MD, PhD. Harvard, Oxford. Educator. Professional Guinea Pig. StayCurious Metabolism Letter, Top Best-Seller in Science 🔗 https://t.co/YoPdkV719L
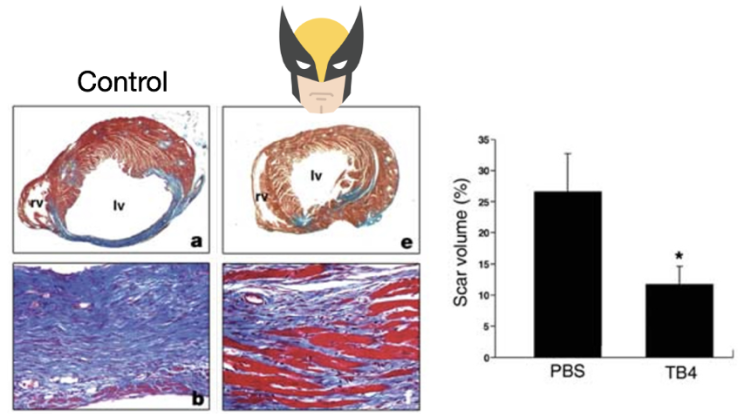 2/6) Since I’ve covered BPC-157 at length before, let’s focus on TB4.
2/6) Since I’ve covered BPC-157 at length before, let’s focus on TB4.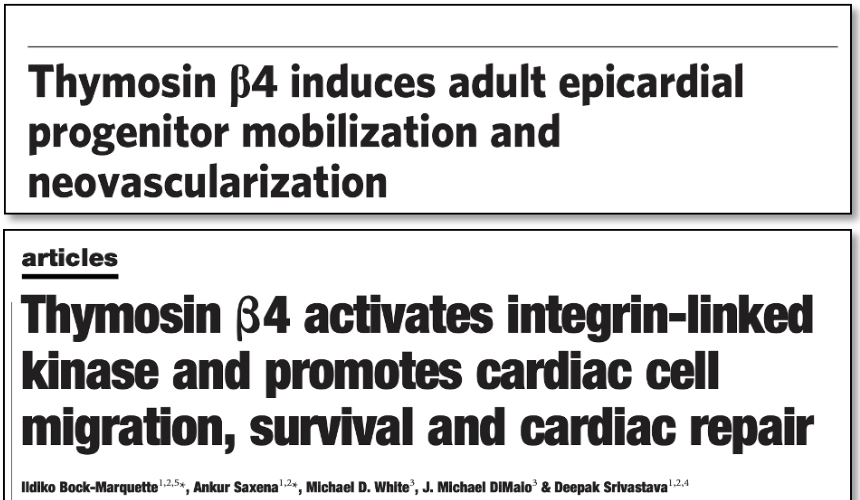
 2/7) Here’s a remarkable fact: You can feed your gut even when you’re not eating.
2/7) Here’s a remarkable fact: You can feed your gut even when you’re not eating.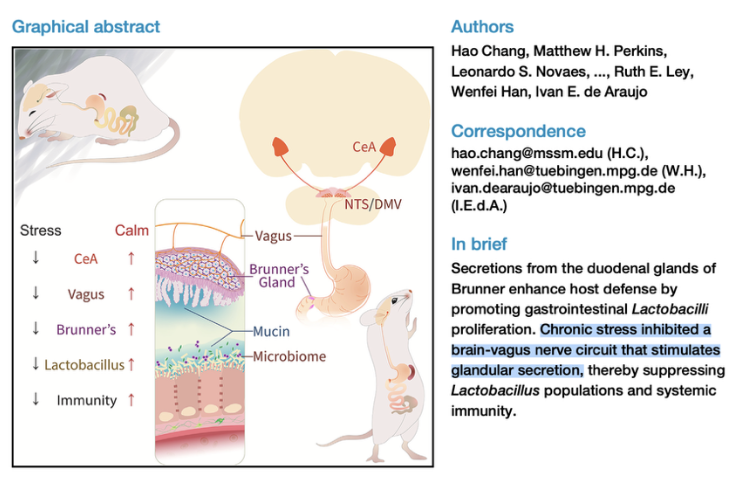
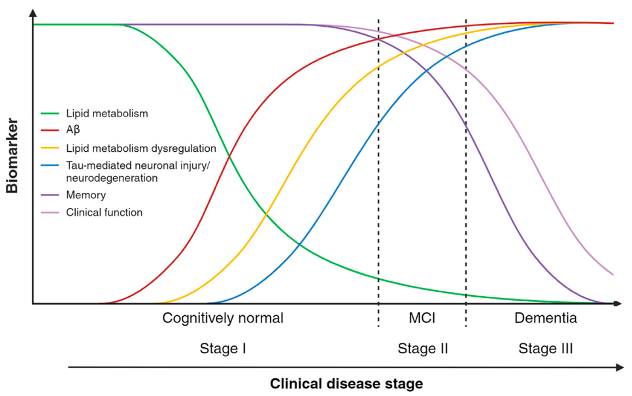
 2/7) Starting with brain health. Higher GLP-1 signaling appears associated with less amyloid in the human brain.
2/7) Starting with brain health. Higher GLP-1 signaling appears associated with less amyloid in the human brain.
 2/7) The mechanism centers on one of the body’s master metabolic regulators: AMPK.
2/7) The mechanism centers on one of the body’s master metabolic regulators: AMPK.
 2/5) Let’s start with something free:
2/5) Let’s start with something free:
 2/5) Tesamorelin is a growth hormone-releasing hormone (GHRH) analog.
2/5) Tesamorelin is a growth hormone-releasing hormone (GHRH) analog.
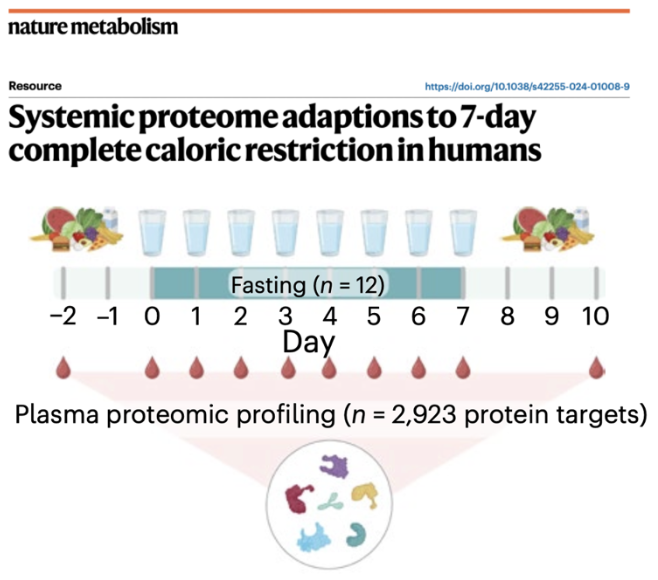 2/5) During the first two days, the body performed a fuel switch.
2/5) During the first two days, the body performed a fuel switch.
 2/5) Many studies and meta-analyses find: no cognitive harm, neutral effects, or even potential protection against dementia
2/5) Many studies and meta-analyses find: no cognitive harm, neutral effects, or even potential protection against dementia
 2/4) In a 2026 paper published in Cell Metabolism, researchers connected a compound found in aged garlic extract—called S1PC (1)—to this longevity pathway.
2/4) In a 2026 paper published in Cell Metabolism, researchers connected a compound found in aged garlic extract—called S1PC (1)—to this longevity pathway.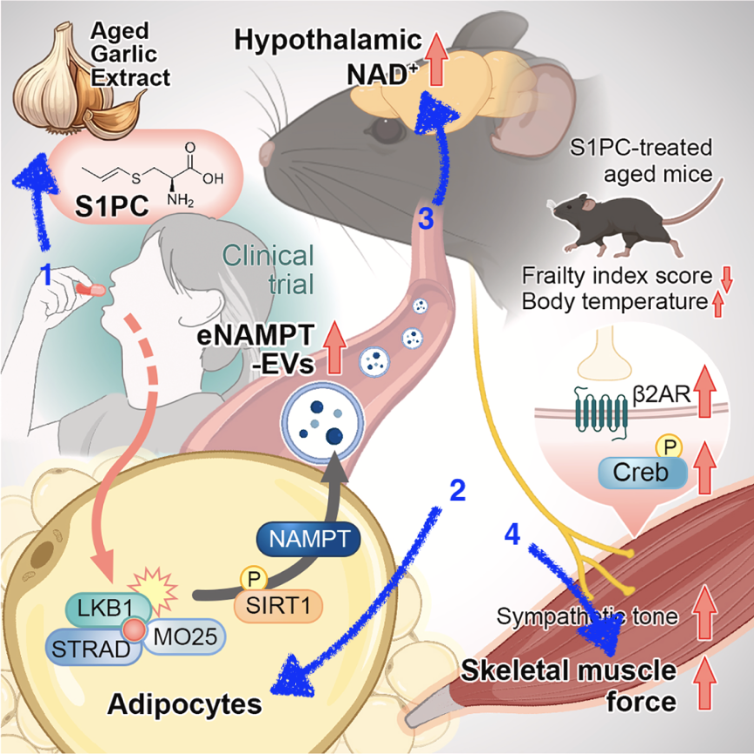
 2/6) The answer is the glymphatic system.
2/6) The answer is the glymphatic system.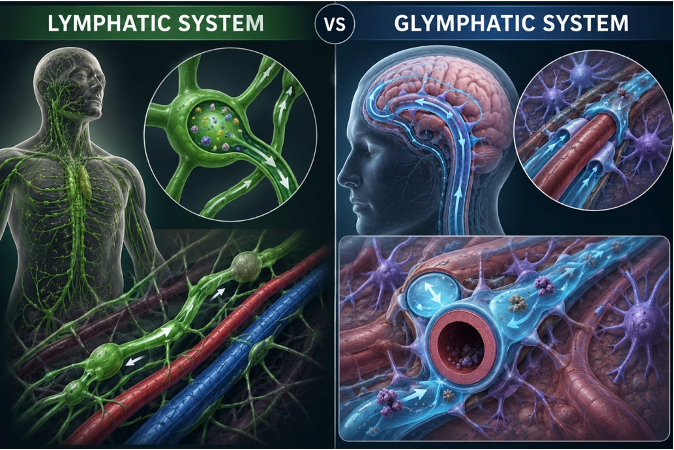
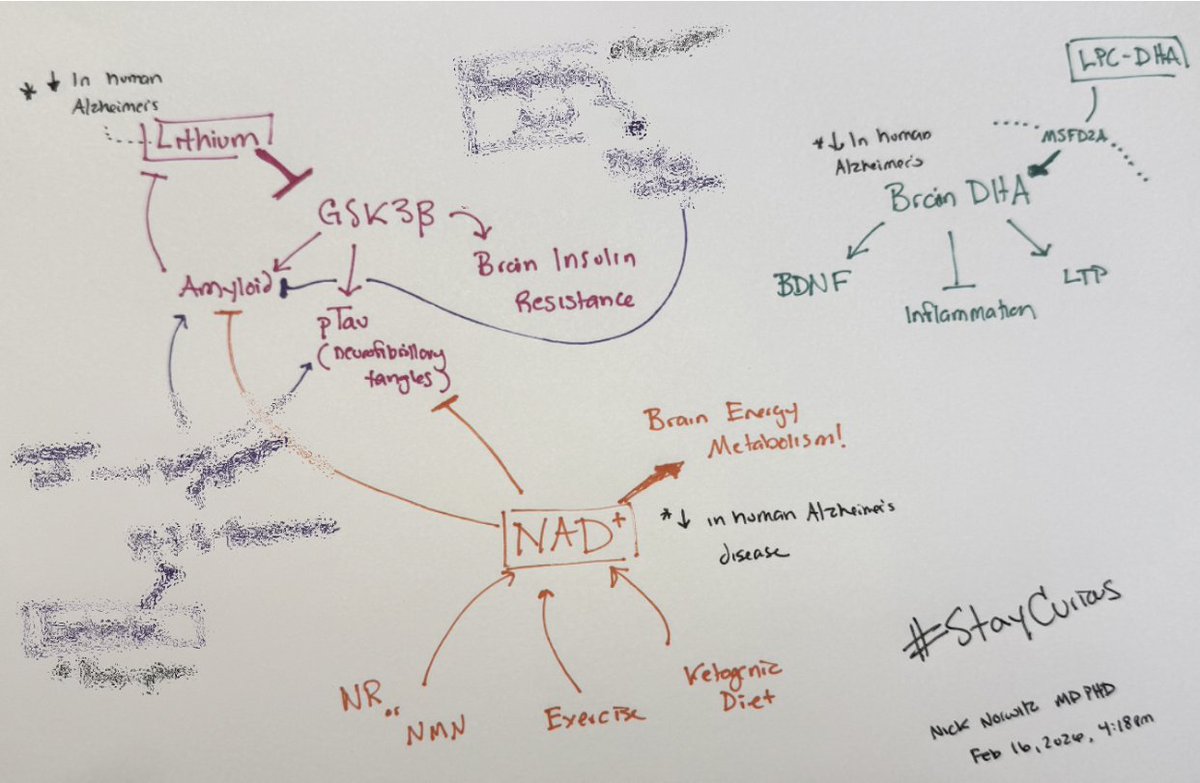 2/12) The first is lithium.
2/12) The first is lithium.
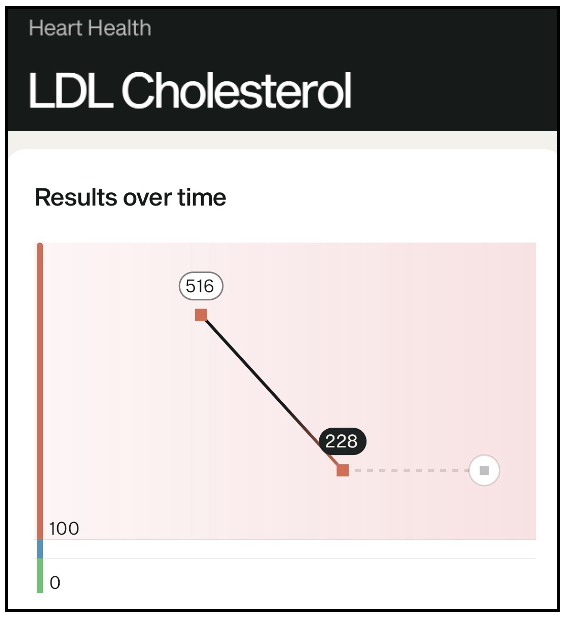
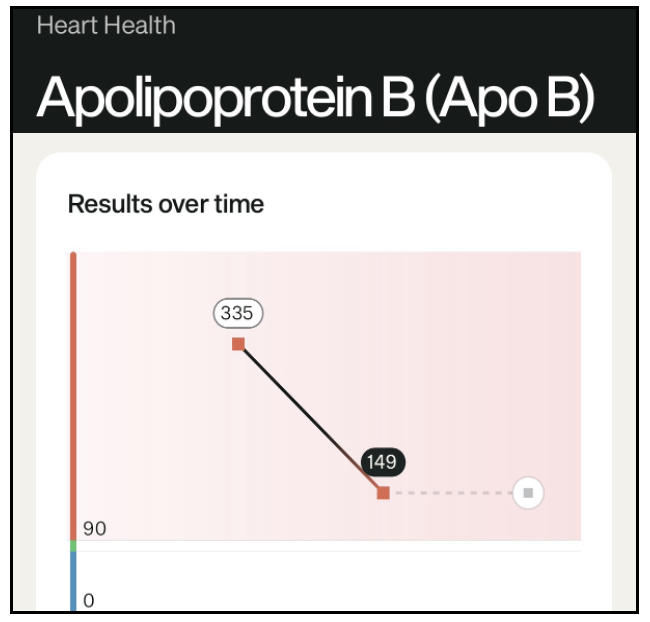
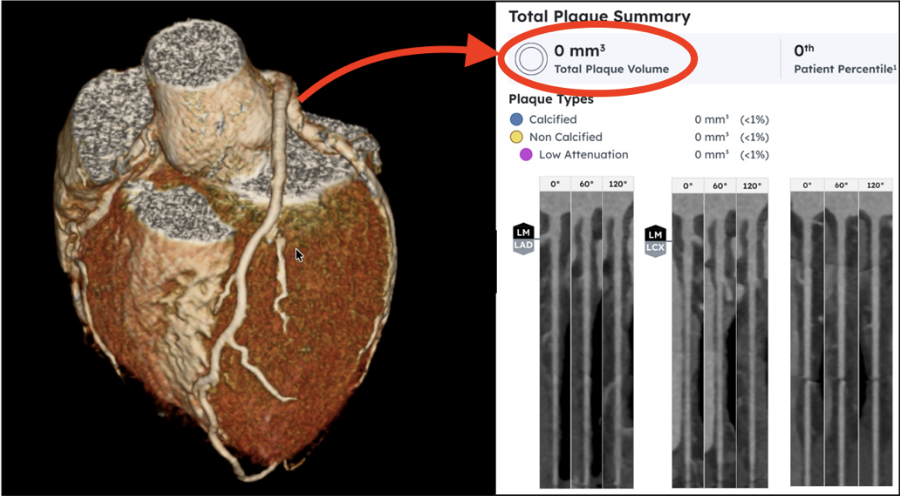 2/7) And although I'm young, at levels like mine, this is still stunning. The only historical comparator group are those with a 1-in-1,000,000 genetic condition: homozygous familial hypercholesterolemia (hoFH). Now, I don't have this hoFH. These children typically get severe advanced atherosclerosis and even a heart attack as young as age 8 or 10.
2/7) And although I'm young, at levels like mine, this is still stunning. The only historical comparator group are those with a 1-in-1,000,000 genetic condition: homozygous familial hypercholesterolemia (hoFH). Now, I don't have this hoFH. These children typically get severe advanced atherosclerosis and even a heart attack as young as age 8 or 10.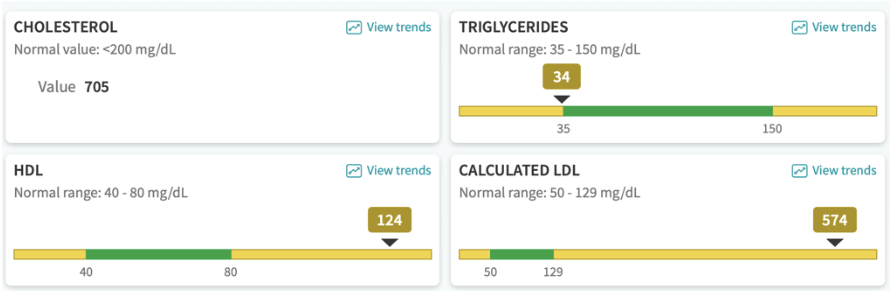
 2/6) Tesamorelin is an analog of growth hormone–releasing hormone, a hormone released by the brain that signals the pituitary to release growth hormone.
2/6) Tesamorelin is an analog of growth hormone–releasing hormone, a hormone released by the brain that signals the pituitary to release growth hormone.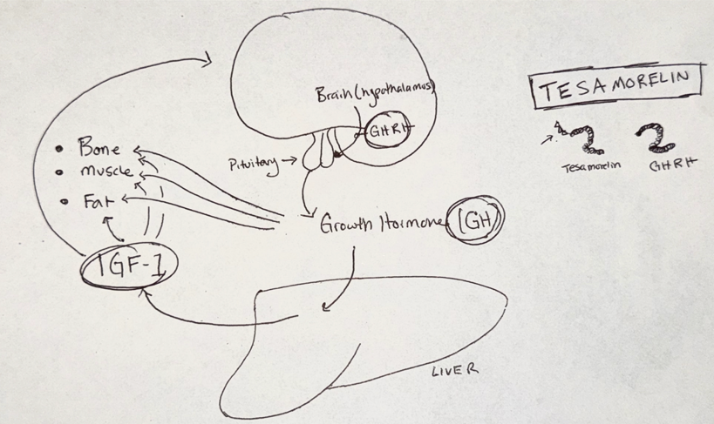
 2/7) Take ezetimibe. Beyond lowering LDL, evidence suggests it crosses into the brain and influences neurobiology.
2/7) Take ezetimibe. Beyond lowering LDL, evidence suggests it crosses into the brain and influences neurobiology. 2/5) Statins disrupt mitochondrial function.
2/5) Statins disrupt mitochondrial function.
 2/8) The most important fat for the brain is DHA, a long-chain omega-3 fatty acid.
2/8) The most important fat for the brain is DHA, a long-chain omega-3 fatty acid.
 2/8) It was new paper in a top journal turned confusion into clarity and left me in awe of how much we’re still uncovering about human physiology.
2/8) It was new paper in a top journal turned confusion into clarity and left me in awe of how much we’re still uncovering about human physiology.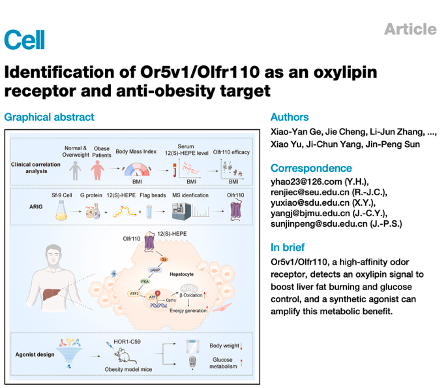
 2/5) More interestingly, one trial showed that while bergamot decreased small dense LDL, it increased‘large, fluffy’ LDL.
2/5) More interestingly, one trial showed that while bergamot decreased small dense LDL, it increased‘large, fluffy’ LDL.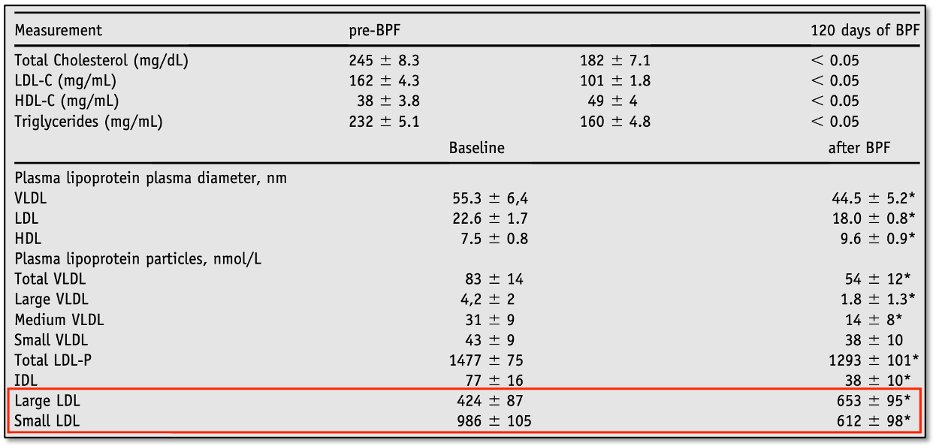
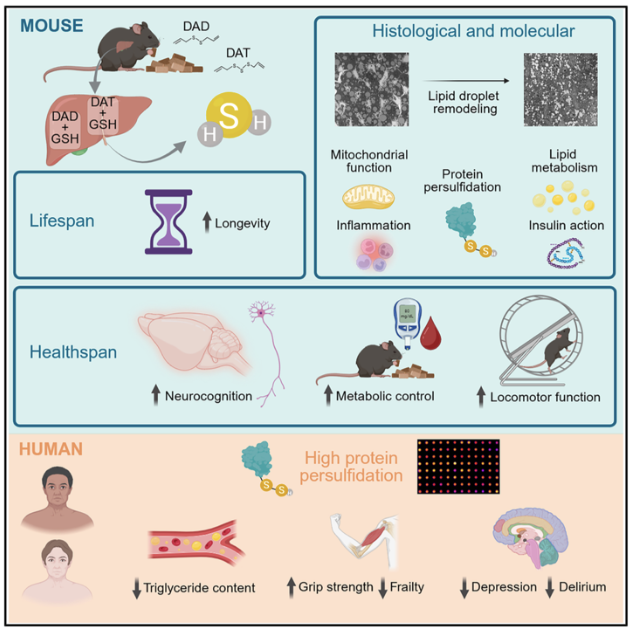 2/7) Garlic is rich in diallyl sulfides (DAS) — sulfur compounds that increase hydrogen sulfide (H₂S) levels. H₂S acts like a hormone: it diffuses through membranes, triggering cellular pathways across the body.
2/7) Garlic is rich in diallyl sulfides (DAS) — sulfur compounds that increase hydrogen sulfide (H₂S) levels. H₂S acts like a hormone: it diffuses through membranes, triggering cellular pathways across the body.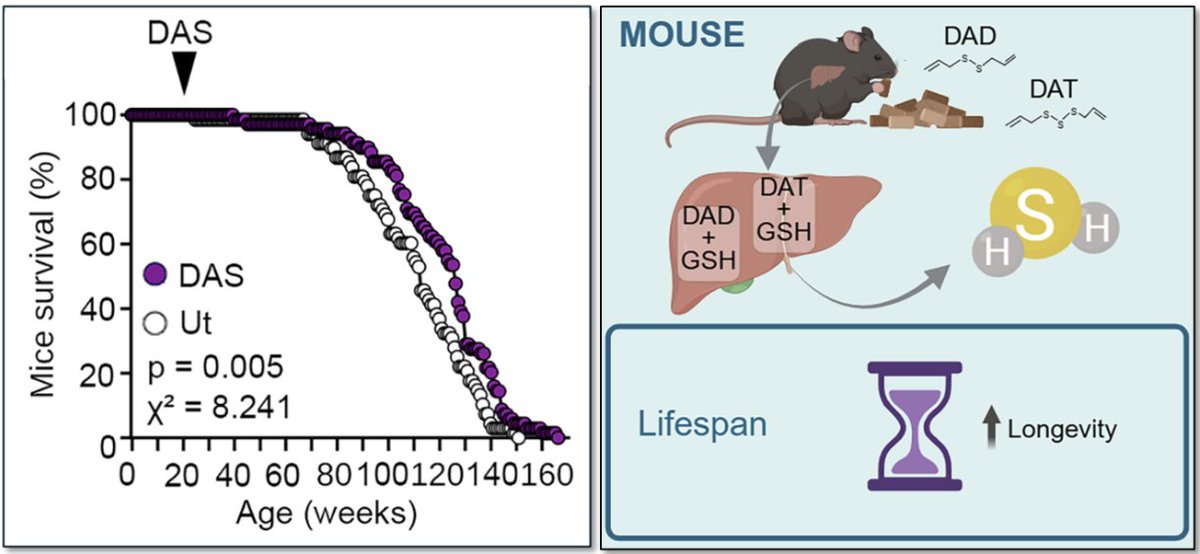
 2/5) To test for a causal connection between sleep deprivation and atherosclerosis (the buildup of plaque in arteries), researchers sleep-deprived mice genetically predisposed to developing atherosclerosis.
2/5) To test for a causal connection between sleep deprivation and atherosclerosis (the buildup of plaque in arteries), researchers sleep-deprived mice genetically predisposed to developing atherosclerosis.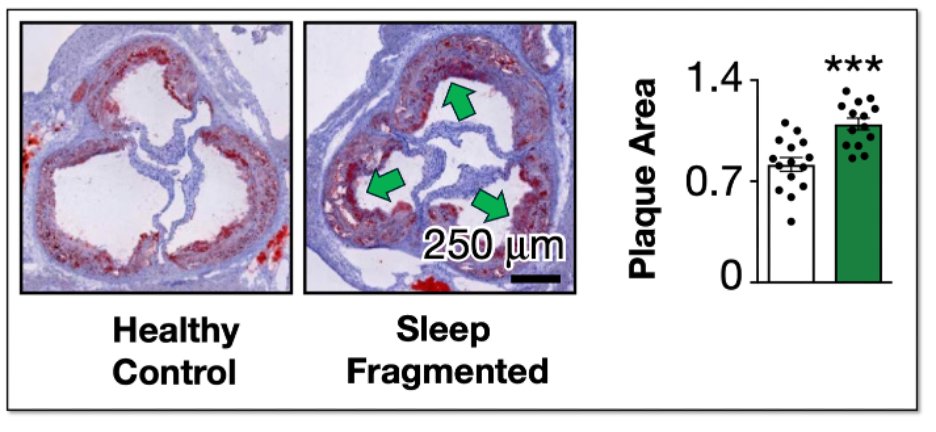

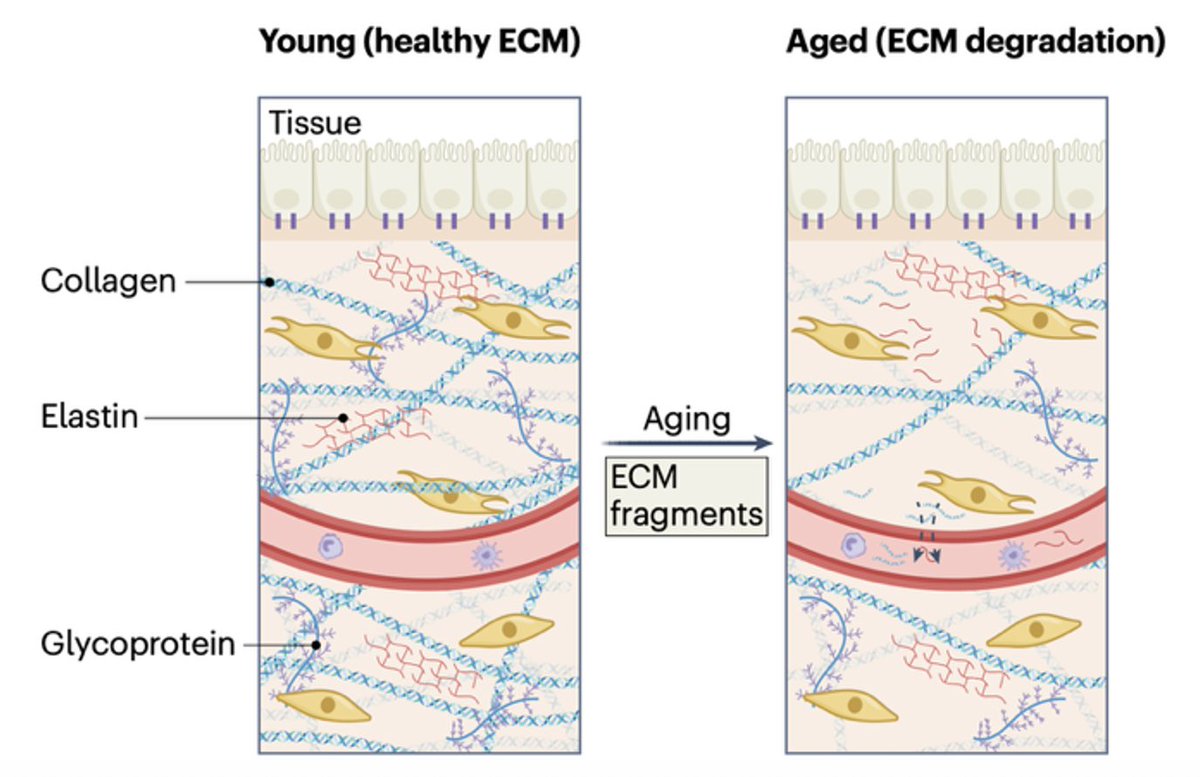
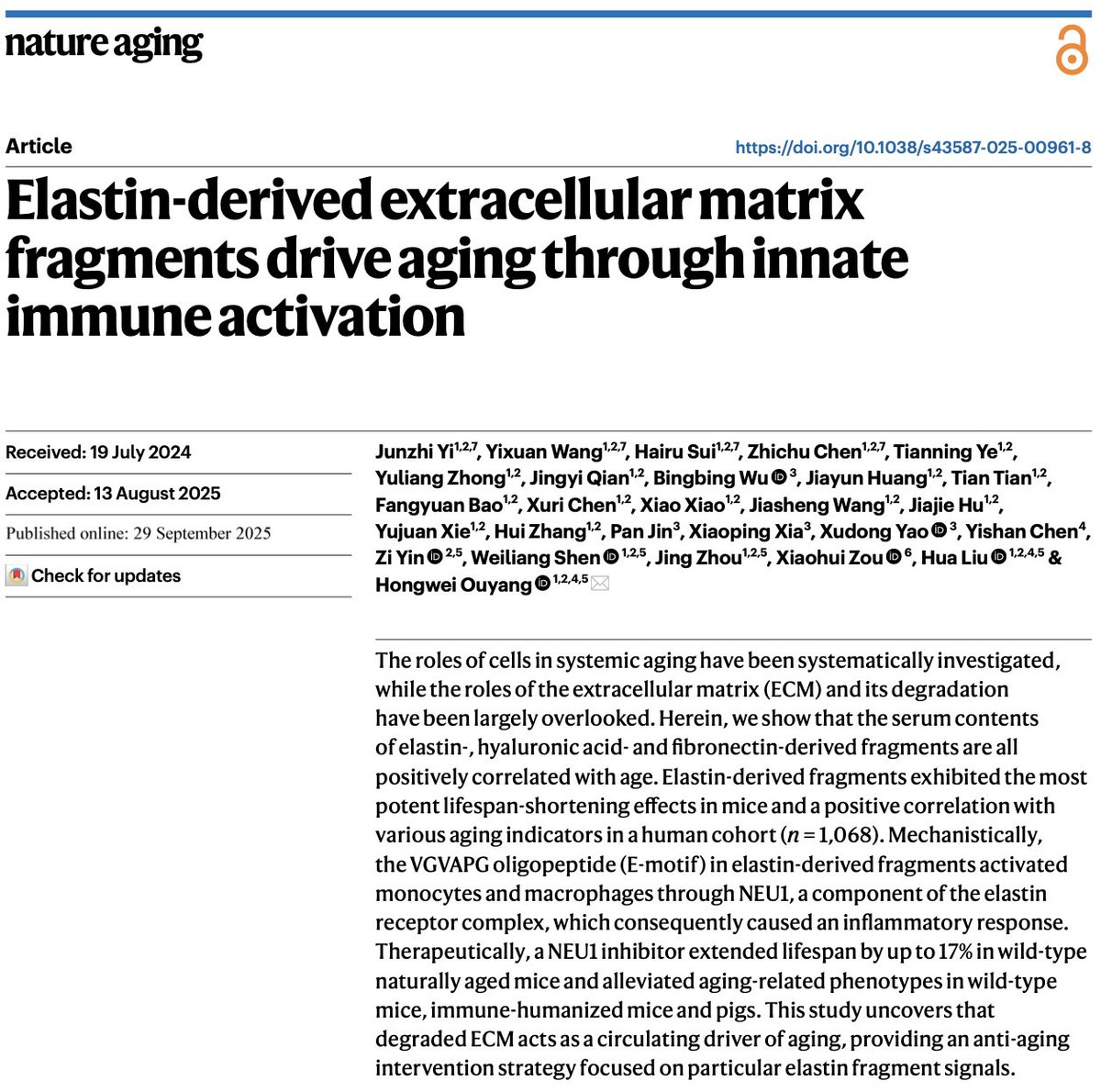 2/6) The scaffolding beneath your skin, made of collagen, elastin, and other proteins is called the “Extracellular Matrix” (ECM).
2/6) The scaffolding beneath your skin, made of collagen, elastin, and other proteins is called the “Extracellular Matrix” (ECM).