
Director of the Systems Serology Lab at the Ragon Institute of MGH, MIT and Harvard. Personal account. Operates on caffeine, optimism, and baking.
 The Sunday evening cookie chronicles II
The Sunday evening cookie chronicles II 
 Most of them were great questions and I tried to help as best I could; but some questions were bonkers.
Most of them were great questions and I tried to help as best I could; but some questions were bonkers.  This particular adenovirus, Ad26, was likely chosen as antibody prevalence against it is very low in humans. This allows for the presentation of the SARS-2 Spike protein without the neutralization of the vehicle (Ad26). (2/5) jvi.asm.org/content/81/9/4…
This particular adenovirus, Ad26, was likely chosen as antibody prevalence against it is very low in humans. This allows for the presentation of the SARS-2 Spike protein without the neutralization of the vehicle (Ad26). (2/5) jvi.asm.org/content/81/9/4…
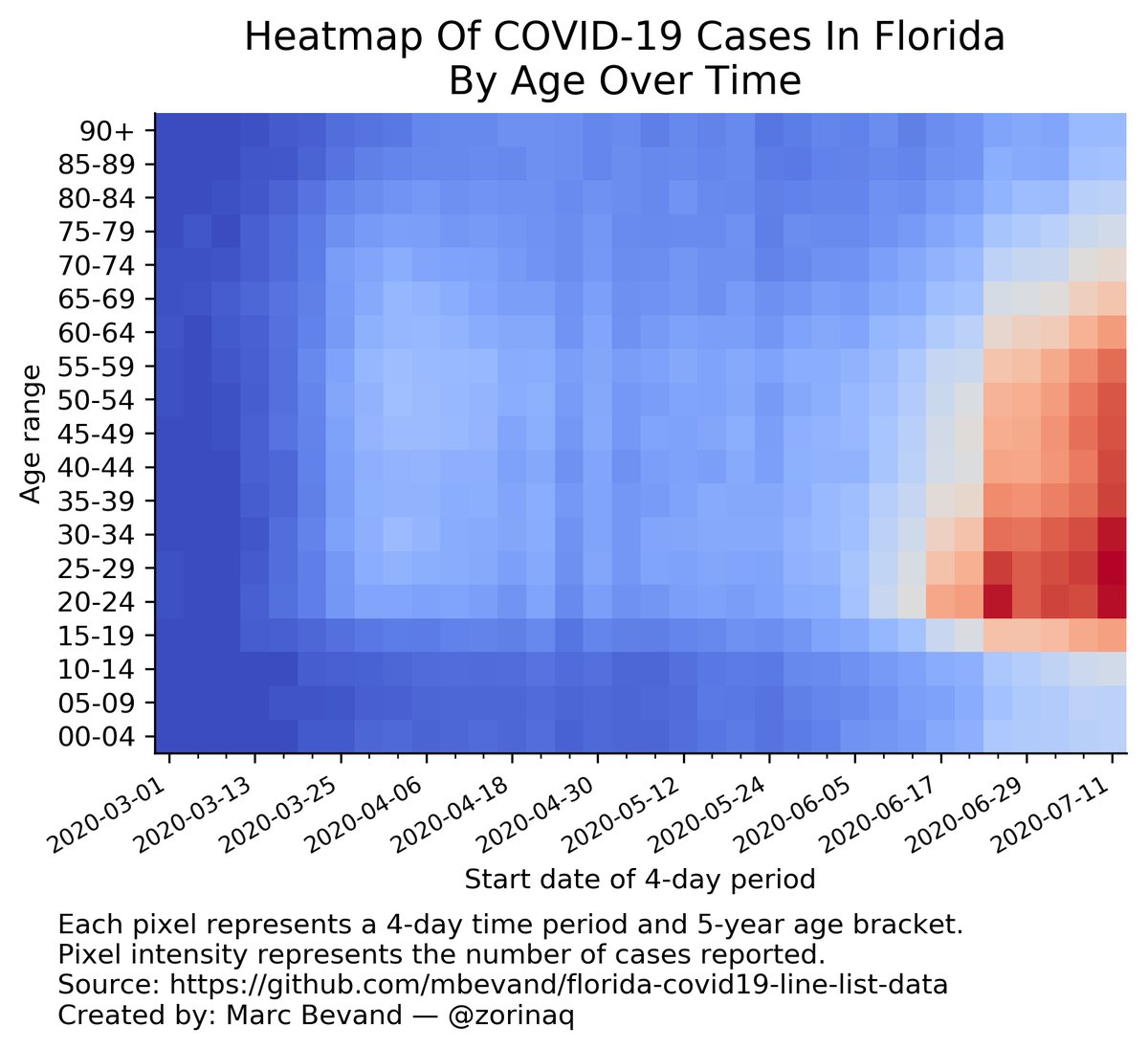
 2) Transmission increased in young adults. This happened in May when young adults saw the biggest spikes in cases.
2) Transmission increased in young adults. This happened in May when young adults saw the biggest spikes in cases. 