
Rheumatologist at Christian Medical College, Vellore | 🎥 YouTube: "Sullys Rounds" | Passionate about travel and research. ✈️🔬@cmcvellore
 1/9 Why this question matters
1/9 Why this question matters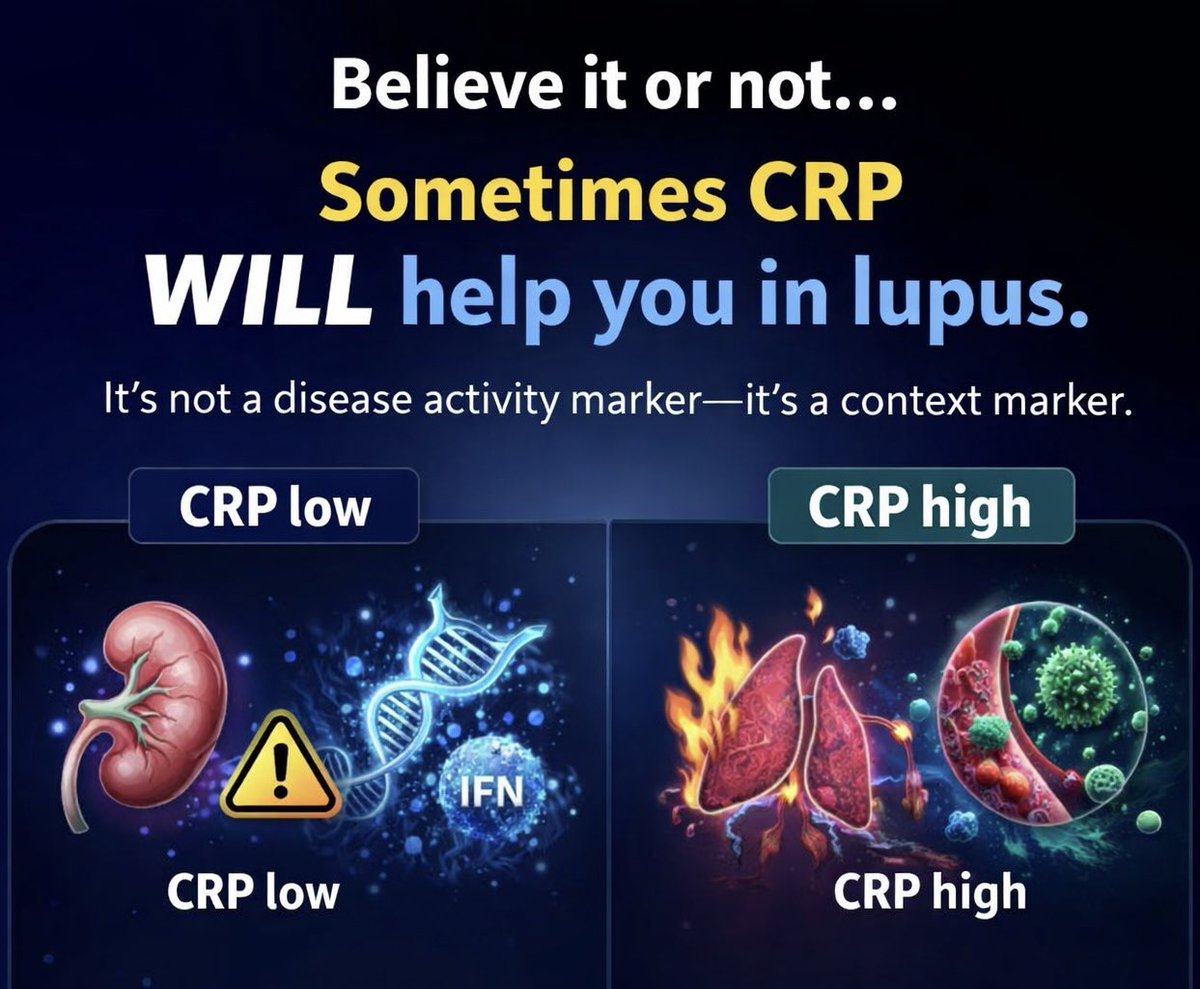 2/6. Lupus is not an IL-6 disease
2/6. Lupus is not an IL-6 disease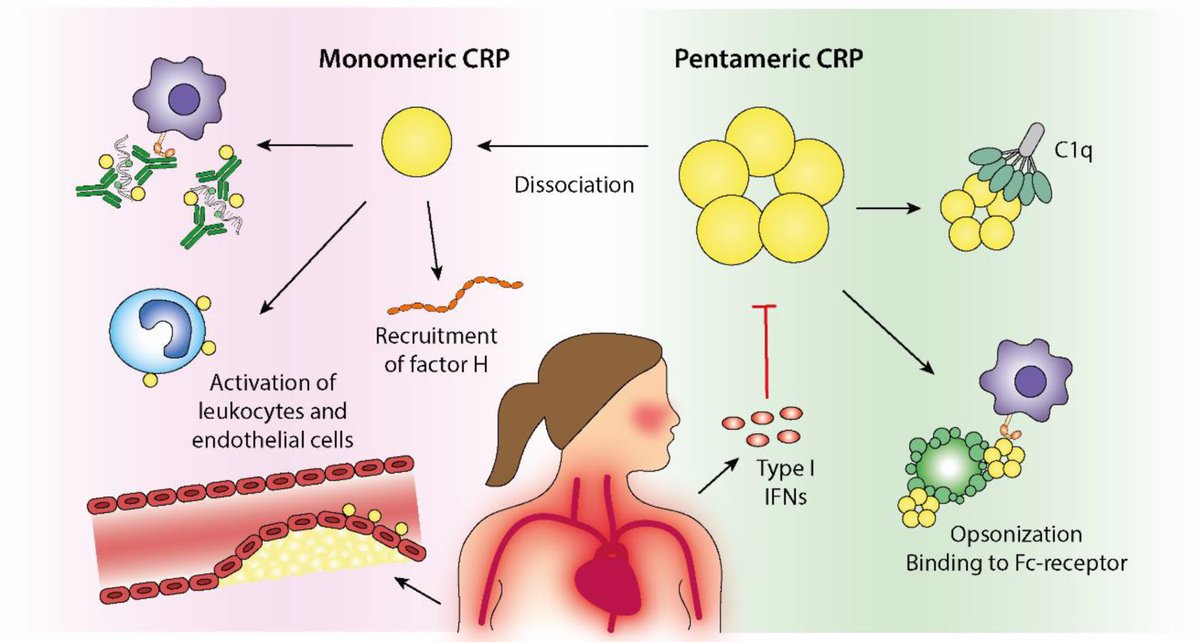
 1/3
1/3 
 1/10
1/10
 🧵 2/7 – STEP 1: Morphology
🧵 2/7 – STEP 1: Morphology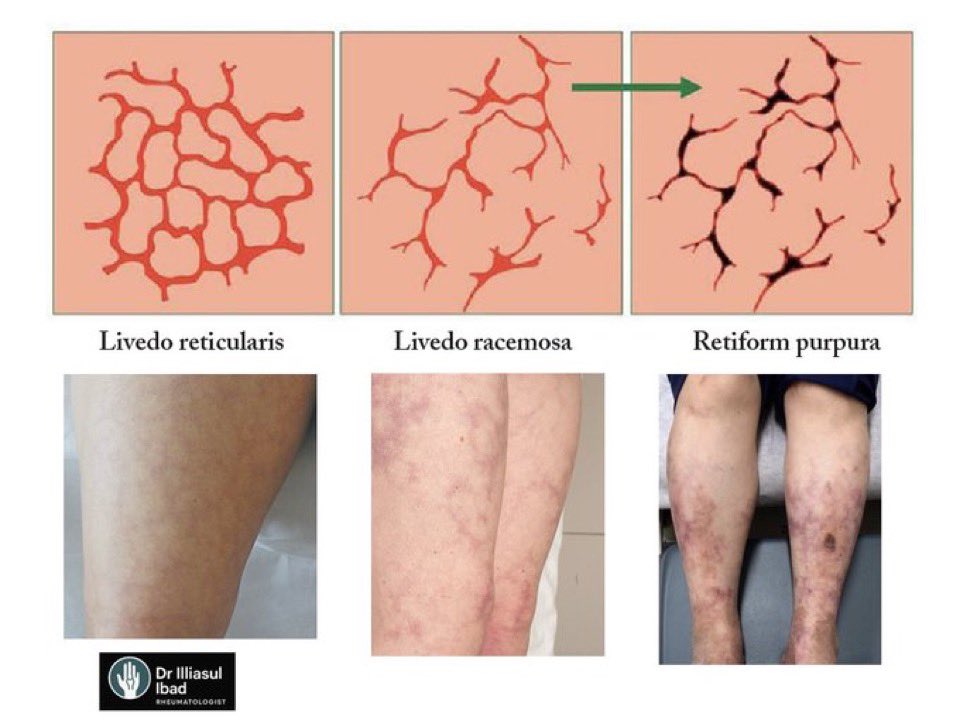
 Tweet 2/6
Tweet 2/6
 Tweet 2/10
Tweet 2/10 Tweet 2/4
Tweet 2/4 Tweet 2/5
Tweet 2/5
 Tweet 2/7
Tweet 2/7 2- Asymptomatic carrier
2- Asymptomatic carrier 
 Tweet 2:
Tweet 2:
 1/
1/
 1/
1/
 2/ Definition of PAH
2/ Definition of PAH  2/
2/
 2/
2/
 2/
2/ Tweet 2:
Tweet 2:
 2/
2/
 But few know about the brilliant scientist who paved the way for its success—Dr. Yellapragada SubbaRow. Let’s uncover his story. 👇
But few know about the brilliant scientist who paved the way for its success—Dr. Yellapragada SubbaRow. Let’s uncover his story. 👇