
Professor of Neurology @MayoClinic. Editor-in-chief @ContinuumAAN. Proud @AANMember. Improving systems of care and healthcare value for our patients
2 subscribers
 The imaging demonstrates a spinal longitudinal extradural CSF collection (SLEC)
The imaging demonstrates a spinal longitudinal extradural CSF collection (SLEC)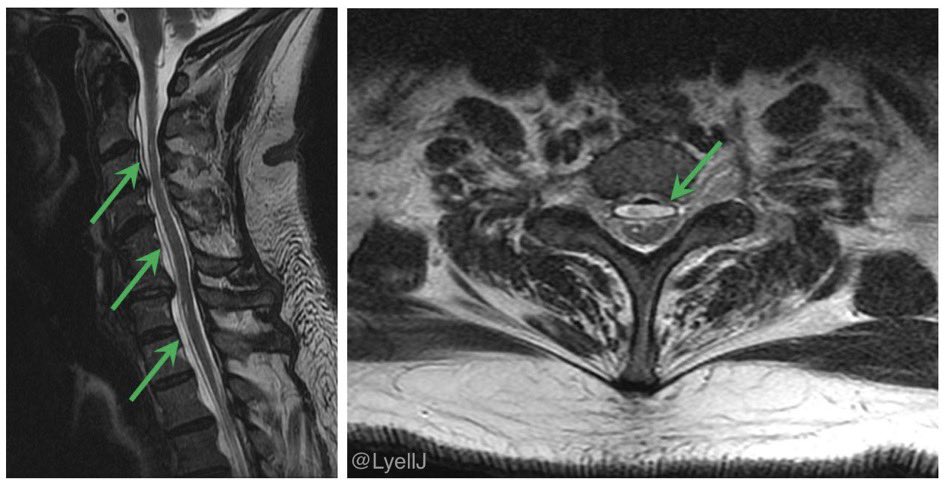
 Back to the patient, a little more history:
Back to the patient, a little more history: Just curious: would you start lecanemab in this hypothetical patient?
Just curious: would you start lecanemab in this hypothetical patient?
 Other features of her pain:
Other features of her pain:

 The patient is a 67 year old woman with episodes of loss of consciousness, leading to a few falls
The patient is a 67 year old woman with episodes of loss of consciousness, leading to a few falls More data:
More data:
 There’s an extra level of difficulty constructing a history in the pediatric setting. Collateral headache history from parents, caregivers, and family is crucial
There’s an extra level of difficulty constructing a history in the pediatric setting. Collateral headache history from parents, caregivers, and family is crucial What is your next move for this patient? #ContinuumCase
What is your next move for this patient? #ContinuumCase
 The patient is otherwise healthy and lives independently. She has a normal neurologic exam and is tolerating her antiseizure medication
The patient is otherwise healthy and lives independently. She has a normal neurologic exam and is tolerating her antiseizure medication Patients undergoing CAR T therapy are medically complex: underlying malignancy, conditioning chemotherapy, risk of infection, and the treatment itself
Patients undergoing CAR T therapy are medically complex: underlying malignancy, conditioning chemotherapy, risk of infection, and the treatment itself You take a closer look.
You take a closer look. 
 More about the spell: he felt lightheaded beforehand, no abnormal movements, and immediately returned to normal thereafter. He has occasional brief lightheadedness on standing
More about the spell: he felt lightheaded beforehand, no abnormal movements, and immediately returned to normal thereafter. He has occasional brief lightheadedness on standing  New spine pain and neurologic deficit in the setting of active malignancy is an emergency!
New spine pain and neurologic deficit in the setting of active malignancy is an emergency! She has a history of migraine and mild hypertension. She’s a light snorer, and gets up 3x a night for the bathroom. She does not have excessive daytime sleepiness, and she has no systemic symptoms (eg weight loss) but she is fatigued
She has a history of migraine and mild hypertension. She’s a light snorer, and gets up 3x a night for the bathroom. She does not have excessive daytime sleepiness, and she has no systemic symptoms (eg weight loss) but she is fatigued At the bedside you see a 57 year old man who is drowsy but oriented following IV lorazepam and levetiracetam. He has low-amplitude writhing movements of all limbs.
At the bedside you see a 57 year old man who is drowsy but oriented following IV lorazepam and levetiracetam. He has low-amplitude writhing movements of all limbs.  Her exam showed severe proprioceptive sensory loss and gait ataxia, so the “inverted V” T2 hyperintensity in the dorsal columns is no surprise. Another clue: her EMG showed an axonal peripheral neuropathy
Her exam showed severe proprioceptive sensory loss and gait ataxia, so the “inverted V” T2 hyperintensity in the dorsal columns is no surprise. Another clue: her EMG showed an axonal peripheral neuropathy First the imaging: his DWI shows an acute right hemispheric ischemic cerebral infarction. SWI shows a convexal subarachnoid hemorrhage, and subcortical microhemorrhages
First the imaging: his DWI shows an acute right hemispheric ischemic cerebral infarction. SWI shows a convexal subarachnoid hemorrhage, and subcortical microhemorrhages
 The MRI shows restricted diffusion and T2 hyperintensity in the cerebellum, temporal lobe, and basal ganglia.
The MRI shows restricted diffusion and T2 hyperintensity in the cerebellum, temporal lobe, and basal ganglia.  How would you respond?
How would you respond?