
Neuro-Interventionist & Neurointensivist, Autodidact, Philomath, Iconoclast, Bibliophile, Technophile, ‘Normie’, Sempiternal scholar (Nerd) & Teacher @ Kochi
2 subscribers
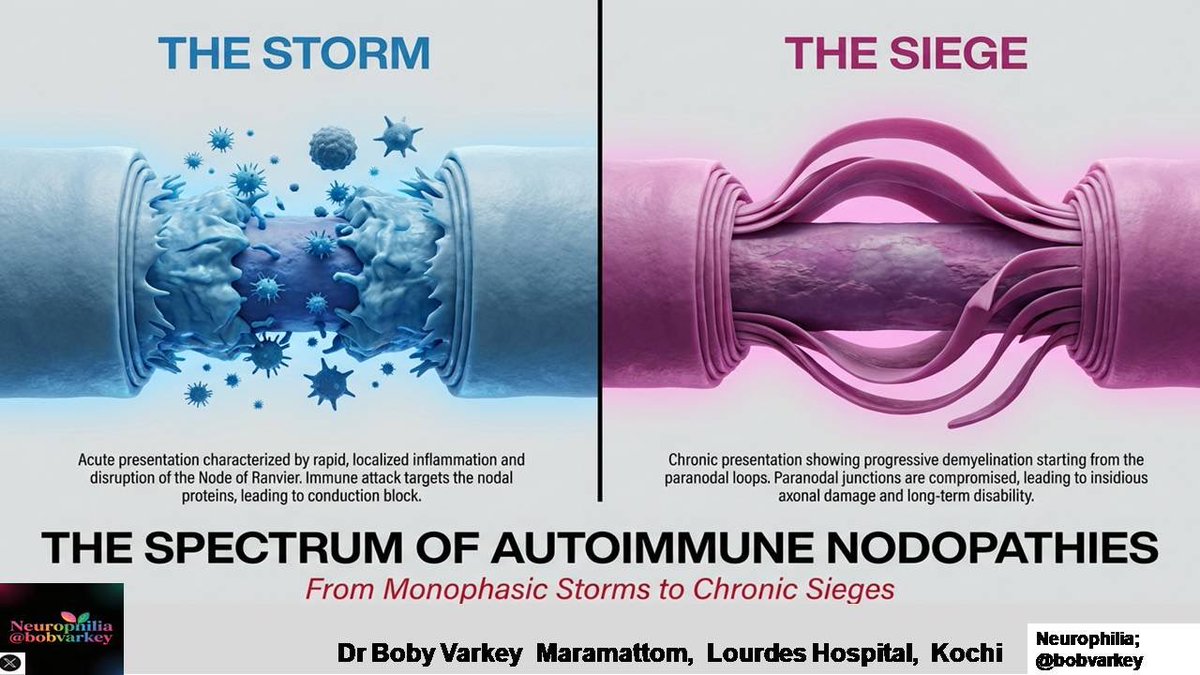
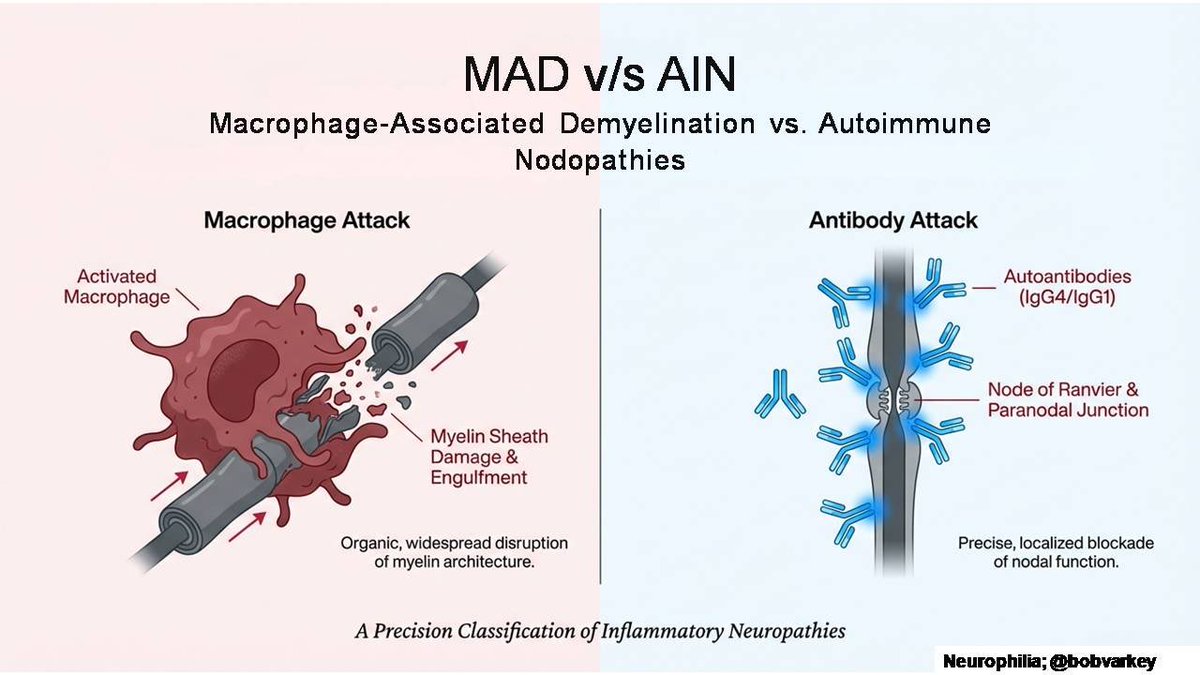
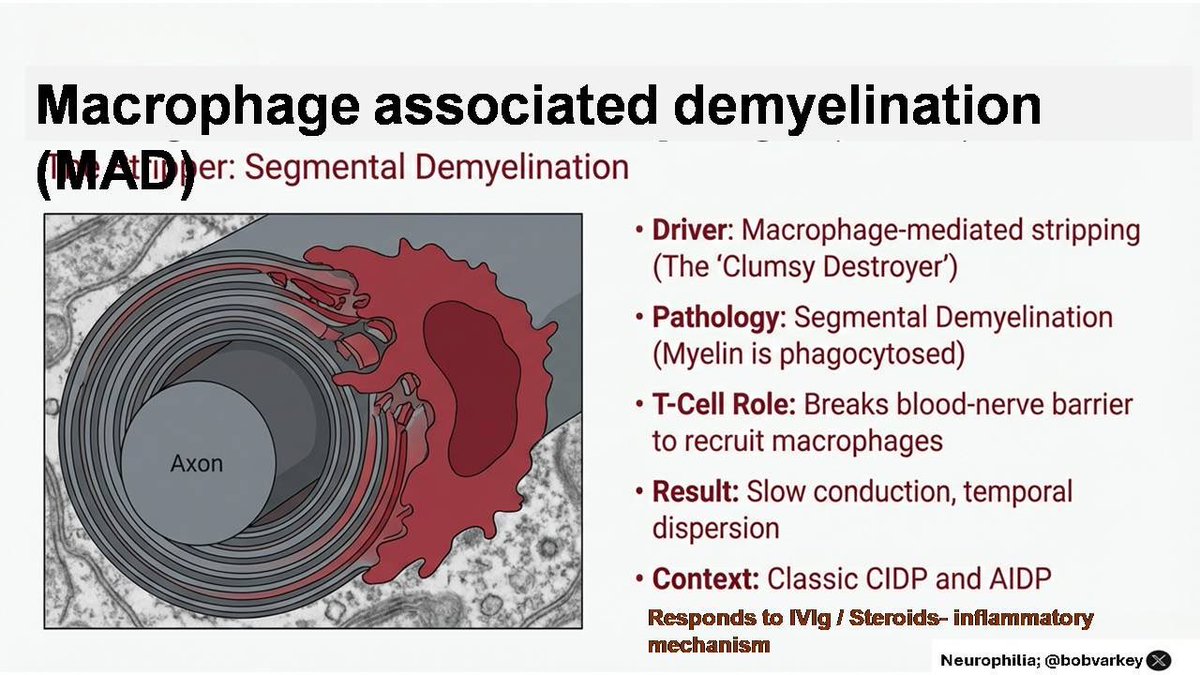 Florid macrophage infiltration in between myelin lamellae and T cell recruitment lead to segmental demyelination. Due to antigenic mimicry, the Schwann cells themselves undergo differentiation into an inflammatory demyelinating subtype (iDSc) which invites macrophages and T cells and unravels the myelin lamellae for them to jump in and chew away
Florid macrophage infiltration in between myelin lamellae and T cell recruitment lead to segmental demyelination. Due to antigenic mimicry, the Schwann cells themselves undergo differentiation into an inflammatory demyelinating subtype (iDSc) which invites macrophages and T cells and unravels the myelin lamellae for them to jump in and chew away
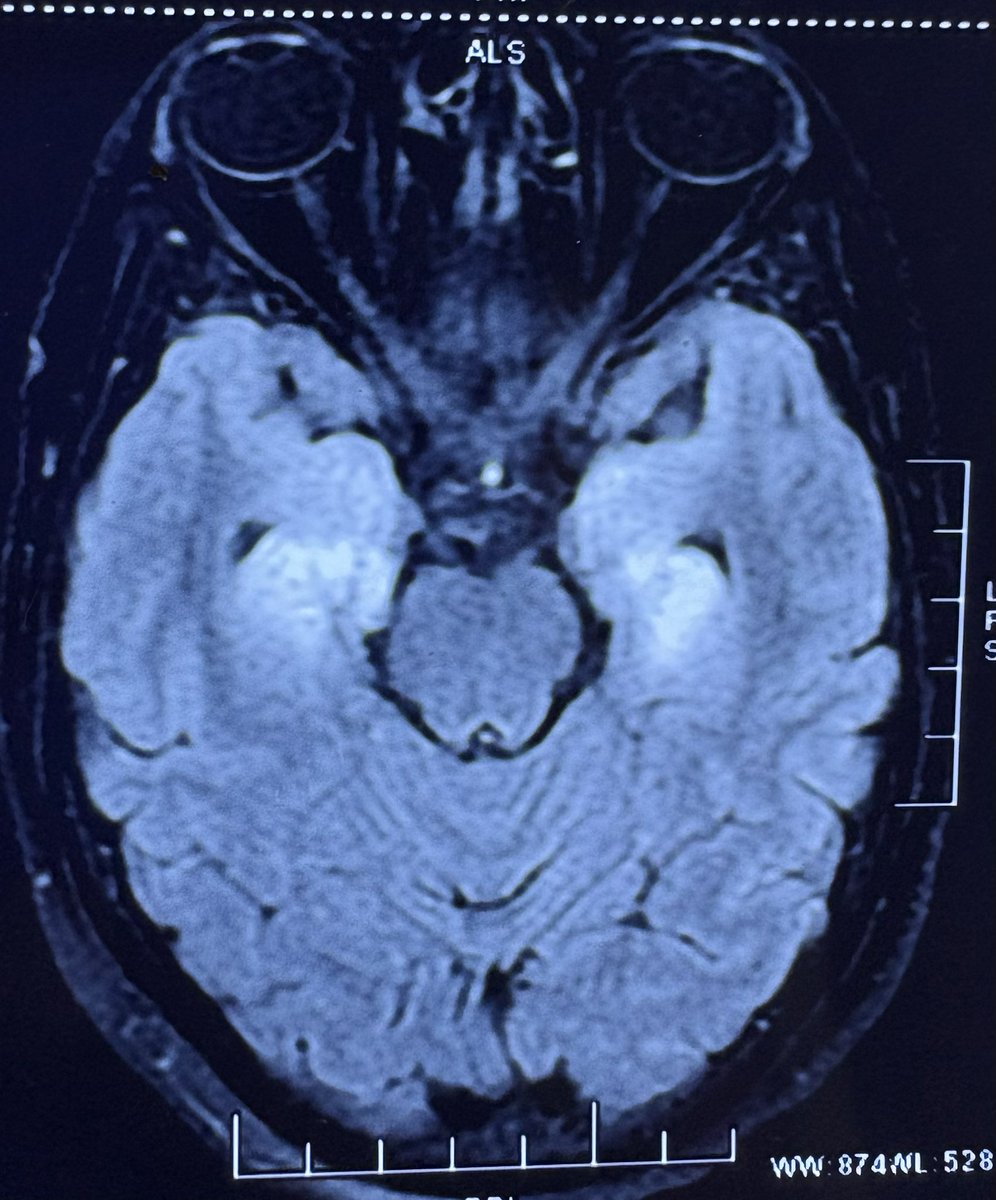
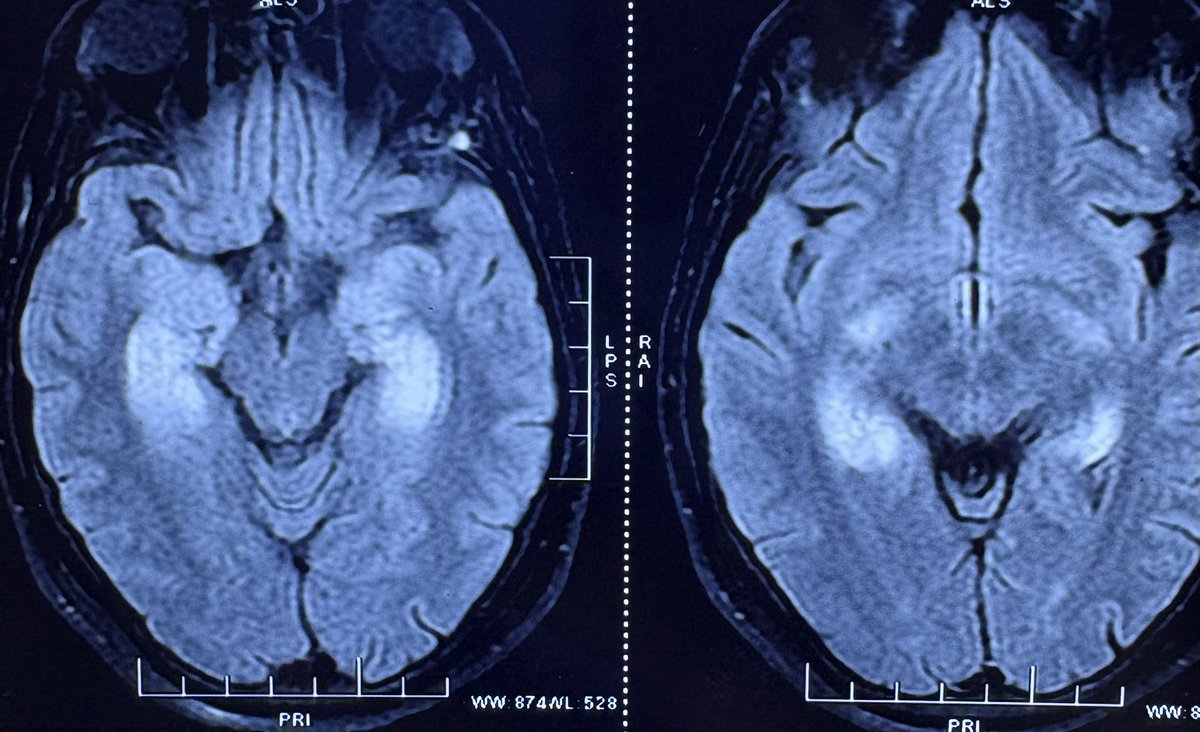 A diagnosis of limbic encephalitis was made. She was started on IVIG x 5 days. HbA1c was 6.4%. An autoimmune encephalitis panel and PET CT turn up negative. She comes for a second opinion. After admission her blood sugar is noted to be 500 mg 🍩🍩🍭
A diagnosis of limbic encephalitis was made. She was started on IVIG x 5 days. HbA1c was 6.4%. An autoimmune encephalitis panel and PET CT turn up negative. She comes for a second opinion. After admission her blood sugar is noted to be 500 mg 🍩🍩🍭


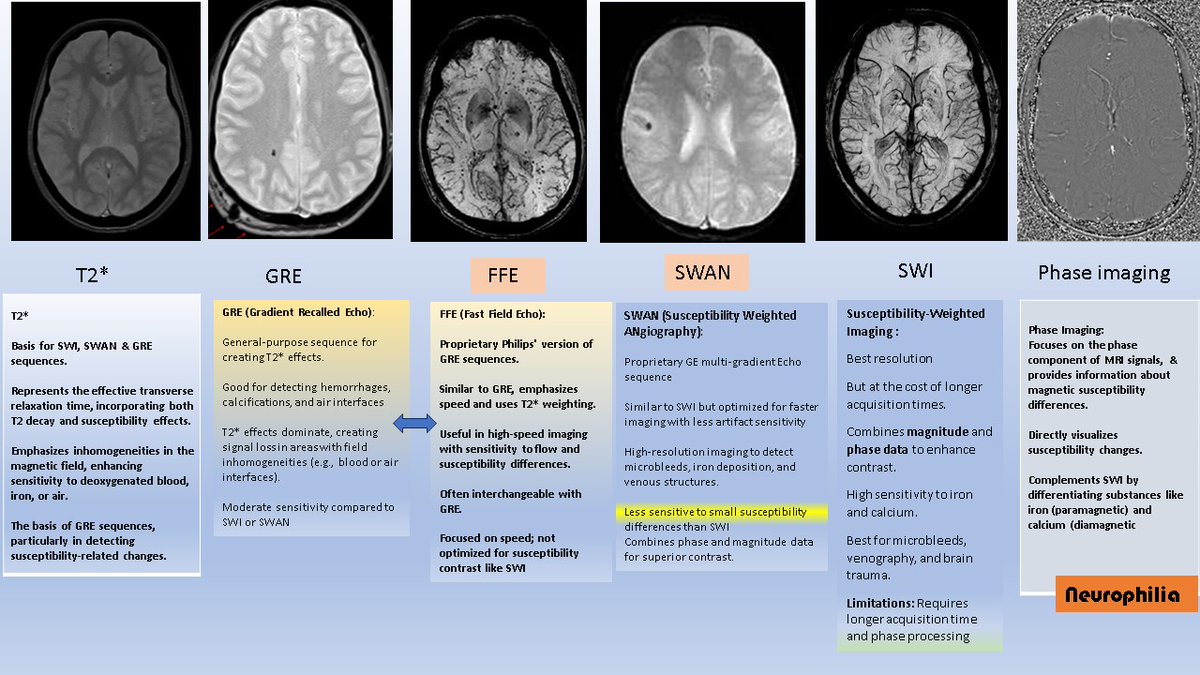 SWAN or GRE may be enough for the majority of MRI aficionados [as they require shorter acquisition times]
SWAN or GRE may be enough for the majority of MRI aficionados [as they require shorter acquisition times]

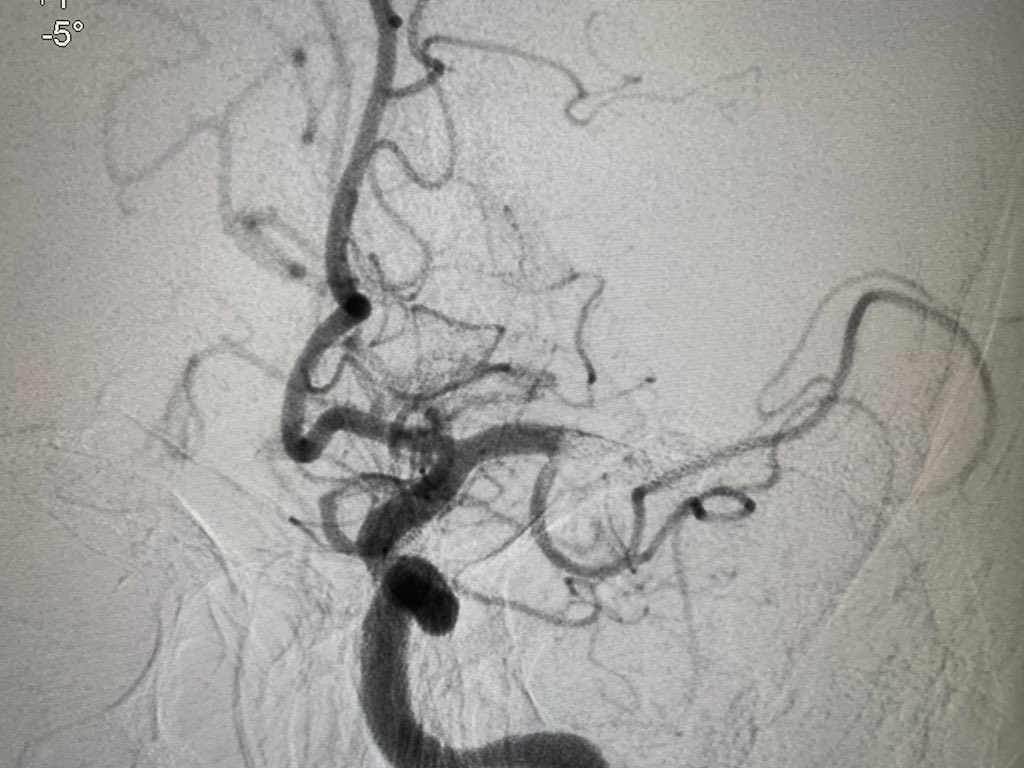
 The MCA can be conveniently divided into 4 segments, each of which moves in a different direction.
The MCA can be conveniently divided into 4 segments, each of which moves in a different direction.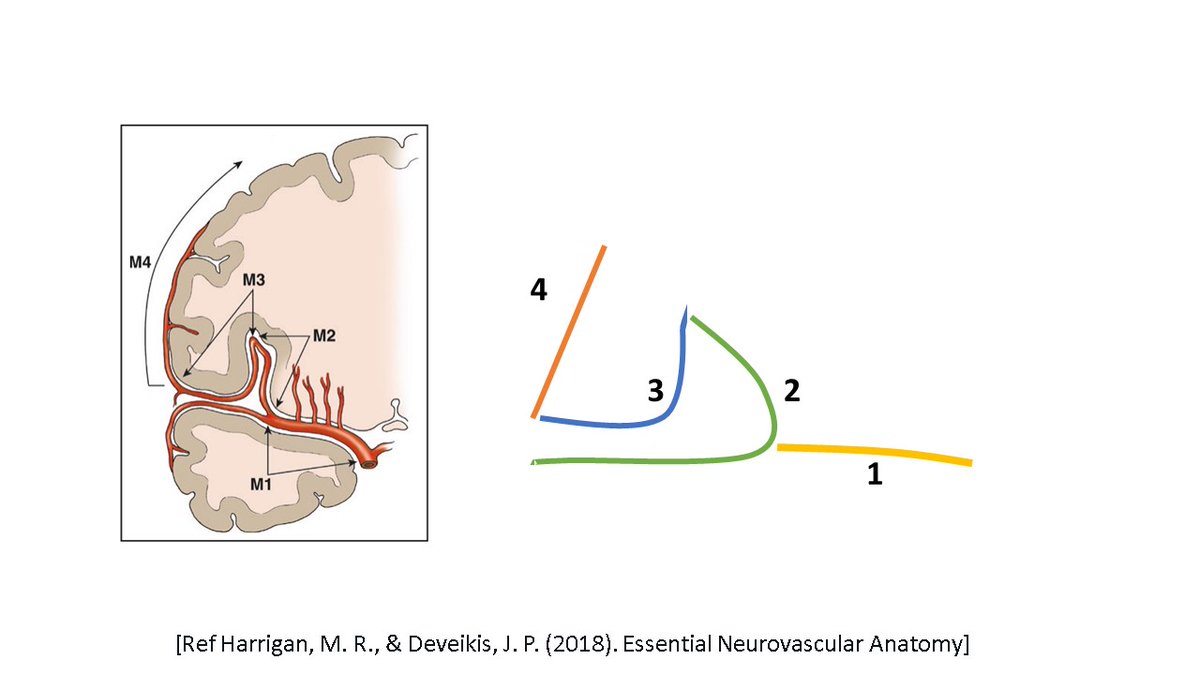

 This is how the normal artery progresses from a fatty streak to total occlusion
This is how the normal artery progresses from a fatty streak to total occlusion 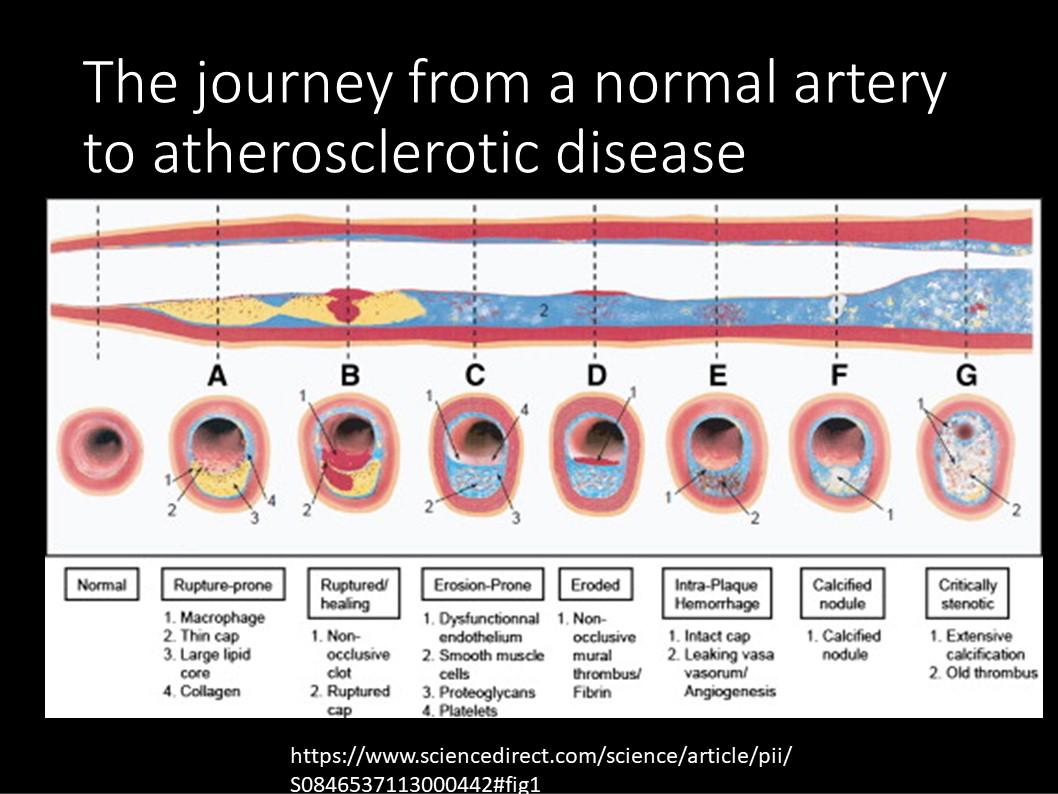
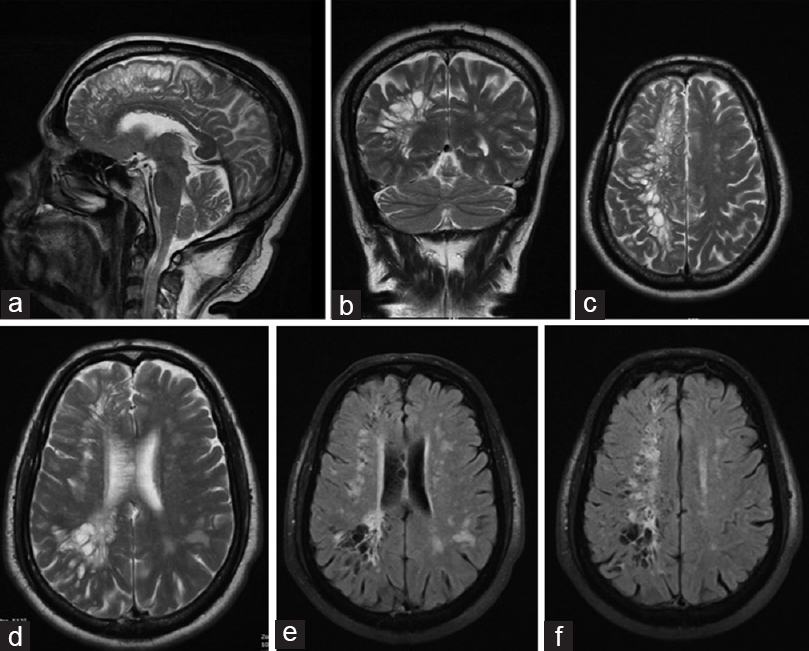
 MRI in leukemia-often;
MRI in leukemia-often;
 ESR 31mm/hr. Blood counts normal after Abx for urosepsis. r/w head CT shows small calcific lesion in front of the odontoid
ESR 31mm/hr. Blood counts normal after Abx for urosepsis. r/w head CT shows small calcific lesion in front of the odontoid 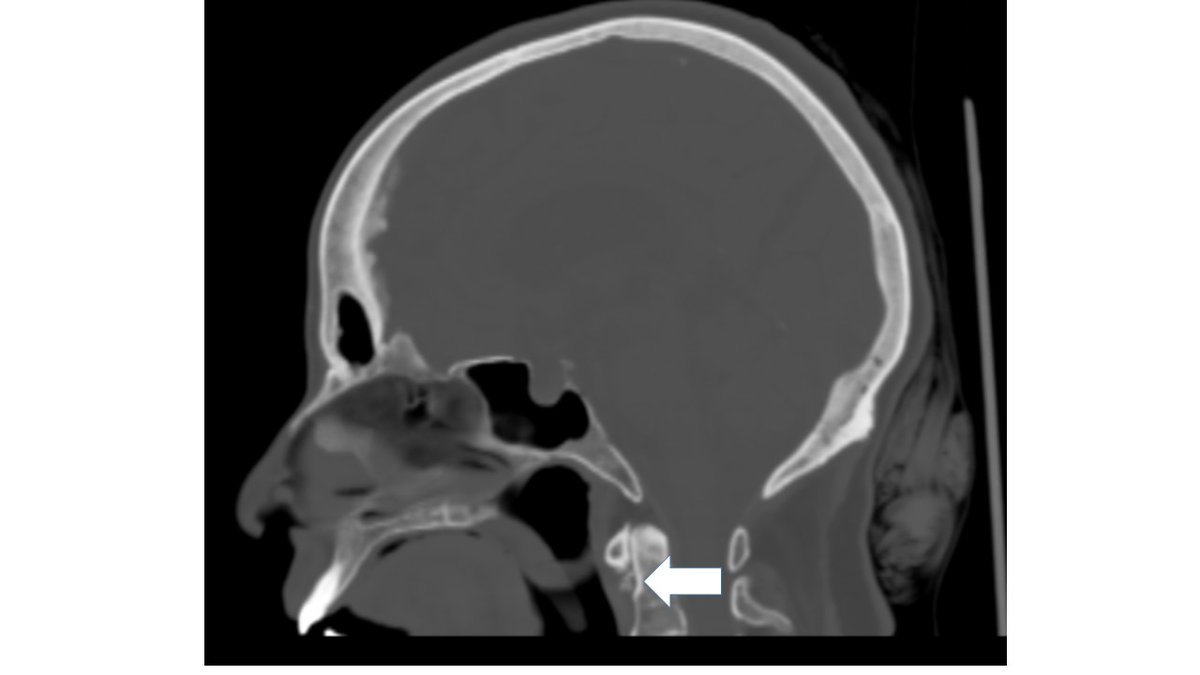

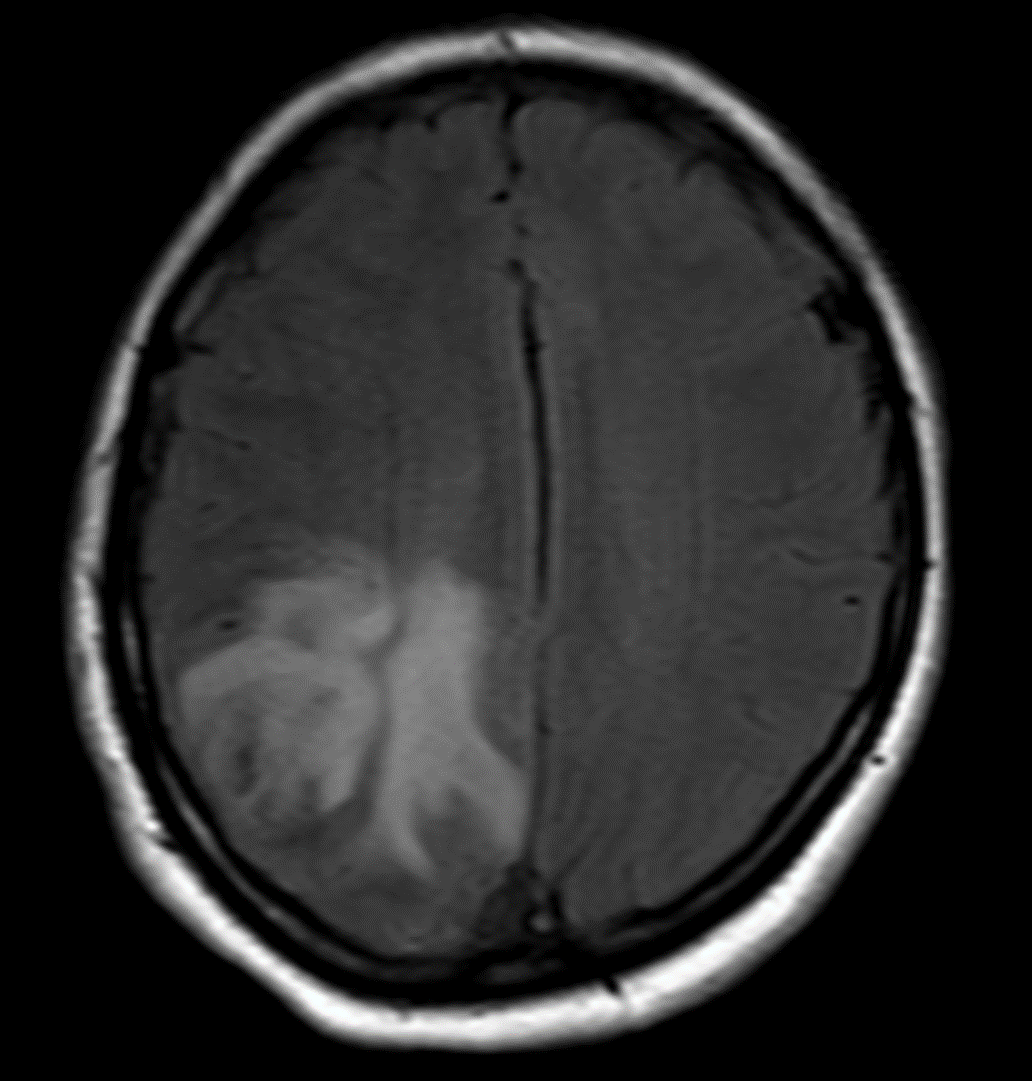
 MRV shows left Transverse and sigmoid sinus thrombosis. No improvement after 2 days of IV heparin. Pt requires heavy sedation, ventilation for headache/agitation.
MRV shows left Transverse and sigmoid sinus thrombosis. No improvement after 2 days of IV heparin. Pt requires heavy sedation, ventilation for headache/agitation.
 Acute dystonic tremor is an exceedingly rare manifestation of a stroke. This patient had ulnar deviation, finger flexion at MCP jts and postural tremors with mild right hand weakness.
Acute dystonic tremor is an exceedingly rare manifestation of a stroke. This patient had ulnar deviation, finger flexion at MCP jts and postural tremors with mild right hand weakness.
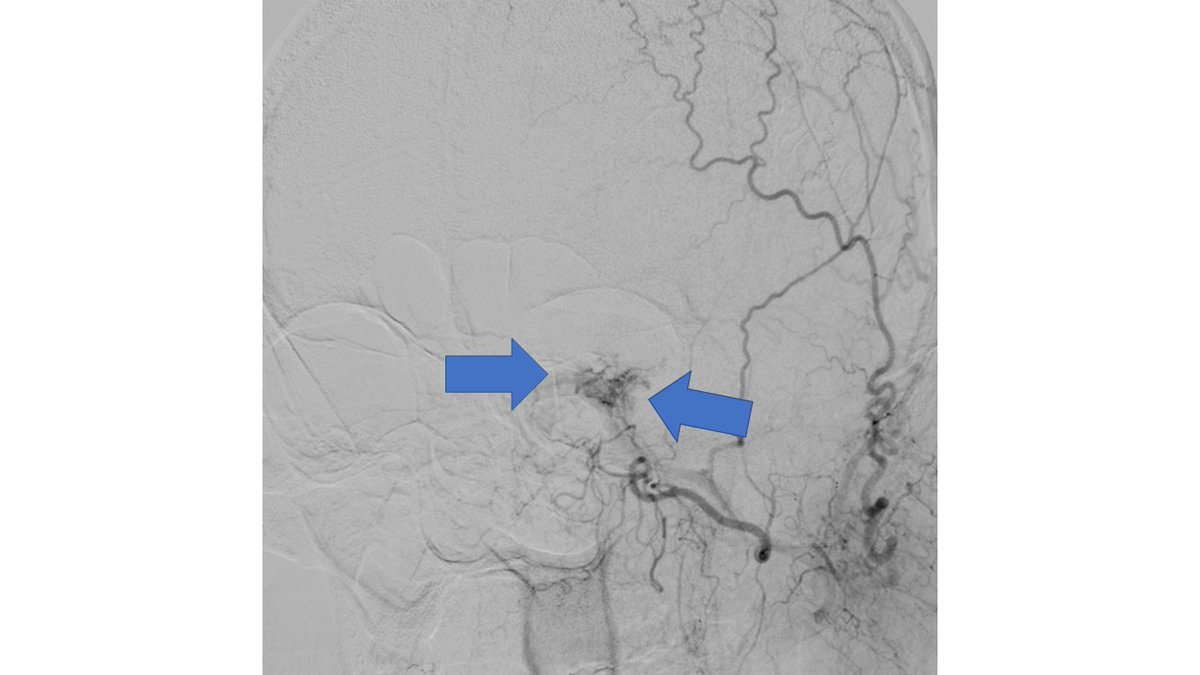
 DSA also confirmed the extensive clot. In view of her recent LSCS 20 days ago, we were hesitant about giving IV lytics (urokinase infusion). Hence went in with an ACE 5 Max catheter and sucked out a mountain of clot
DSA also confirmed the extensive clot. In view of her recent LSCS 20 days ago, we were hesitant about giving IV lytics (urokinase infusion). Hence went in with an ACE 5 Max catheter and sucked out a mountain of clot 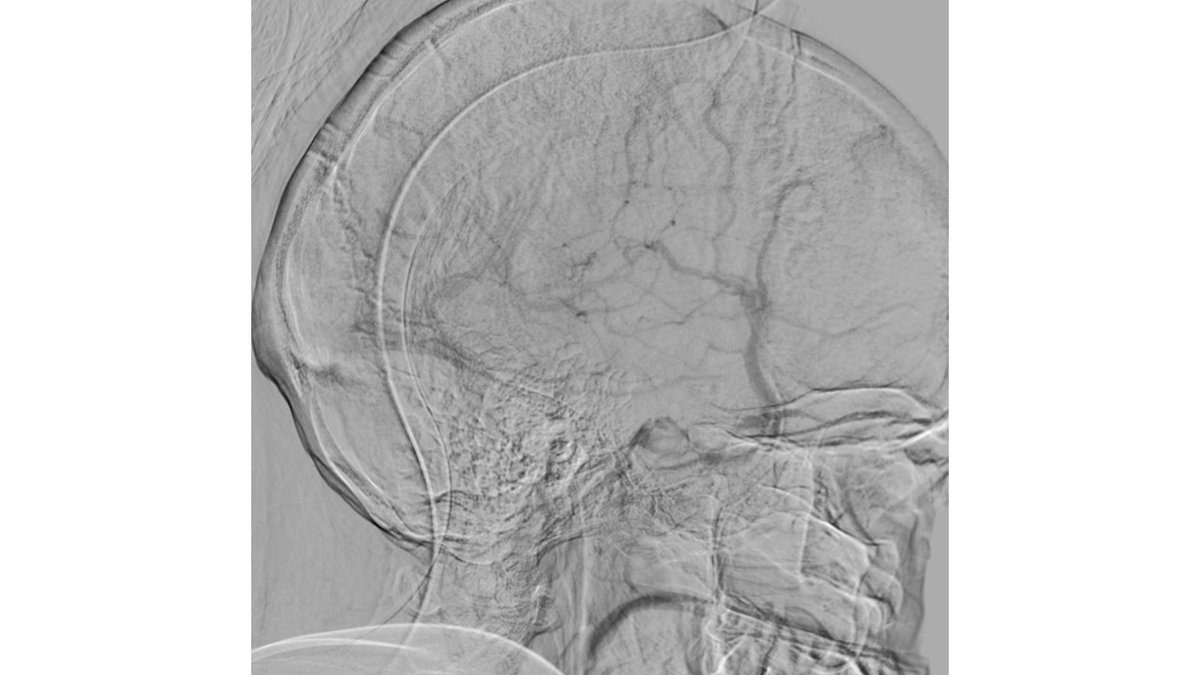

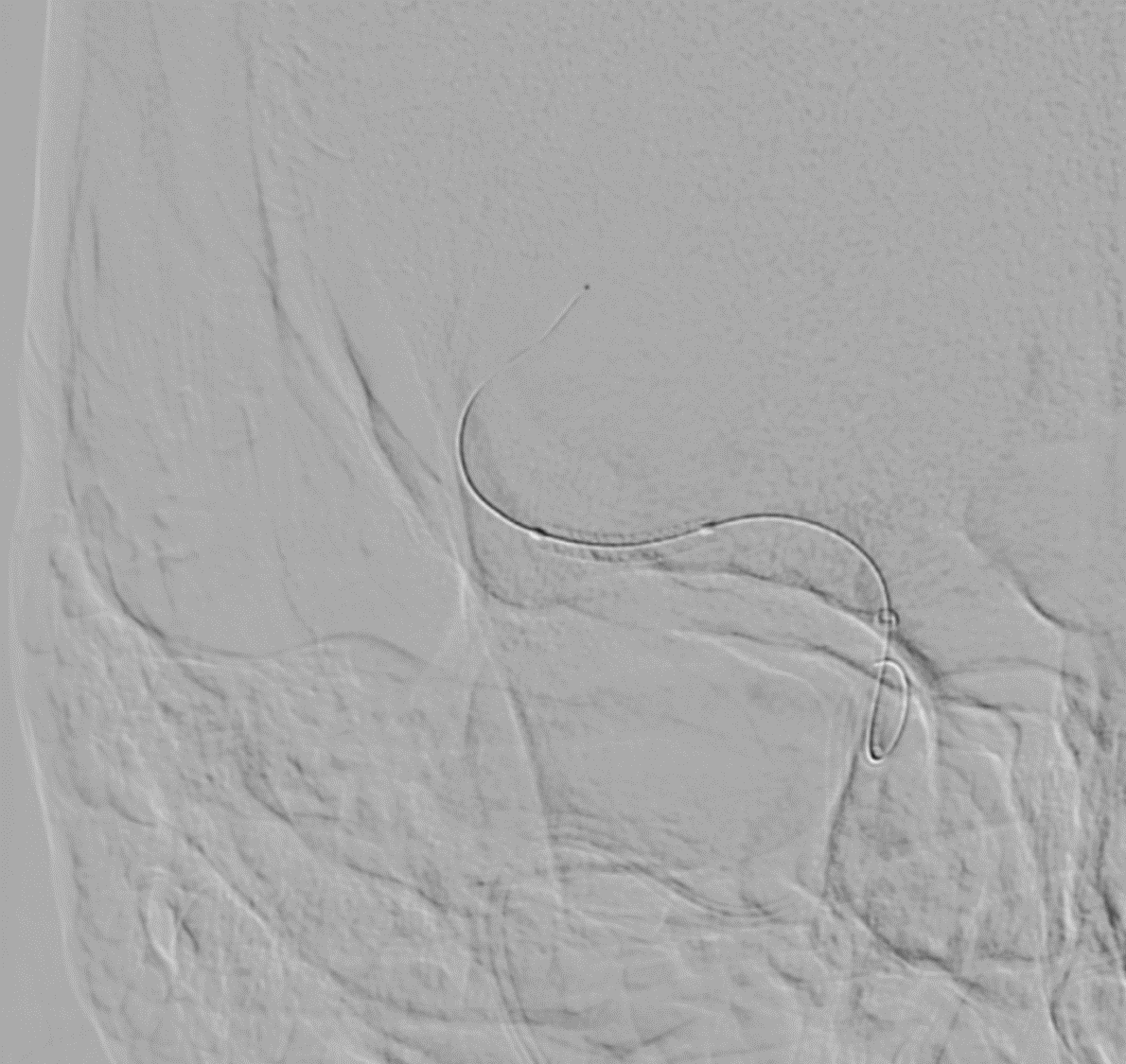 Tight stenosis opened up with a Balloon mounted stent and final result
Tight stenosis opened up with a Balloon mounted stent and final result 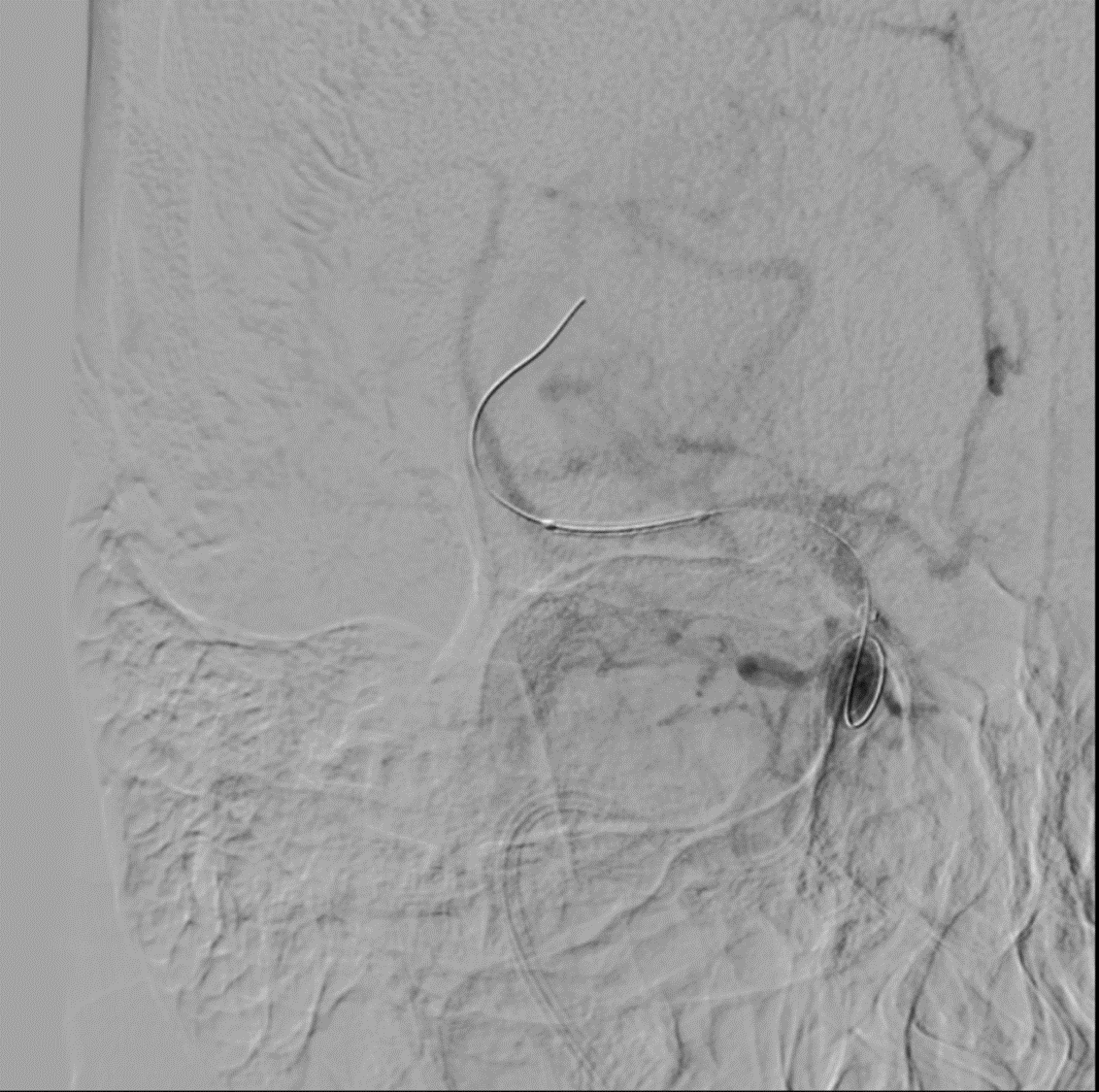

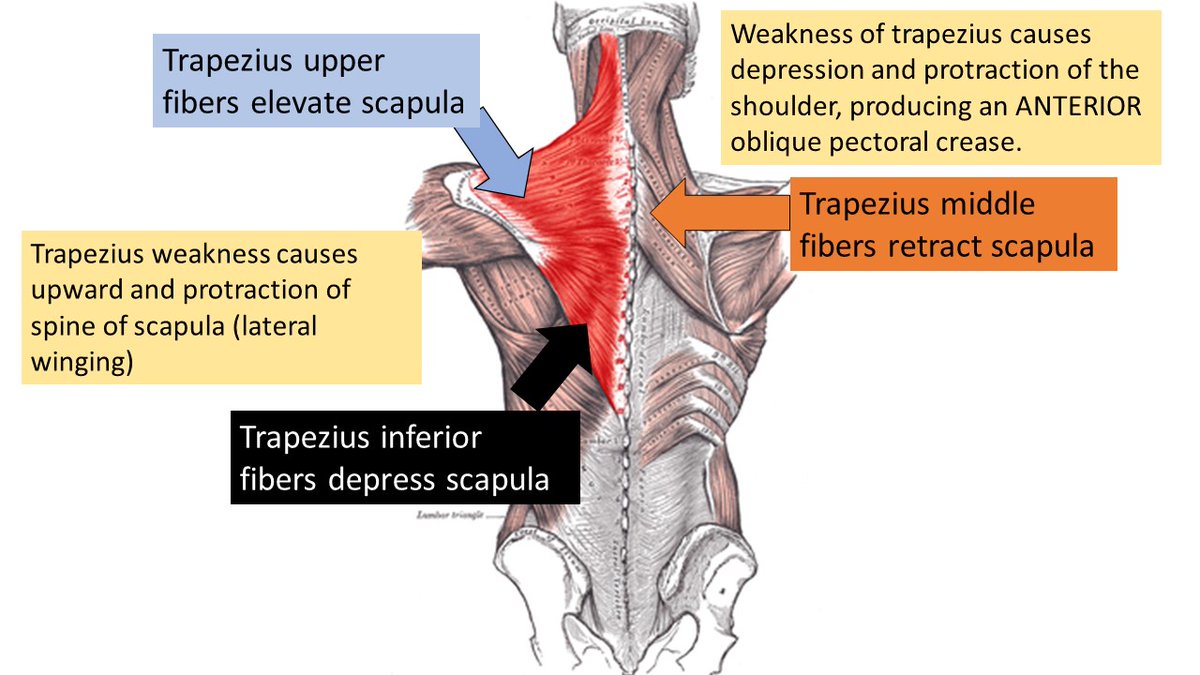
 Quick recap of various scapular movements and the role of the Trapezius in stabilising the scapula
Quick recap of various scapular movements and the role of the Trapezius in stabilising the scapula 
 5 attempts at aspiration + stent retriever -only some red and white clots come out ➡️mTICI score still Zero
5 attempts at aspiration + stent retriever -only some red and white clots come out ➡️mTICI score still Zero 
 A 71-year-old man presented to us with right-sided headache after a flight. Immediately after ascent, he developed severe right eye pain and headache and lost consciousness.
A 71-year-old man presented to us with right-sided headache after a flight. Immediately after ascent, he developed severe right eye pain and headache and lost consciousness.
