
orthopaedic trauma surgeon | mama | educator | associate professor @EinsteinMed | 🧡my rescue dog | @BUOrtho @HSpecialSurgery alum | immigrant | 🇺🇸 🕯️🕯️
 [2/18] If you don’t have table with overlapping legs like Hana (sigh), and have a limit to adduction (red), and don’t want to tape nonop leg to the bar or do lithotomy (I hate that position as can cause compartment syndrome), there are a few things you can do with fracture table.
[2/18] If you don’t have table with overlapping legs like Hana (sigh), and have a limit to adduction (red), and don’t want to tape nonop leg to the bar or do lithotomy (I hate that position as can cause compartment syndrome), there are a few things you can do with fracture table. 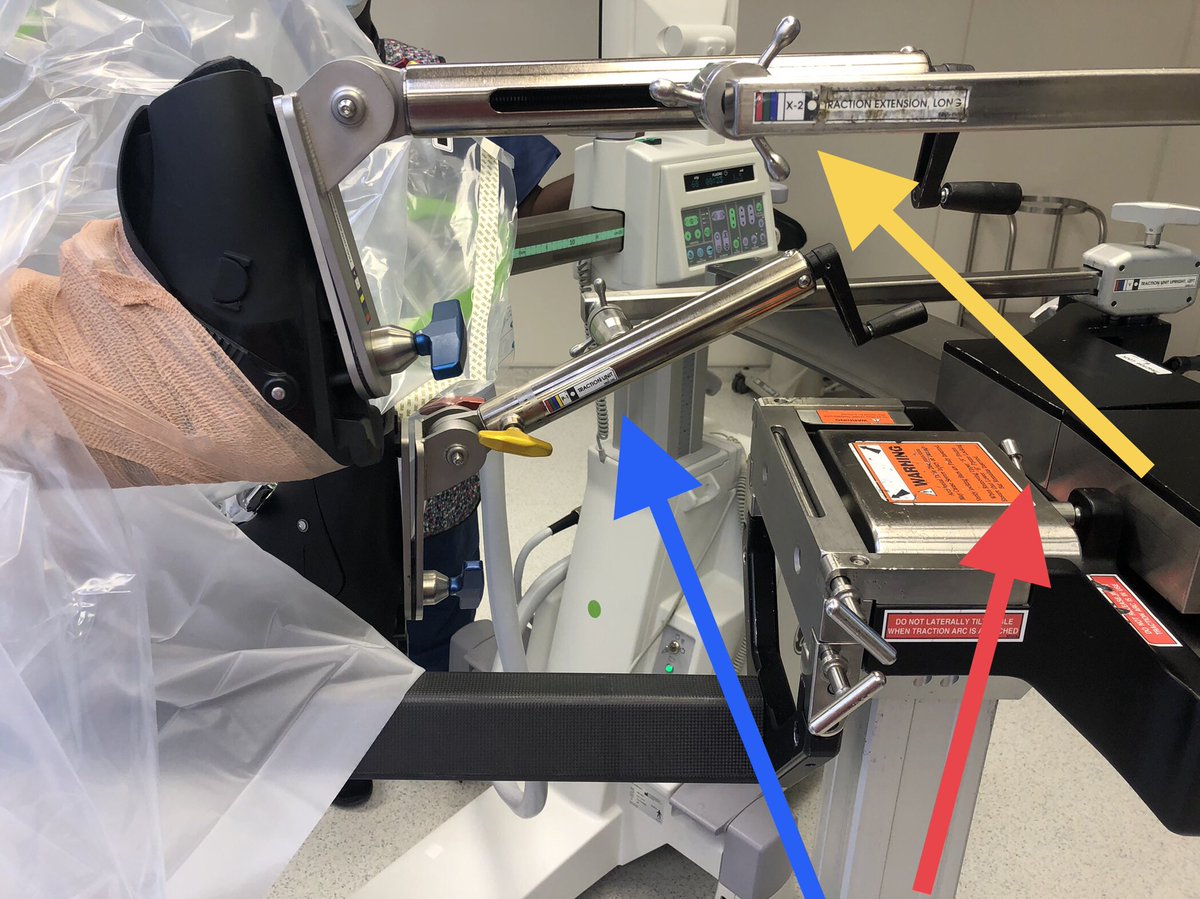

 [2/8] Lateral decubitus is what you want so you can convert, but this can also be done prone (although harder). Unlike most people, he does not use Harris, only AP and lateral and the paper talks about that.
[2/8] Lateral decubitus is what you want so you can convert, but this can also be done prone (although harder). Unlike most people, he does not use Harris, only AP and lateral and the paper talks about that. 



 [2/12] 3D CT of medial, posterior, and lateral. Let this percolate in your brain a minute— what is the order of fixation? How many approaches? Which fragments have joint on them and must be fixed?
[2/12] 3D CT of medial, posterior, and lateral. Let this percolate in your brain a minute— what is the order of fixation? How many approaches? Which fragments have joint on them and must be fixed? 


 [2/9] The lateral shows us the fibula fracture which is the standard SER pattern (proximal posterior to distal anterior), as well as the talus subluxating posteriorly with the posterior malleolus fragment, making the joint incongruent.
[2/9] The lateral shows us the fibula fracture which is the standard SER pattern (proximal posterior to distal anterior), as well as the talus subluxating posteriorly with the posterior malleolus fragment, making the joint incongruent. 
 [2/11] Although this seemed like clear case of undertreated hypertrophic nonunion with stability issue, CRP slightly elevated so I did 2-stage. First was bone biopsy and cultures, which were negative. It also showed how big metaphyseal gap is once hypertrophic bone cleared out.
[2/11] Although this seemed like clear case of undertreated hypertrophic nonunion with stability issue, CRP slightly elevated so I did 2-stage. First was bone biopsy and cultures, which were negative. It also showed how big metaphyseal gap is once hypertrophic bone cleared out. 
