The TRUTH about Statins, formerly @holmanm
Info is provided for educational purposes only & should not be considered as medical advice. (NO DM's please)
Jul 6 • 8 tweets • 1 min read
1/8 I’ve spent nearly 20 years studying statins through independent research, not industry narratives or marketing. Statins inhibit the mevalonate pathway, reducing far more than cholesterol. They also suppress the production of CoQ10, GGPP, FPP, steroid hormones, heme-A,
/22/8 and other molecules fundamental to normal cellular function.
This isn't simply about lowering LDL. Blocking the mevalonate pathway compromises mitochondrial function, disrupts protein prenylation, alters cell signalling, and affects cell membrane integrity.
/3
Jul 3 • 13 tweets • 2 min read
1/13 A study from 2016 suggests the immune system may play a much bigger role in protecting us from heart disease than previously appreciated.
Researchers found that people with higher levels of IgG antibodies were significantly less likely to suffer a heart attack, /2
2/13 even after accounting for established risk factors such as blood pressure and cholesterol. They also found that antibodies directed against oxidised LDL were associated with lower cardiovascular risk.
/3
Jun 29 • 14 tweets • 3 min read
1/14 A mainstream cardiologist who understood that most lipid-lowering trials have failed to deliver meaningful clinical benefits, and that whatever modest benefit statins appear to show in industry-funded secondary prevention trials may not primarily be due to LDL lowering.
/22/ His letter showed that at least some cardiologists were willing to question the prevailing narrative.
Dear FDA: Resist the Urge on PCSK9 Drugs
An FDA advisory committee recommended approval of two PCSK9 inhibitor drugs. /3
Jun 28 • 7 tweets • 2 min read
1/7 You've finally described one proposed pleiotropic mechanism, but you've presented it as though it's the whole story.
Statins don't selectively inhibit farnesyl and geranylgeranyl synthesis. They inhibit HMG-CoA reductase upstream, /2
2/7 reducing flux through the entire mevalonate pathway.
That affects not only FPP and GGPP, but also dolichols, ubiquinone (CoQ10), heme A precursors and numerous other downstream products. Why are those consequences absent from your explanation ? /3
Jun 24 • 11 tweets • 2 min read
1/11 Lp(a) - Friend or Foe ?
Lp(a) is usually labeled “atherogenic,” but if you look at the biology, there’s a more nuanced story that may intersect with Alzheimer’s pathways.
Lp(a) is basically LDL + apolipoprotein(a), and apo(a) looks a lot like plasminogen. /2
2/11 That matters because plasminogen is part of the fibrin breakdown system, and fibrin isn’t just about blood clots in the body, it also shows up in brain microvasculature and has been found in association with amyloid-β deposits.
/3
Jun 24 • 10 tweets • 2 min read
1/10 It is often claimed that statins are "merely HMG-CoA reductase inhibitors." This is not true. Statins also dramatically elevate reductase levels. In a 1984 Merck paper, they reported that statins trigger more reductase production to compensate for blocking mevalonate
/2
2/10 synthesis, which is essentially a desperate cellular workaround.
Merck even photographed the resulting structural damage to cells. Is this a toxic effect of statins ? Yes, it is unequivocally toxic. It is not normal for cells to churn out bizarre whorls and crystals of /3
Jun 23 • 6 tweets • 1 min read
1/6 This is the Lp(a) paradox: We are told that statins consistently reduce cardiovascular risk in trials, yet they also consistently increase Lp(a), a lipoprotein strongly associated with higher risk of cardiovascular disease.
/22/6 Statins inhibit the mevalonate pathway, reducing downstream products such as ubiquinone, GGPP, FPP and dolichols. This creates metabolic and redox stress within hepatocytes (liver cells), long before any overt cellular dysfunction.
/3
Jun 15 • 12 tweets • 2 min read
1/12 Something has bothered me for years about how we talk about statins.
After a heart attack, NICE recommends high-intensity statin therapy, usually Atorvastatin 80mg. It has become so routine that few stop to ask what the drug is doing beyond lowering cholesterol.
/2
2/12 The assumption is simple:- lower cholesterol equals lower risk, therefore more intensive lowering must be better. If only it was that simple. Statins inhibit HMG-CoA reductase, a key enzyme in the mevalonate pathway. This is often described as the cholesterol pathway, /3
Jun 6 • 10 tweets • 2 min read
1/11 One thing has always puzzled me about statins.
Cardiologists will often say they are cautious about prescribing statins in primary prevention, yet have no hesitation prescribing them in secondary prevention. The question I've never heard properly answered
is WHY ?
/2
2/11 Not with references to guidelines. Not with appeals to authority. Not with a list of studies or trial outcomes. Studies can be manipulated, designed, interpreted and debated in countless ways. What interests me is the biology, because ultimately any claimed benefit
/3
May 30 • 8 tweets • 2 min read
1/8 Spend time in Lp(a) forums and you’ll see a striking pattern: people willing to do almost anything to drive it down. That response is understandable given how strongly Lp(a) has been framed as a cardiovascular risk factor. /22/8 However, there’s an uncomfortable question that rarely gets asked: why is it one of the most genetically locked-in lipoproteins in human biology ?
Lp(a) rises in inflammation and infection. It behaves like an acute-phase reactant, driven by cytokines such as IL-6,
/3
May 29 • 6 tweets • 1 min read
1/6 Note to self: spending too long on Lp(a) forums can seriously damage your brain cells.
Today’s masterpiece was a 72-year-old endurance cyclist proudly explaining how a CAC score of 6,020 - a number so high his coronary arteries now resemble fossilized plumbing, is /22/6 actually evidence that Lipitor saved him.
Apparently decades of statins “stabilized” his arteries by calcifying them into reinforced concrete, while thousands of hours of endurance exercise & oxidative stress somehow combined to create an “elite-flowing athlete’s heart.” /3
May 26 • 10 tweets • 2 min read
1/10 Amazing how every pharma-funded “revolution” starts with dramatic storytelling and ends with a lifetime revenue model.
A few things conveniently missing from this thread:
FOURIER - the largest PCSK9 inhibitor trial ever run (27,564 patients, NEJM), was celebrated as a /2
2/10 triumph because Repatha crushed LDL by 59%. The headlines screamed “15% reduction in cardiovascular events.”
Then independent researchers obtained the underlying clinical study reports from regulators and re-adjudicated the outcomes.
Result ?
/3
May 18 • 11 tweets • 2 min read
1/11 Statins are increasingly linked in both genetic and clinical research to higher rates of insulin resistance and type 2 diabetes - and the mechanism may not be a “side effect” at all, but a direct consequence of how statins 'work'.
/2
2/11 Randomized controlled trials have repeatedly shown increased incidence of T2D in statin users, especially with higher-intensity treatment. Genetic studies examining variants in the HMG-CoA reductase pathway show the same pattern.
/3
May 17 • 9 tweets • 2 min read
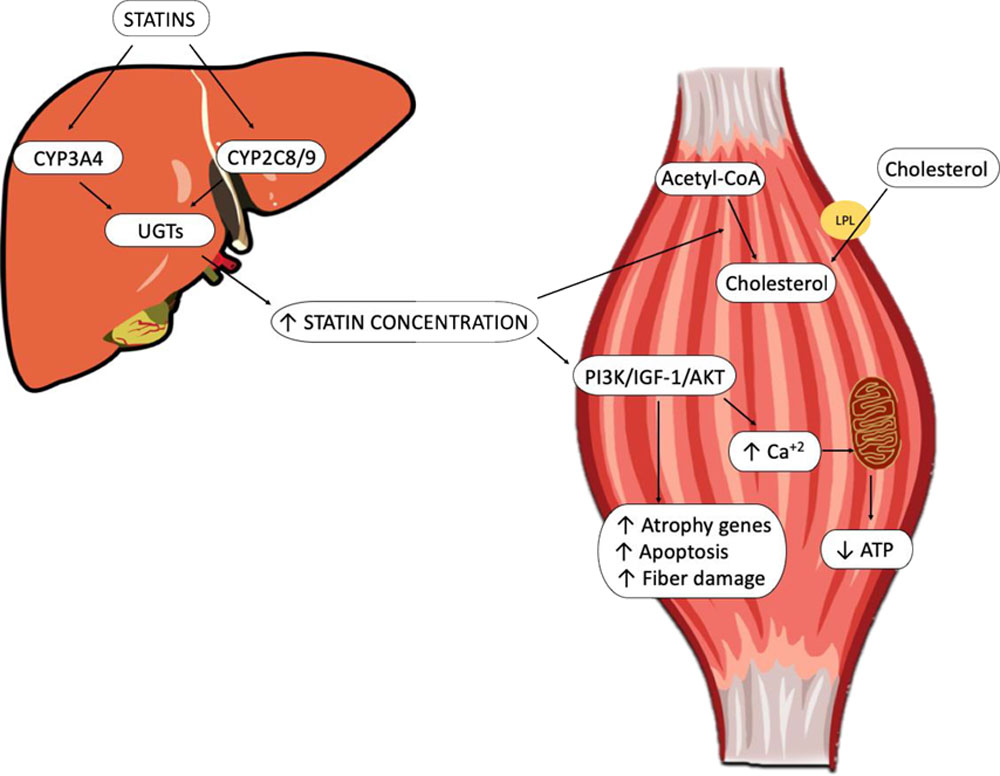
1/9 A lot of people dismiss this, but statin-related muscle and tendon damage is well documented.
Statins block the mevalonate pathway - not just cholesterol production, but pathways essential for muscle-cell energy, repair, and recovery. /2
2/9 The result can be muscle pain, weakness, stiffness, cramps, loss of endurance, and delayed healing.
There is also published evidence linking statins to tendon disorders, including rotator cuff injury (shoulder), Achilles tendon damage, tendonitis, and even tendon rupture. /3
May 16 • 6 tweets • 1 min read
1/6 If you’re the kind of person who needs a peer-reviewed, double-blind, placebo-controlled trial proving fire is hot before you’ll question pharma narratives, this probably isn’t for you.
/22/6 The brain is one of the most cholesterol-dense organs in the human body. Not by accident. Cholesterol is essential for neuronal membranes, synapse formation, myelin production, serotonin receptor function, and cellular signalling. In other words: basic brain function.
/3
May 14 • 12 tweets • 2 min read
1/12 The CoQ10 paradox:
Statins inhibit HMG-CoA reductase to lower cholesterol. but this same pathway is also responsible for endogenous CoQ10 synthesis.
CoQ10 is essential for mitochondrial energy production, especially in tissues with the highest metabolic /2
2/12 demand: skeletal muscle and the heart.
Metabolism is how cells “breathe.” Oxygen delivery is only half the equation - mitochondria require CoQ10 to transfer electrons and generate ATP. Without adequate CoQ10, cellular energy production is impaired. /3
May 11 • 9 tweets • 2 min read
1/9 Please don’t be fooled. Statin damage is not a “side effect.” It is the direct biological consequence of blocking the mevalonate pathway by inhibiting HMG-CoA reductase - the enzyme responsible for producing mevalonate.
/22/9 What is often called “statin intolerance” is evidence of toxicity. Some cells cannot compensate for the mevalonate blockade by increasing reductase activity, and the result is direct cellular damage. Pharmaceutical companies knew this decades ago.
/3
May 8 • 8 tweets • 1 min read
1/8 NNT (Number Needed to Treat) and NNH (Number Needed to Harm) for statins are often presented with surgical precision, as if they describe real, identifiable patients. They don’t.
/22/8 They are statistical artefacts built from trial design choices, group averages, and endpoint definitions - not direct clinical observations.
/3
May 8 • 15 tweets • 3 min read
1/15 I often hear the claim that statins can be “very helpful in secondary prevention” - meaning after a heart attack or stroke, while being far less effective in primary prevention.
But how can that logically be true ? /2
2/15 If a drug genuinely prevents CVD, why would the mechanism suddenly become beneficial only after damage has already occurred ?
If statins truly reduced the underlying risk of CVD, we should expect to see consistent benefit across both primary and secondary prevention. /3
May 5 • 8 tweets • 2 min read
1/8 This 2013 post was written by an administrator of a “statin side effects” forum, sharing her husband’s experience in the hope others may avoid a similar outcome. /22/8 Her husband, now 68, underwent quadruple bypass surgery at age 52 after a stress test revealed a major blockage. Following surgery, he was prescribed statins and blood pressure medication. Previously very active and healthy, he was no longer able to run due to muscle pain. /3
May 4 • 10 tweets • 2 min read
1/10 Challenging the LDL Dogma:
The dominant narrative claims that elevated LDL directly causes atherosclerosis by accumulating in arterial walls and forming plaques. Yet if LDL were truly the primary driver, CVD would track consistently with LDL levels. It does not. /2
2/10 Contradictory clinical reality:
There are documented cases, including those discussed by Dr. Malcolm Kendrick, of individuals with familial hypercholesterolemia and extremely high LDL who show no coronary artery disease even after decades of exposure. /3