POCUS, NBE CCE diplomat, Echo, Resuscitation, VExUS, Emergency Medicine, 🏴




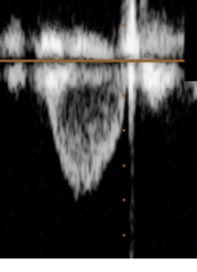
 RVOT VTI after milrinone/epoprostenol medneb:
RVOT VTI after milrinone/epoprostenol medneb: 
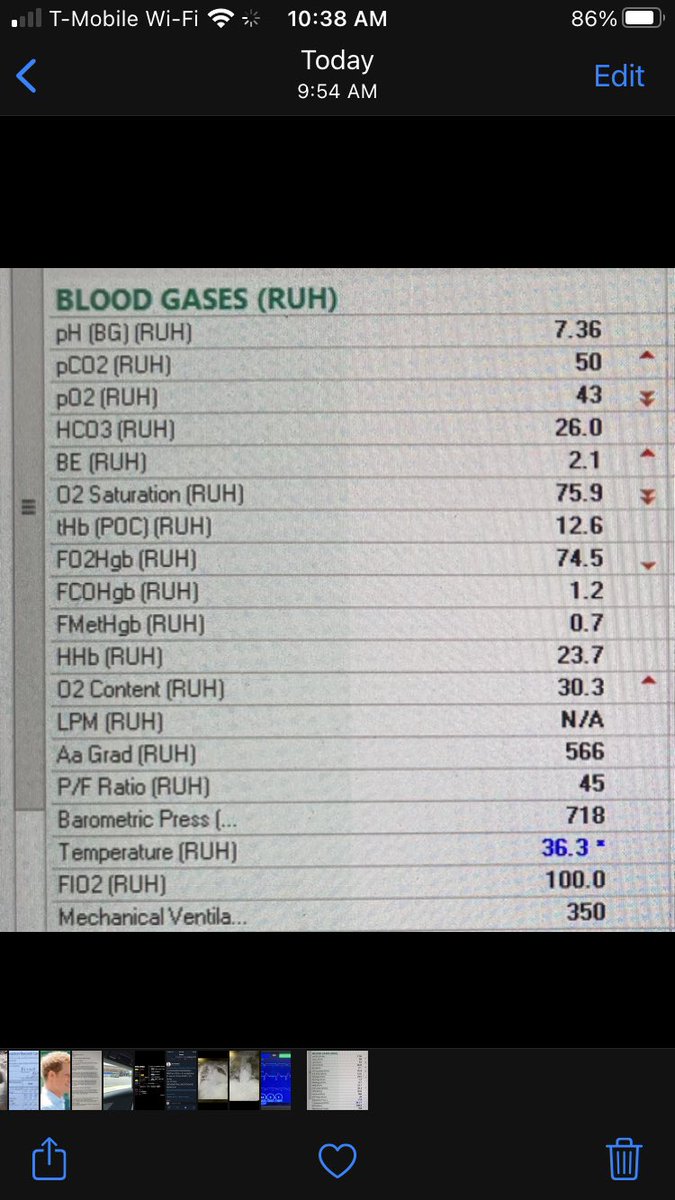
 2/ Initial vent settings were with 6cc/kg TV. Initial ABG on FiO2 100% is seen below.
2/ Initial vent settings were with 6cc/kg TV. Initial ABG on FiO2 100% is seen below.