mar 3, 2024 • 19 tweets • 4 min read
I think it’s really harmful when fellow #LongCovid patients w/ #MCAS insist on low-histamine diet as some kind of bulletproof approach that is bound to make #MCAS better and patients unable/unwilling to follow it should feel bad about themselves for not wanting to get better
First of all, mast cells have over 300 receptors => 300+ things control whether and how they degranulate, while dietary histamine is just an additional histamine burden in #MCAS. In contrast, in #HistamineIntolerance dietary histamine is indeed the main problem.