
Husband to @monanniecakes| Intensivist @nhsbartshealth| Ultrascoundrel |#FOAMed|@thosewecarry|@ics_updates|@wicsbottomline|@esicm|@tea_empathynhs| 🇳🇬
 This is a difficult presentation to do as I have multiple conflicts of interest related to #POCUS - here they are:
This is a difficult presentation to do as I have multiple conflicts of interest related to #POCUS - here they are: 
 @yourICM @AVBmir @chiara_robba @avkwong After Delphi a decent consensus was reached- here are some summaries
@yourICM @AVBmir @chiara_robba @avkwong After Delphi a decent consensus was reached- here are some summaries





 @RKleinpell Our changed visitation policies had…consequences #lives2021
@RKleinpell Our changed visitation policies had…consequences #lives2021 

 @HalliePrescott Recommends learning from Jean-Luc Dumont on scientific communication presentationzen.com/presentationze…
@HalliePrescott Recommends learning from Jean-Luc Dumont on scientific communication presentationzen.com/presentationze… @remap_cap Preprint available here
@remap_cap Preprint available here
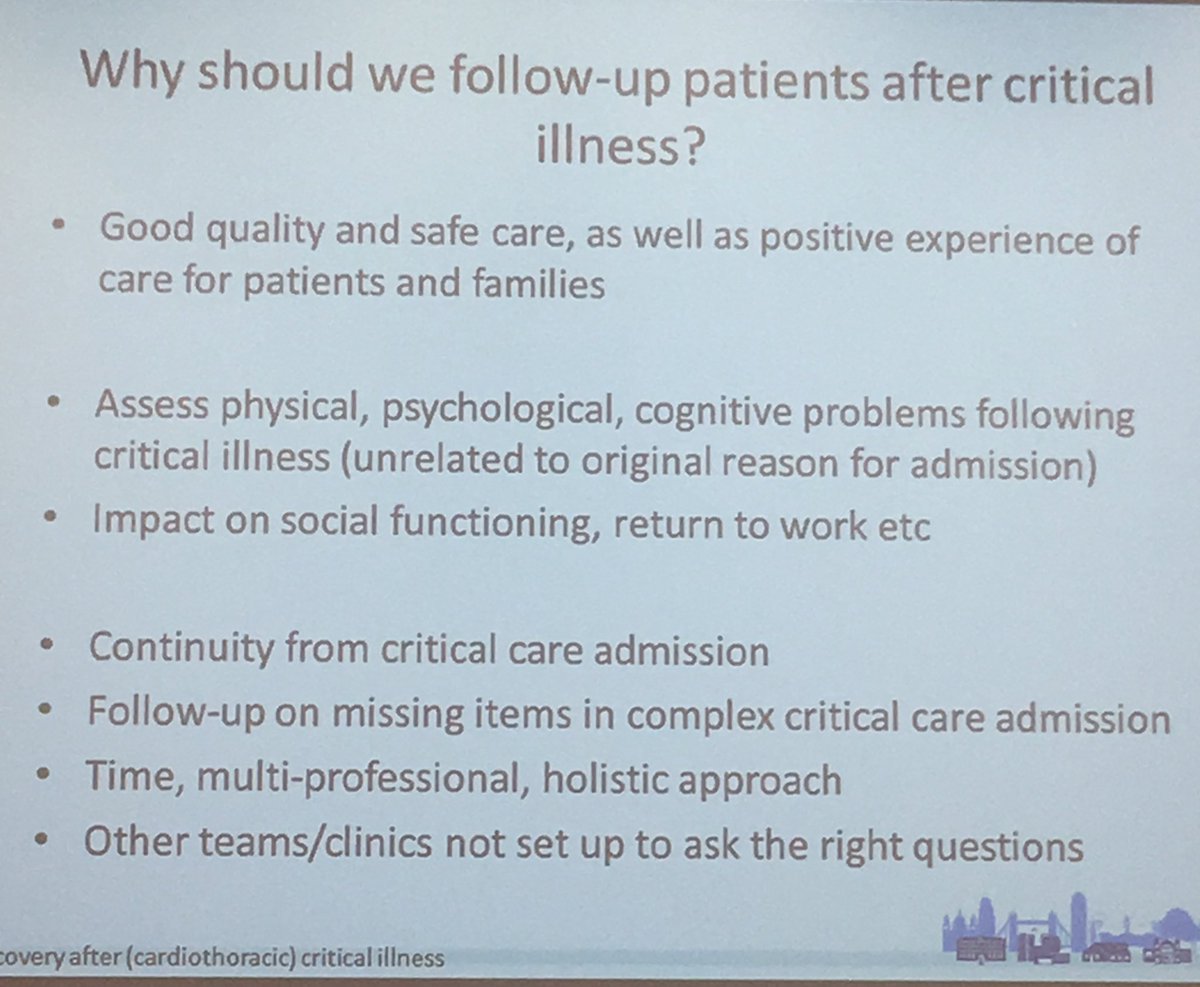 I’m not even sure ICU “survivor” is the right word.
I’m not even sure ICU “survivor” is the right word.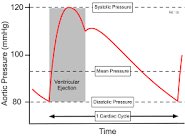
 The fall in Sepsis mortality hasn’t coincided with the introduction of the guidelines #lives2018 🤔
The fall in Sepsis mortality hasn’t coincided with the introduction of the guidelines #lives2018 🤔 
 And as if by magic in a parallel stream... #lives2018
And as if by magic in a parallel stream... #lives2018
 Marlies starts with a couple of case histories:
Marlies starts with a couple of case histories: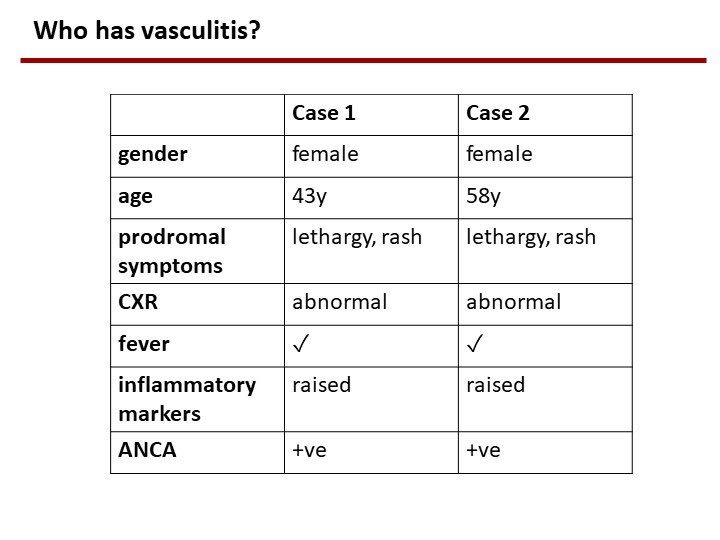
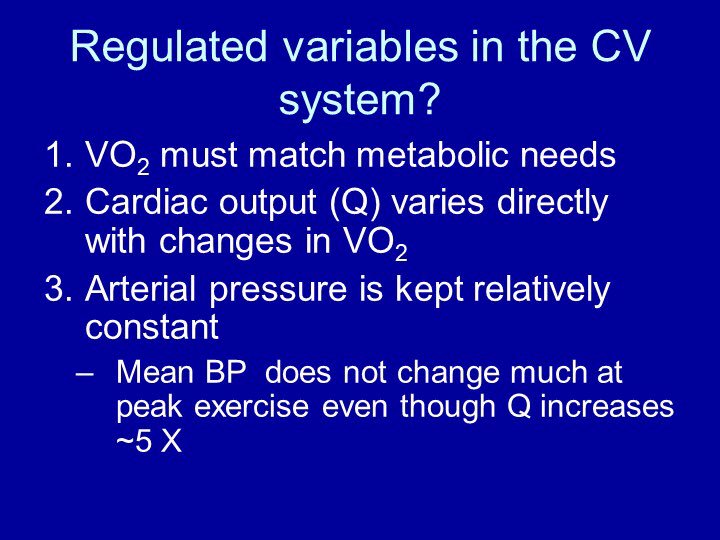 “a compliant system is necessary for pulsation flow”- S Magder
“a compliant system is necessary for pulsation flow”- S Magder