
We are a registered charity promoting education, communication and the sharing of knowledge to ensure safer IV fluid prescribing.
 2/
2/
 2/
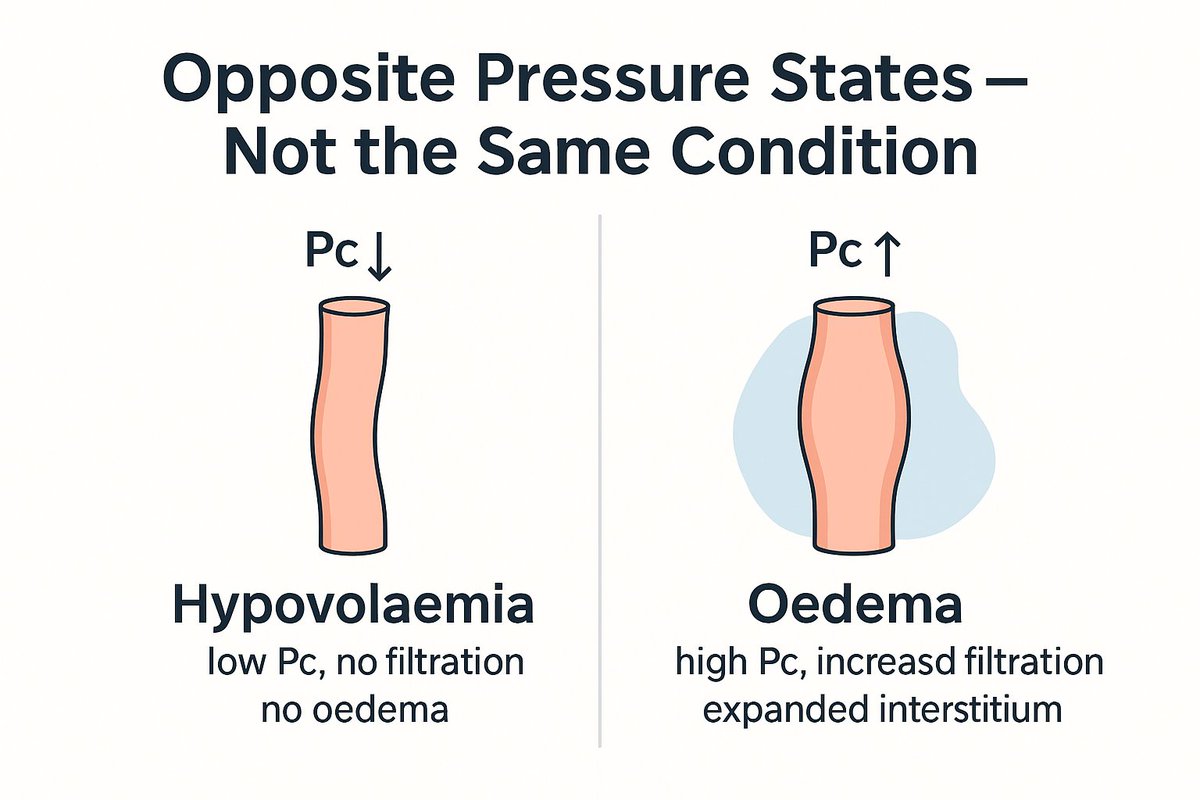
2/ 2/ In our hypovolaemia thread we saw:
2/ In our hypovolaemia thread we saw: 2/
2/ 2/
2/ 2/
2/
 2. Your kidneys have an impressive range — but they need the tools.
2. Your kidneys have an impressive range — but they need the tools.
 2/
2/ 2/
2/ The lungs are uniquely fragile:
The lungs are uniquely fragile: 2/
2/