
Interop Officer @LDN_Ambulance & @MetPoliceUK | Tactical/Joint Resp Paramedic | Tactical, Mil, Austere & Operational Med MSc | Ex CMT1(v) | Co-Developer #TST
 Users will be divided into:
Users will be divided into: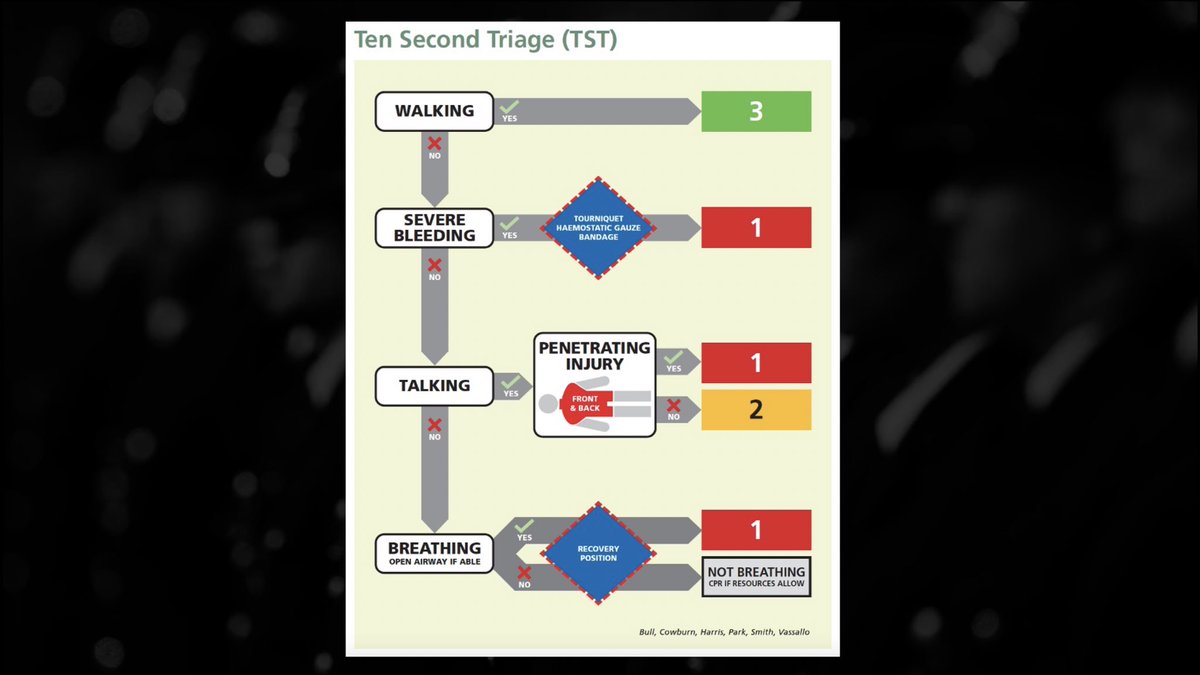 TST is designed as a pan-emergency service early scene triage tool, actively confronting the challenges experienced by tools that have come before it (none of which were good enough)
TST is designed as a pan-emergency service early scene triage tool, actively confronting the challenges experienced by tools that have come before it (none of which were good enough)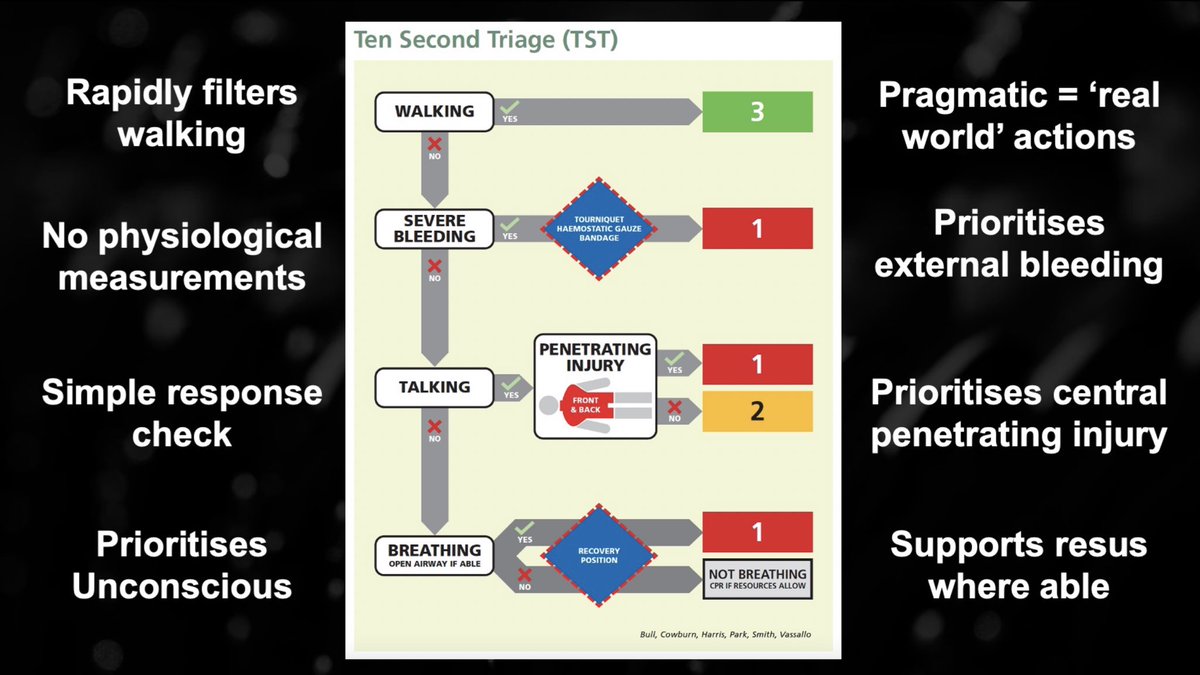

 We will all meet / have met a patient who was saved by a non-uniformed #SpontaneousResponder
We will all meet / have met a patient who was saved by a non-uniformed #SpontaneousResponder