
@pennmedicine Heme/Onc Fellow via @UCDmedicine; @thebianchilab; @mayoMN_imres
 #2: West Haven Criteria
#2: West Haven Criteria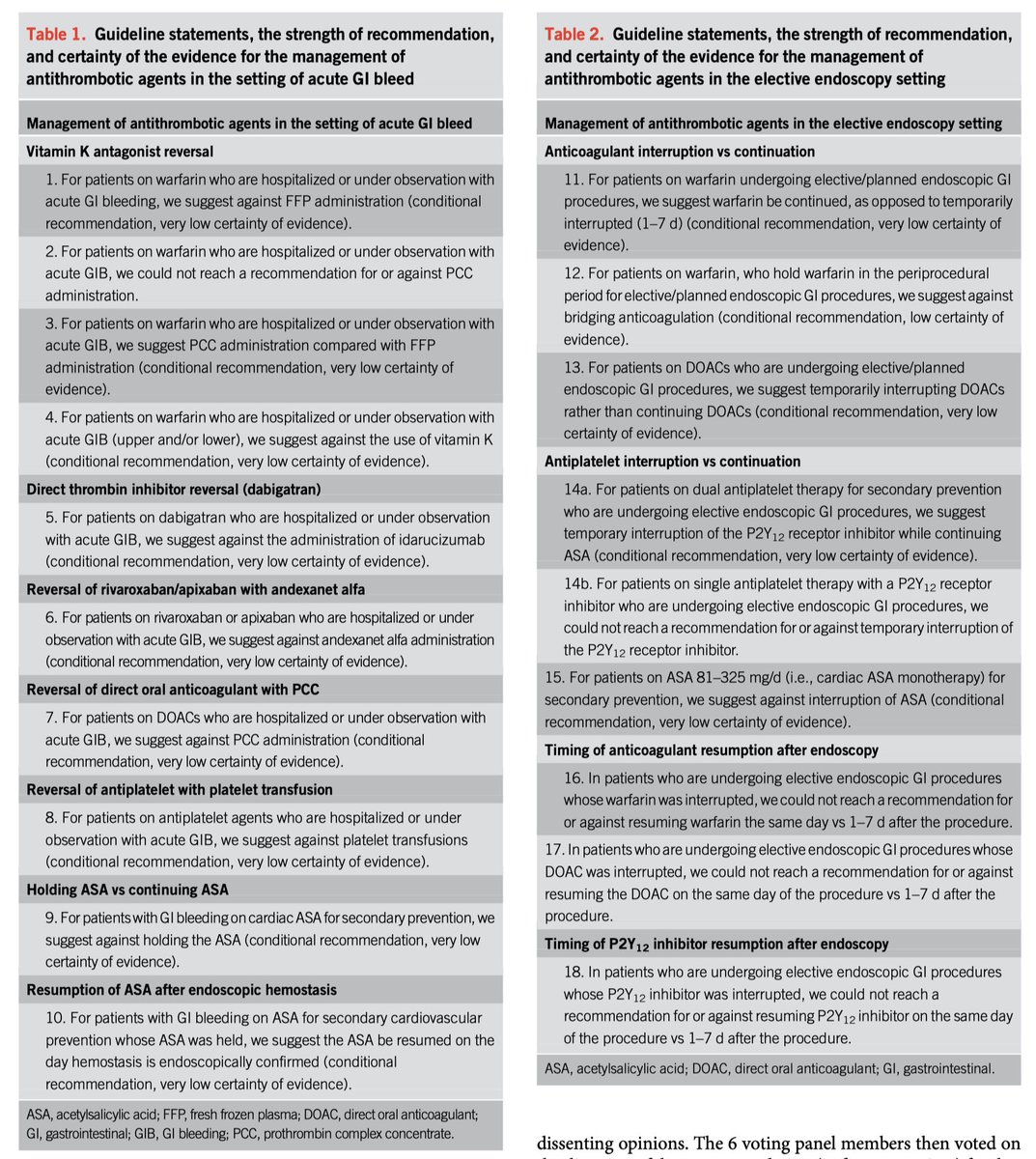 Evidence for continuing (RCT small sample size)
Evidence for continuing (RCT small sample size)
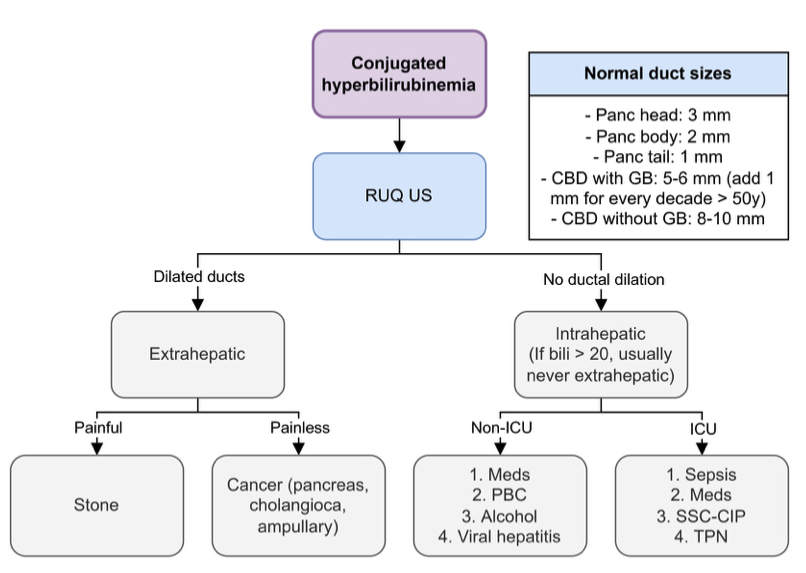
 Bilirubin thresholds:
Bilirubin thresholds: 
 ABG vs VBG:
ABG vs VBG:
 2. Approach to iron deficiency anemia
2. Approach to iron deficiency anemia 