
Solving problems with technology. Chief Clinical Information Officer, Consultant Neurologist, Chair Welsh Technical Standards Board, Developer, Researcher.
 1. The same data can be used for direct care, service management, continuous improvement, audit governance, and research if we do our job right. Different levels of granularity, and governance wrap, but we artificially separate these.
1. The same data can be used for direct care, service management, continuous improvement, audit governance, and research if we do our job right. Different levels of granularity, and governance wrap, but we artificially separate these. 
 The conventional approach means thinking in terms of applications, and not data, and is centred on organisations / providers, not the patient, or the wider ‘service’. Architecturally, it is a monolith, at least to outsides, and proprietary and organisationally-centric.
The conventional approach means thinking in terms of applications, and not data, and is centred on organisations / providers, not the patient, or the wider ‘service’. Architecturally, it is a monolith, at least to outsides, and proprietary and organisationally-centric. 
 If you look carefully, I’m asking for attributes - but I’m drilling into those and having my queries resolved by multiple microservices; this is a federated distributed electronic health record. We start at an edge and navigate seamlessly. Notice how I can resolve ethnicity and
If you look carefully, I’m asking for attributes - but I’m drilling into those and having my queries resolved by multiple microservices; this is a federated distributed electronic health record. We start at an edge and navigate seamlessly. Notice how I can resolve ethnicity and

 Most us of recognise that health and care need to provide a suite of computing & data services forming a platform on which a range of user-centred solutions can be built, underpinned by robust open standards?
Most us of recognise that health and care need to provide a suite of computing & data services forming a platform on which a range of user-centred solutions can be built, underpinned by robust open standards? 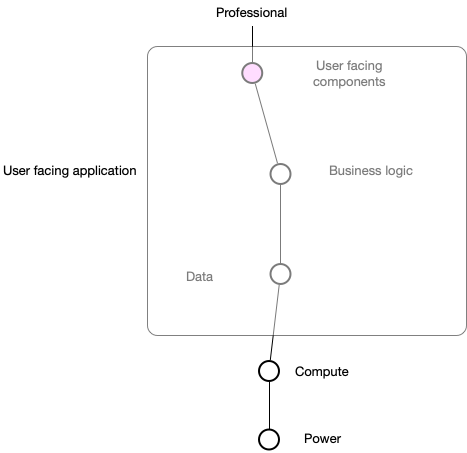
 Firstly, I’m sure that we all agree that we want to create a seamless patient-centred service that blurs the boundaries between disciplines and organisations across health and care. Likewise, we surely recognise that technology is an enabler of those ambitions.
Firstly, I’m sure that we all agree that we want to create a seamless patient-centred service that blurs the boundaries between disciplines and organisations across health and care. Likewise, we surely recognise that technology is an enabler of those ambitions.
